Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
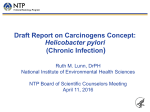
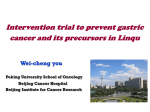
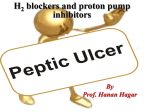
Grand Rounds 4/16/15 Ashish Sharma PGY-4 Gastroenterology Fellow Mentor- Maya Balakrishnan,MD Case presentation • 54 y/o Hispanic female was brought in by her family after recurrent falls. • She felt progressively feeling weak for at least 2 months. • She had persistent nausea/vomiting, post prandial fullness, inability to tolerate PO and a 30 lb. wt. loss over 2 months. Case presentation • She reported tingling sensation of fingers and tows, “felt funny on the bottom of foot”, “not able to feel pressure”, and “walked like a robot”. • She denied any hematochezia, hematemesis or melena. Case presentation • PMH/PSH - None • Family history – thyroid disorder and lupus in her daughters • Social history – works as a cleaner, denied ETOH/smoking/illicit drugs • Medications - None Case presentation - Exam • Vitals – Afebrile, P – 65, BP- 86/47, RR- 15, Pulse Ox – 99% on RA, BMI -22 • Exam – GEN: NAD HEENT: mild icterus, OP clear CV: RRR, soft systolic murmur CHEST: CTAB ABD: + BS, soft, mild periumbilical tenderness with no guarding or rebound, non distended EXT: No edema NEURO: Rhomberg positive, otherwise non focal and intact Case presentation - Labs • • • • • • • • • • • CBC - WBC 3; Hb 5.6; PLT 96; MCV 115 CMP – Chemo 8 normal, TB 4, DB 0.8, other LFTs normal Coagulation profile – normal; TSH - normal B12 – 187, Folate – 15, Ferritin – 434, Iron Sat – 37% Reticulocyte count – 1% (low) LDH – 3670 (high), Haptoglobin < 32 Coomb’s test - negative Homocysteine – 13.2 (ULN 10.7) Methylmalonic acid (MMA) – 35437( ULN 378) Intrinsic factor ab - Neg Parietal cell ab - 48.7 (ULN 24.9) Case presentation – Peripheral smear Macrocytosis, + tear drops, Dysmorphic RBC, + hypersegmented neutrophil, early granulocyte progenitors, + platelet (normal morphology) Case presentation - EGD Atrophic stomach body Normal stomach body Case Presentation - Pathology Atrophic stomach body Normal stomach body No H. pylori seen on immunohistochemical stains Case Presentation - Pathology Intestinal Metaplasia Synaptophysin staining Diagnosis • Pernicious Anemia - Pernicious anemia (PA) is a macrocytic anemia that is caused by vitamin B12 deficiency, as a result of intrinsic factor deficiency (which is caused by an autoimmune corpus restricted atrophic gastritis) Clinical Questions • Background- Epidemiology, clinical presentation and diagnosis of PA • Is there a relationship between H pylori and PA? • Gastric cancer in PA - Incidence & role of surveillance Epidemiology • PA is an uncommon disease • Primarily a disease of the Caucasians, however there are recent reports of occurrence in Blacks, Latin Americans and Asians • Incidence - 9 cases/100k per year; and about 0.13% of population is affected in high risk groups • Up to 1.9 % of persons > 60 years may have undiagnosed PA • F: M- 2:1 per older data, but newer data shows no difference in gender distribution Pedersen AB. Morbidity of pernicious anaemia. Incidence, prevalence, and treatment in a Danish county. Acta Med Scand 1969 Carmel R. Prevalence of undiagnosed pernicious anemia in the elderly. Arch Intern Med 1996 Clinical presentation • Mean age of presentation is 59-62 years • General symptoms - weakness, asthenia, decreased mental concentration, headache and with chest pain/palpitations in elderly. Edith Lahner. Pernicious anemia: New insights from a gastroenterological point of view. World J Gastroenterol 2009 Clinical presentation • GI symptoms – dyspepsia (up to 28% patients) • Neurological symptoms - paresthesia, unsteady gait, clumsiness, and in some cases, spasticity (up to 19% patients) • Association with other autoimmune disorders Edith Lahner. Pernicious anemia: New insights from a gastroenterological point of view. World J Gastroenterol 2009 Diagnostic algorithm Edith Lahner. Pernicious anemia: New insights from a gastroenterological point of view. World J Gastroenterol 2009 Clinical Questions • Background- Epidemiology, clinical presentation and diagnosis of PA • Is there a relationship between H pylori and PA? • Gastric cancer in PA - Incidence & role of surveillance PA and H pylori • PA was primarily understood as an autoimmune condition occurring in a genetically predisposed individual – clustering with other autoimmune conditions, presence of auto-antibodies, HLA- DR restriction • In recent years, H pylori (infectious etiology) is thought to be implicated in the pathogenesis of PA • Mechanism ? -Molecular mimicry between H+/K+-ATPase and H pylori antigens likely resulting in loss of immunological tolerance in a genetically predisposed individual Amedei A. Molecular mimicry between Helicobacter pylori antigens and H+, K+ --adenosine triphosphatase in human gastric autoimmunity. J Exp Med 2003 PA and H pylori Reasons for this association – - H pylori serology positive in upto 50% of PA patients - H pylori found in upto 30% of stomach biopsies of PA patients - PA (initially defined as corpus restricted atrophic gastritis), also involves antrum in upto 50% cases, with atrophic antrum gastritis seen in upto 30% cases - Serology positive for H pylori antigens - Cag A and Vac A Annibale B. CagA and VacA are immunoblot markers of past Helicobacter in upto 50% patients pylori infection in atrophic body gastritis. Helicobacter 2007 Fong TL. Helicobacter pylori infection in pernicious anemia: a prospective controlled study. Gastroenterology 1991 PA and H pylori Edith Lahner. Pernicious anemia: New insights from a gastroenterological point of view. World J Gastroenterol 2009 PA and H pylori • Therefore, pathogenesis of PA may be a autoimmune and/or infectious (H pylori related) PA and H pylori Importance of H pylori association with PA? - May be a prognostic factor in gastric neoplasia in PA - Study by Rugge et al. 4/562 PA confirmed patients had gastric neoplastic epithelial lesions (all were OLGA stage III or IV, and all had H pylori association). - 116/562 PA patients (9/10 PA patients treated for H pylori) studied prospectively with EGD/biopsy over a mean of 54 months developed NO gastric epithelial neoplasia. Rugge et al. Autoimmune gastritis: histology phenotype and OLGA staging. Aliment Pharmacol Ther 2012 Clinical Questions • Background- Epidemiology, clinical presentation and diagnosis of PA • Is there a relationship between H pylori and PA? • Gastric cancer in PA - Incidence & role of surveillance Gastric cancer and PA There is a 7 fold increase in RR of gastric cancer in PA patients Vannella et al. Systematic review: gastric cancer incidence in pernicious Anaemia. Aliment Pharmacol Ther 2013; Gastric cancer and PA - ASGE guidelines 2006 • ASGE states that risk for gastric cancer in PA patients in US population is low (about 1.2%, close to average population risk) • Recommends at least one EGD after diagnosis of PA (risk is highest within 1st yr of diagnosis) • Guidelines for gastric cancer surveillance in intestinal metaplasia/dysplasia should probably be applicable to PA patients as well ASGE guideline: the role of endoscopy in the surveillance of premalignant conditions of the upper GI tract GASTROINTESTINAL ENDOSCOPY Volume 63 Gastric cancer and PA • Given that there are no guidelines for surveillance, an individualized approach needs to be adopted. • In patients with gastric symptoms, pre-neoplastic lesions (on index EGD), age >50 yr at diagnosis, family h/o gastric cancer, high risk ethnicity (Asian/Hispanic) and H pylori associated PA may be considered for gastric cancer surveillance Back to our patient • Patient had remarkable improvement in her fatigue and asthenia with Vitamin B12 injections. Hb and B12 levels improved. LDH and MMA decreased, and reticulocyte index increased • Neurological symptoms did not reverse • Repeat EGD done with mapping biopsies in 3 months, showed extensive intestinal metaplasia. Will repeat EGD in 4 years with mapping biopsies for reasons mentioned before • Will monitor for iron deficiency • Will obtain H pylori IgG for prognostication Take home points • PA is an uncommon cause of anemia resulting from autoimmune atrophic body gastritis; presents in 5th or 6th decade of life, mostly commonly with general anemia symptoms • H pylori plays role in pathogenesis of PA via mechanism of molecular mimicry. This relationship may have prognostic significance for gastric neoplasia in PA • From the data shown, there is increased risk of gastric cancer in PA patients compared to average population. However there are no guidelines yet to support surveillance. Take home points • Per ASGE at least one EGD is warranted after diagnosis of PA (preferably within 1 yr), to screen for neoplastic or pre-neoplastic lesions. Thereafter, surveillance should be individualized. Thankyou!