Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
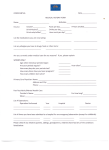
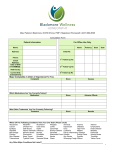
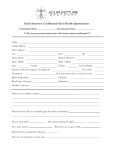
INTAKE FORM (CONFIDENTIAL) Borealis Naturopathic Health Center Ashley Guité B.A. D.H.M.H.S Reg. BIE Practitioner Date: ____________________ Name: _____________________________________________________________ (Surname) (Given Name) Date of Birth: DD/MM/YYYY ____________ Age: ______ □M □F Address: ___________________________________________________________ City: ____________________ Province: _________ Postal Code: ______________ Home Phone: ______________________ Work Phone: ______________________ Emergency Contact: _______________________ Phone: _____________________ Family Physician: ____________________________ Phone: __________________ E-mail Address: ______________________________________________________ Occupation: _________________________ Number of Children if any: __________ How were you referred? Physician Self Referral Other FOR FEMALE PATIENTS ONLY Age at First Menses: _______________ Number of Pregnancies: _______________ Every disease, drug or accident leaves its mark and remains a weak point in our system. Homeopathic treatment takes into account all of these details of the past and aims to strengthen the system. It is important to know about all the ailments you have suffered in the past as well as the treatments you have taken. What problem brings you to this appointment ________________________________________________ _____________________________________________________________________________________ When did the symptoms begin? ___________________________________________________________ Are your symptoms getting worse? Yes No. Please which of the following substances you are currently using: □ Alcohol □ Chewing Tobacco How Much? ______ □ Coffee How Much? ______ □ Recreational Drugs How Much? ______ How Much? ______ □ Cigarettes How Much? ______ □ Teas How Much? ______ In the list below ALL the major illnesses so far suffered (past & present): □ Allergy □ Ear Infections □ Luekaemia □ Ringworms □ Anemia □ Eczema □ Lumbar Puncture □ Scabies □ Appendicitis □ Food poisoning □ Major Bleeding □ Asthma □ Fungus □ Malaria □ Sexual Abuse □ Backache □ Gallbladder □ Malnutrition □ Sinusitis □ Boils □ German Measles □ Measles □ Small Pox □ Bronchitis □ Goiter □ Meningitis □ Cancer □ Gonorrhea □ Carbuncles □ Hay Fever □ Mumps □ Chicken Pox □ Headaches □ Numbness □ Cholera □ Head Injury □ Paralysis □ Cold Sores □ Spleen □ Mononucleosis □ Hepatitis □ Septic Tonsils □ Strep Throat □ Stroke □ Syphilis □ TB □ Pimples □ Typhoid □ Convulsions □ Herpes □ Pneumonia □ Ulcers □ Cramps □ HIV/Aids □ Polio □ Unconsciousness □ Diabetes □ Hypertension □ Prolapsed Uterus □ Urticaria □ Diarrhea □ Jaundice □ Prostate □ Venereal Warts □ Diphtheria □ Kidney/Urine □ Psoriasis □ Whooping Cough □ Dysentery □ Liver Disease □ Rheumatism □ Worms □ Other: _____________________________________________________________________________ _____________________________________________________________________________________ Any Serious: □ Depression □ Grief □ Disappointments □ Fright □ Mental Upset □ Shock □ Nervous Breakdown Please list any necessary information about the illnesses checked: Onset (can you trace the origin of your illness to any particular circumstance, accident, illness, or mental upset), medications used, duration, if you completely recovered, etc: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ When are your symptoms worse? Year Round January May September February June October Are symptoms better away from home? March July November Yes No. April August December If yes, when? _________________________ Please list any hospitalizations regardless of cause: ___________________________________________ _____________________________________________________________________________________ List any food allergies and reactions experienced: _____________________________________________ _____________________________________________________________________________________ List any drug allergies and reactions experienced (i.e. penicillin, aspirin, sulfa, latex, etc): _____________________________________________________________________________________ _____________________________________________________________________________________ Describe any reaction to insect stings: _____________________________________________________________________________________ Please list any major injuries you may have had in the past: ______________________________ _____________________________________________________________________________________ Please list any major surgeries you may have had in the past: ____________________________ _____________________________________________________________________________________ Are you currently taking ANY medications or supplements? Medication/Supplement For What? (mg) Dosage Frequency – Amount/Day Relationship Father Mother Paternal Grandfather Paternal Grandmother Maternal Grandfather Maternal Grandmother Sister(s) Brother(s) Age If deceased age at death Cause of Death Diseases