Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
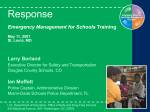
LSS Foster Care INCIDENT REPORT (When this form is being used, the Foster Care on-call staff or Supervisor MUST be notified by calling the crisis number.) Child’s Name: Date of Report: Date of Incident: Date of Birth: County: Male Female Foster Home: Time of Incident: AM PM Location of Incident: 1. Detailed Description of Incident: (Include who, when, what, where, how; Include what led up to the incident, the incident and follow up) 2. Summarize Prevention & Intervention Strategies Used Prior To and After Incident: (Strategies used to prevent incident and child’s reaction; describe efforts in increase supervision and resolve situation.) 3. Outcome and Response: (Describe outcome of incident, status of youth-child’s feelings, reactions, attitudes, behaviors observed, anger, rage, sullen, despondence, compliance, etc. If a physical intervention (i.e. physical escort or passive physical restraint) was initiated identify the SPECIFIC “dangerous” behavior that warranted the physical intervention) 4. Report of Physical Injuries: 5. Medical Attention Given: 6. Case Manager/On-call staff was called/involved No Yes If yes, who: 7. Contacts Made (The following contacts were authorized by a Supervisor/Case Manager/On- Call. Include name, date, and time) Law Enforcement Agency: Health Care Provider: Other: Required External Reports Neglect* Physical Abuse* Sexual Acting Out* Sexual Abuse* Suicidal Gestures* Reported Past Abuse* Runaway* Psychiatric Hospitalization* Medical Hospitalization* Emergency Medical Care* Victim of Assault High Risk Watch Potential Runaway Behavior* Potential Self Harm Behavior* Noncompliance Illegal Conduct Significant Disruption Physical Assault/Aggression* Verbal Aggression Dangerous Behavior* Threatening Behavior* Property Destruction* Inappropriate Sexual Comments Attempted Inappropriate Sexual Behavior* Actual Left Without Permission* Drug Possession/Use* Tobacco Related Weapon Possession* Gang Related Theft* Interfering in a Crisis* Medical Noncompliance Injury – Self Harm* Grooming - Sexual Injury – Accidental Grooming – Nonsexual Basic First Aid Power Thrusting/Intimidation Blood Borne Pathogen* Other Urine Feces Child Reported Incident* Blood Saliva Interventions Verbal Redirection 1:1 Processing Time Out Given Room Search Police Report Filed Child Physically Restrained 1. Danger to Self 2. Danger to Others 3. Restraint Length: *=May require external report Signature of Care Giver/TFC Staff Completing report: Date: Signature of Witness, if applicable: Date: ***************************************************************************************************** Child Review/Comment: This incident report is: accurate inaccurate. Other Comments: Signature of Child:____________________________________________________________ Report must be sent to LSS Case Manager within 24 hours of the incident. Rev. Feb 2017 Date:________________