Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
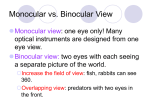
I. Definition of transient vision loss A. Abrupt and temporary loss of vision 1. Can be monocular or binocular 2. No etiology implied II. Assessment of the patient A. History 1. Is the vision loss monocular or binocular? a) Monocular implies disorder anterior to optic chiasm but can be systemic cause b) Binocular involves optic chiasm, tracts, radiations or visual cortex but can be systemic cause 2. How long did the vision loss last? a) Differential diagnosis can depend on duration (1) Migraine: 10 – 30 minutes (2) Papilledema: seconds 3. How would you describe the vision loss? 4. Are there any actions which can precipitate the vision loss? a) Posture changes? b) Postprandial? c) When reading? 5. Has there been more than one episode? 6. Do you experience any other symptoms at the time of the episode? a) Headache? b) Difficulty speaking? c) Difficulty walking? 7. History of medical conditions a) Hypertension b) Diabetes c) Hyperlipidemia B. Examination 1. Visual acuity 2. Visual fields 3. Funduscopy 4. Physical exam as appropriate a) Auscultate carotids b) Auscultate heart c) Cranial nerve evaluation III. Differential Diagnosis of Monocular Transient Vision Loss A. Gaze or reading evoked 1. Intraorbital mass most common cause a) Look for other signs like proptosis, conjunctival congestion, ONH edema b) Graves’ ophthalmopathy, tumors and trauma c) Neuroimaging if suspected B. Monocular vision loss lasting minutes to hours 1. General considerations a) Ischemia most common cause and increases risk of stroke b) Often associated with heart disease 2. Thromboembolic disease a) Aortic or carotid artery atherosclerosis (1) Cholesterol emboli (Hollenhorst plaques) (2) Ipsilateral vision loss and contralateral body symptoms (3) Increased risk of stroke b) Cardiogenic (1) Calcific emboli (2) Valvular disease (3) Atrial fibrillation 3. Ocular ischemic syndrome a) Carotid artery stenosis (1) Postprandial vascular steal or postural changes (2) Light induced amaurosis fugax (3) Ocular angina (4) Mid-peripheral retinal hemorrhages b) Increased risk of stroke 4. Impending retinal vein occlusion a) Variable length of vision loss b) Venous stasis c) Often associated with atherosclerosis, diabetes and hypertension 5. Giant cell arteritis a) b) c) d) e) Vasculitis Ask about scalp tenderness, jaw claudication, headache, weight loss, fatigue Check for decreased temporal artery pulse with tenderness Risk of permanent loss of vision or visual field including other eye Risk of death 6. Collagen vascular disease a) History of diseases like SLE, Sjögren’s, RA b) Skin lesions c) Joint dysfunction 7. Retinal Migraine a) b) c) d) May be associated with exercise Often in young patients May be preceded by premonitory symptoms Typically benign course but a diagnosis of exclusion 8. Coagulopathies a) Polycythemia (1) Increased blood viscosity and altered red blood cells (2) Tiredness, depression, vertigo, tinnitus (3) Associated with hypertension, angina, intermittent claudication b) Sickle cell disease (1) Genetic mutation changes hemoglobin so that the cells become more rigid and change shape (2) Decreases ability of RBC to pass through small vessels which decreases perfusion 9. Ocular causes a) b) c) d) Typical optic neuropathy – Uhthoff’s phenomenon Intermittent angle closure glaucoma Spontaneous hyphema Morning glory syndrome C. Monocular vision loss lasting seconds 1. Papilledema a) Whiting or graying out of vision b) Spontaneous or with changes in position c) Bilateral disc swelling 2. Optic nerve sheath meningiomas 3. Congenital optic nerve abnormalities a) ONH drusen b) Peripapillary staphyloma 4. Thromboembolic disease (usually longer duration) IV. Differential Diagnosis of Binocular Vision Loss A. Papilledema 1. Pseudotumor cerebri a) Intracranial hypertension without mass or infection b) Cause remains unproven in 90% of cases (idiopathic) and it is a diagnosis of exclusion c) More common in women d) Associated with many medications e) Headaches, decreased acuity, pulsatile tinnitus 2. Space occupying lesion B. Bilateral carotid disease C. Hypotension 1. Orthostatic a) Postural changes b) Lightheadedness 2. Cardiac failure a) Shortness of breath (orthopnea) b) Swelling of legs 3. Dehydration D. Migraine 1. Migraine with aura a) Usually unilateral headache with family history b) Caused by a complex cascade of neurological and vascular changes c) Can have precipitating factors and characteristic build up 2. Migraine aura without headache a) Binocular symptoms b) Longer duration than typical ischemia E. Collagen vascular disease F. Vertebrobasilar ischemia 1. Associated symptoms include vertigo, dysarthria, diplopia, gait disturbances 2. Visual field loss common (contralateral to lesion) G. Seizure 1. Uncommon cause 2. Visual loss can be ictal or post ictal 3. Blurred vision or white out 4. Associated visual field defect V. Diagnostic testing A. Any testing indicated by history results B. Erythrocyte sedimentation rate in any patient over 50 1. Westergren sedimentation rate a) Normal for men = age/2 b) Normal for women = (age+10)/2 2. C-reactive protein in any patient over 50 a) Value > 2.45 mg/dl considered elevated C. Temporal artery biopsy if suggestion of GCA D. Carotid duplex ultrasound in any patient over 50 or younger if vascular risk factors such as diabetes, hypertension or hyperlipidemia E. Cardiac evaluation including Holter monitoring and echocardiography F. ECG to rule out cardiac morbidity or mortality G. Brain MRI: especially if bilateral TVL and symptoms of vertebrobasilar ischemia or MS H. Hypercoagulable testing if history suggestive: (prior thrombosis, family history) I. If young with no other risk factors and symptoms are classic for migraine, may consider no testing J. Despite extensive work-up, some cases will be idiopathic VI. Reading References 1. Lee A, Brazis P. Transient Visual Loss . In: Clinical Pathways in Neuroophthalmology. Thieme Medical Publishers, New York, Stuttgart 1998. p. 135 – 150. 2. Kumar P, Clark M. Clinical Medicine 6th ed. Elsevier Limited 2005. Various chapters.