Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
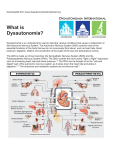
Complex Care Curriculum: DYSAUTONOMIA Facilitator Guide for Small Group Teaching Please allow 35 minutes for this session with an additional 10-15 minutes for discussion and questions Below is a slide-by-slide guide with suggested discussion points. The slides are equipped with animations that can be triggered when you see the word [click] in brackets. Before facilitating this session, please thoroughly review these slides and notes and practice triggering the animation. SLIDE Complex Care Curriculum DISCUSSION POINTS/NOTES Welcome to this discussion on Dysautonomia. DYSAUTONOMIA Dysautonomia Sonaly Rao McClymont, MD Sarah Helen Evans, MD Melanie Anspacher, MD Neha H. Shah, MD, MPH Complex Care Curriculum DYSAUTONOMIA Define dysautonomia in simple terms Identify risk factors Summarize basic pathophysiology Identify signs and symptoms Make the diagnosis Describe the consequences Make a basic treatment plan By the end of this learning module you should be able to: [click] Describe dysautonomia in simple terms [click] Identify patients at risk for developing dysautonomia [click] Have a basic understanding of the leading theories on pathophysiology [click] Identify signs and symptoms of dysautonomia [click] Make the diagnosis [click] Explain the consequences of untreated dysautonomia [click] Have a basic understanding of the most common medications used to treat dysautonomia, Make a preliminary management plan for it and be able to revise this plan over time with the help of a PM&R consultant Complex Care Curriculum DYSAUTONOMIA Metabolic Overdrive Dysautonomia is a syndrome characterized by episodes of autonomic nervous system “up-regulation” resulting in metabolic hyperdrive and increased muscle tone. It has also been described as a syndrome of simultaneous and paroxysmal sympathetic and muscle overactivity In simpler terms, dysautonomia can also be thought of as [click] “metabolic overdrive” or “brainstorming” [click] [click again to end] “BRAIN-STORMING” Complex Care Curriculum DYSAUTONOMIA Severe Brain Injury Traumatic Infectious Anoxic Metabolic Dysautonomia can occur in patients with old neurologic injury. Autoimmune Increased It should not be present in the patient with no Intracranial known neurologicIntracranial injury. Pressure Hemorrhage *Incidence after Traumatic Brain Injury is approximately 10% Complex Care Curriculum Spinal Cord Injury DYSAUTONOMIA Dysautonomia without Brain Injury Dysautonomia: TACHYCARDIA Autonomic Dysreflexia: BRADYCARDIA Spinal Cord Injury above T6 Autonomic Dysreflexia Who is at risk for dysautonomia? [click] Any patient with severe brain injury can develop dysautonomia. Types of neurologic injury may include: Traumatic, Anoxic, Acute increase in ICP, Infectious, Metabolic, Autoimmune, or Intracranial Hemorrhage. [click] Of note, incidence is approximtely 10% after Traumatic Brain Injury (TBI) [click] While any patient with a new brain injury is at risk, keep in mind that dysautonomia may also occur in patients with old neurologic injury without prior treatment for dysautonomia. [click] In addition, dysautonomia should not be present in a presumed neurologically normal patient, therefore, if sxs of dysautonomia persist in a person who is not known to have any neurologic deficits, then strongly consider neurologic imaging as part of the diagnostic evaluation. I’d like to take a quick moment to differentiate between brain injury and spinal cord inury [click] Patients with spinal cord injury (SCI) without brain injury will [click] NOT have dysautonomia [click] If the SCI is above the level of T6 a patient can have [click] Autonomic Dysreflexia in which there is excessive sympathetic outflow from the splanchnic plexus in response to noxious stimuli. Autonomic Dysreflexia will manifest clinically with similar symptoms and signs as dysautonomia (such as increased blood pressure, facial flushing, and sweating), however [click], Autonomic Dysreflexia is generally associated with BRADYCARDIA (due to intact parasympathetic inhibitory baroreceptor reflexes mediated by the vagal nerve) Complex Care Curriculum Disconnection Theory Cerebral Damage DYSAUTONOMIA D Y S A U T O N O M I A Excitatory:Inhibitory Ratio Model Damage to Central Inhibition Cortex↔Hypothalamus x Excessive Autonomic Reactions Autonomic Hyperactivity Complex Care Curriculum Complex Care Curriculum DYSAUTONOMIA DYSAUTONOMIA Heart Rate Respiratory Rate Agitation SYMPTOMS Sweating Blood Pressure DysautonomiaTemperature causes hyperthermia, NOT temperature instability There is a limited understanding of the pathophysiology of dysautonomia. It was originally thought to have an epileptogenic cause however EEGs did not consistently demonstrate epileptiform activity and anticonvulsant drugs failed to treat the symptoms. Currently, [click] The Disconnection Theory and [click]the Excitatory:Inhibitory Ratio Model are the leading theories on pathophysiology. [click] The Disconnection theory states that [click] diffuse or focal cerebral damage affects the [click] functional interaction between the cortex and hypothalamus [click] causing autonomic hyperactivity [click] The Excitatory:Inhibitory Ratio Theory states that [click] damage to the central inhibitory structures and pathways which regulate afferent information cause [click] excessive autonomic reactions to painful or even normal stimuli In simpler terms – in patients with dysautonomia [click] the control mechanism or regulation of the autonomic nervous system is [click] broken. The lack of feedback inhibition causes the ANS to act like a “Runaway Train.” Can you name the 6 most common symptoms associated with a dysautonomic storm? [click] Tachycardia, [click] Tachypnea, [click] Hypertension, [click] Hyperthermia, [click] Diaphoresis, [click] and Marked Agitation. Additional symptoms include posturing (decerebrate or decorticate), spasticity and dystonia. -When assessing blood pressure with a manual or automatic cuff, keep in mind that if a patient has increased tone associated with his/her episodes, it makes the blood pressure reading difficult to interpret - the reading is most likely partially real and partially mechanical. A reading from an arterial line, however, should be reliable. -Also, remember to rely only on central temperatures when assessing for hyperthermia. [click] Make note that dysautonomia classically does not include temperature instability – it is usually limited to hyperthermia. Complex Care Curriculum DYSAUTONOMIA Differential Diagnosis for Dysautonomia Diagnosis Infection High Pain of Dehydration Index of Drug fever ExclusionHeart Suspicion disease Rhabdomyolysis Narcotic withdrawal Complex Care Curriculum DYSAUTONOMIA Random Noxious Stimuli Constellation Complex Care Curriculum DYSAUTONOMIA Duration Risks Cost$ In this section, I will discuss how to make the diagnosis of dysautonomia. [click] The 2 main points to remember are that dysautonomia is a diagnosis of exclusion and it requires a high index of suspicion. As such, you must always rule out other causes of these symptoms. [click] [click] The differential diagnosis should be tailored to your patient’s individual circumstances; however the following diagnoses could masquerade as dysautonomia in an at risk patient: Infection, Pain, Dehydration, Drug fever, Heart disease, Rhabdomyolysis, and Narcotic Withdrawal When the work-up for other causes of your patients symptoms is negative, you must have a high index of suspicion to ultimately diagnose and treat for dysautonomia. Here are some clues that may help point you in the right direction: [click] There is a random pattern or timing to the onset of symptoms [click] The symptoms occur in response to noxious stimuli. Keep in mind that the stimuli that trigger autonomic storms may seem to be normal to the care providers however to the brain-injured patient they can be noxious (for example, loud noises, constipation, or full bladder). [click] Dysautonomic storms occur as a constellation of symptoms. Keep in mind that if the patient is already on medications that control some symptoms you may not see the entire constellation. For example a patient on a beta blocker may not have tachycardia associated with their storms. Consequences of dysautonomia are associated with sympathetic overdrive [click] such as increased energy expenditure and decreased feeding tolerance. If left untreated, it can lead to [click] longer duration of posttraumatic amnesia, mechanical ventilation, and coma. The longer the duration of symptoms, the increase in [click] risk for secondary brain injury, nosocomial infections, spasticity , dislocation of joints, fractures, development of heterotopic ossification, and overall worse outcomes. [click] All of these things translate into prolonged hospitalization and greater overall healthcare cost. Unfortunately, there is often a cyclical pattern associated with untreated dysautonomia as the consequences are frequently perceived as noxious to the patient resulting in an increase in dysautonomic storms. Complex Care Curriculum DYSAUTONOMIA Complex Care Curriculum DYSAUTONOMIA Decrease External Stimulation Complex Care Curriculum DYSAUTONOMIA Bowel and Bladder Musculo- FEN/GI Remove Noxious Stimuli Respiratory skeletal DERM Because dysautonomia is a hyperadrenergic state, associated with elevation of catecholamine levels, the goals of treatment are to [click] decrease sympathetic outflow and to [click] enhance the parasympathetic system with both [click] nonpharmacologic and pharmacologic methods. Nonpharmacologic treatment includes [click] decreasing external stimulation for your patient. What makes a comfortable environment will vary from patient to patient and it may take time to recognize what calms or triggers a patient. [click] For example if a patient is out of bed and becomes symptomatic you may try putting him/her back in bed, however if a patient is laying supine you may try different positioning. Try to create a calm and quiet environment for your patient by [click] dimming the lights, [click] decreasing the noise level, and limiting the number of visitors. [click] Allow your patient plenty of rest and sleep. [click] Holding or swaddling the patient can also help. Nonpharmacologic treatment also includes [click] avoiding noxious internal stimuli that may trigger an autonomic storm. These triggers may include [click] Constipation, full bladder, kinked foley catheter, urinary tract infection [click] Fracture, heterotropic ossification, splints that are too tight or have been on too long [click] Pressure ulcers, IV site irritation, fingernails or toenails that are too long [click] Mucus plugs, increased secretions, inappropriate ventilator settings [click] Cold feeds, Gastroesophageal reflux, or dehydration It is important to educate the entire care team about potential triggers for dysautonomia so that action can be taken as soon as possible to relieve the noxious stimulus. I will now move on to discuss pharmacologic treatment options. Complex Care Curriculum DYSAUTONOMIA First-line Agents • Benzodiazepines • Dopamine Agonists • Beta Antagonists Second-line Agents • Alpha Agonists • GABA B Agonists • Calcium Channel Modulators • Opiate Agonist Complex Care Curriculum DYSAUTONOMIA Benzodiazepines: Diazepam ACUTE management Spinal cord AND Brain Not for LONG TERM Tolerance, Resp depression [click] There are many types of medications that have been shown to help manage dysautonomia and we will review these individually over the next few slides. Keep in mind that all drug classes will cause cognitive impairment. In addition most of the drugs will have the additional effect of helping with tone. [click] In the following slides pay particular attention to Diazepam, which is an excellent choice for acute mgmt, as well as Bromocriptine and Propanolol which are the top choices for longer term management. [click] Second line agents can also be used in combination with first line agents to enhance treatment effect. [click] Of the benzodiazepines, diazepam works very well and works quickly, making it the best choice for acute management. [click] It acts both in the spinal cord AND the brain. [click] Some of the cons of Diazepam include that it is not suitable for longterm management of dysautonomia and there is rapid development of tolerance. Due to the way in which it is metabolized, there is an additive effect and thus a risk of respiratory depression. Complex Care Curriculum DYSAUTONOMIA Acute Management of Dysautonomia with Diazepam Established on Benzodiazepine? YES Complex Care Curriculum NO Extra PRN dose Use starting dose Increase frequency Can repeat x 1 Increase dose WARNING: RESP DEPRESSION DYSAUTONOMIA Benzodiazepines: Clonazepam Spinal cord AND Brain LONGTERM management Watch for seizures when weaning… Tolerance Cognitive Suppression As stated, Diazepam is the best choice for acute management of an autonomic storm. To determine dosage the practitioner must first [click] determine if the patient is on a benzodiazepine at baseline. [click] If already on a BZD, then consider these options: [click] Give an extra prn dose of that BZD which is the same amount as the scheduled dose, [click] Increase frequency of dosing, or [click] Increase the dose itself If your patient has not yet been treated for dysautonomia and is already on a BZD, it is most likely for management of a seizure disorder or a narcotic wean. If this established BZD does not appear to be controlling the new onset of dysautonomia, consider switching from the established BZD to Diazepam until the Dysautonomia is under better control. [click] If your patient is NOT already on a benzodiazepine then [click] Use Diazepam at the starting dose in the formulary; [click] If no results after 30 minutes you may repeat the dose once. [click] Remember, If you increase the dose too rapidly, give frequent PRN doses, or start with too high a dose the active metabolite will eventually build up and cause [click] respiratory depression. Also, when you are trying to adjust doses, keep in mind that parents, if available and involved, can be very helpful in knowing the background of what works for the patient. Finally, remember to take vital signs more frequently when assessing for response to new doses. [click] If a patient responds to acute management with Diazepam you may transition to Clonazepam for better long term management. [click] Like Diazepam, it also acts in the spinal cord AND brain. [click] While tolerance and cognitive suppression are side effects of clonazepam, it causes the slowest progression to tolerance of all the benzodiazepines and it is less cognitive suppressive compared to diazepam. [click] KEY POINT: When weaning clonazepam monitor closely for seizures which may occur due to unmasking of an underlying seizure disorder OR simply weaning too quickly Complex Care Curriculum DYSAUTONOMIA Dopamine agonists: Bromocriptine 1st line Acts centrally Least cognitive suppression [click] Bromocriptine, a dopmaine agonist, is thought to be effective for treating dysautonomia by regulating neuronal excitability. Dopamine is an inhibitory neurotransmitter that is thought to help regulate the autonomic nervous system which is in a state of chaos in patients with dysautonomia. [click] It is considered first line treatment for longterm management. It acts centrally and has the least cognitive suppressive effects of all the medications used to treat dysautonomia. [click] The main side effect to watch for is hypotension. Hypotension Complex Care Curriculum DYSAUTONOMIA Beta-antagonists: Propranolol 1st choice if Hypertension sympathetic overdrive Penetrates blood-brain barrier Albuterol can be used to counteract side effects of Propranolol acutely Bradycardia Secondary Hypotension Complex Care Curriculum DYSAUTONOMIA Beta antagonists: Labetalol Intravenous formulation Hypotension $$$ [click] Of the beta-antagonists, Propanolol is the [click] 1st choice for patients with prominent HYPERTENSION. It minimizes sympathetic overdrive by decreasing circulating catecholamines, reducing cardiac work and reducing catabolic drive. It also penetrates the Blood Brain Barrier and is therefore thought to act centrally as well. [click] Side Effects include : Bradycardia and Secondary Hypotension. KEY POINT: If your patient is experiencing bradycardia or hypotension secondary to an increased dose of propanolol then consider giving albuterol [click], a beta agonist, to counteract this beta blocker. Also, if a patient requires Propanolol at baseline for dysautonomia and also requires Albuterol for pulmonary disease – consider switching to Xopenex for pulmonary disease to improve the efficacy of propanolol on the heart. [click] Labetolol, another beta antagonist, while less commonly used for dysautonomia, [click] is an excellent choice for the patient who is NPO because it is available in an IV formulation. [click] The most notable side effect is hypotension. Due to differences in mechanism of action, one must monitor blood pressure more closely than you would with propanolol. In addition, it is significantly more expensive than propanolol. Complex Care Curriculum DYSAUTONOMIA Alpha agonists: Clonidine Transdermal patch available Acts at spinal cord AND brain Rapid onset of action - oral Cognitive suppression Hypotension Complex Care Curriculum DYSAUTONOMIA Calcium Channel Modulators: Gabapentin [click] Of the alpha agonists, Clonidine is the most commonly used medication for treatment of dysautonomia, often used [click] transdermally in a patch formulation. It acts at the spinal cord and brain and has the added benefit of rapid onset of action when given orally so can be used in acute situations or in patients who are already on multiple drugs. [click] Clonidine is not good for cognitive recovery in patients with neurologic injury. In addition it can cause hypotension and requires careful monitoring of blood pressure. Once your patient is stabilized, wean off Clonidine as soon as able to limit further cognitive suppression. [click] The calcium channel modulators are less efficacious medications for treating dysautonomia. [click] Gabapentin, while helping to regulate dysautonomia, can also manage tone and neuropathic pain. In addition, it has a relatively safe profile. [click] The major side effect is sleepiness that is dose-dependent and resolves with time. Can also manage tone and neuropathic pain Sleepiness Complex Care Curriculum DYSAUTONOMIA Calcium Channel Modulators: Dantrolene No affect on seizure threshold No cognitive suppression Treats hypertonia Severe hepatotoxicity [click] Dantrolene is another calcium channel modulator that can be part of a management plan for dysautonomia. [click] Benefits include the fact that it does not affect seizure threshold, it does not cause cognitive suppression, and it is effective treatment for hypertonia. [click] However the severity of the potential side effects, mainly hepatotoxicity, are worth considering. There is a black box warning associated with the use of dantrolene secondary to the risk of fatal chemical hepatitis. For most patients it is dose related. Careful monitoring of the liver enzymes may preclude this serious side effect. Complex Care Curriculum DYSAUTONOMIA GABA B Agonists: Baclofen Useful in patients with spasticity Acts in Spinal Cord in Brain if given orally Abrupt AND withdrawal can lead to seizures and rhabdomyolysis Sleepiness initially Lowers seizure threshold Complex Care Curriculum DYSAUTONOMIA Opiate Agonists: Morphine, Methadone Used to treat pain Suppresses sympathetic outflow Opiate wean can unmask dysautonomia, which can look similar to opiate withdrawal Sedation Respiratory depression Limit rehab potential Complex Care Curriculum MOST DYSAUTONOMIA Morphine, Methadone Clonidine Diazepam, Clonazepam Propranolol, Labetalol Baclofen LEAST Gabapentin, Dantrolene Bromocriptine [click] Baclofen, a GABA B Agonist, is not used in first line treatment for dysautonomia. [click] It is however a 1st line treatment for spasticity and often has the helpful side effect of decreasing sxs of dysautonomia. It acts primarily in spinal cord, but oral formulation may act on the brain as well. [click] Side Effects include sleepiness when initiating which usually resolves after a few days and lowering of the seizure threshold. [click] KEY POINT: Very rapid withdrawal can cause seizures and rhabdomyolysis; this is usually only seen with intrathecal baclofen withdrawal. [click] Similarly, Opiates like morphine and methadone, are not used in first line treatment for dysautonomia. [click] They are used to treat pain and have the helpful side effect of easing the symptoms of dysautonomia. Specifically, the opiates modify the extremes of autonomic nervous system changes and dystonic posturing while suppressing sympathetic outflow. [click] Unfortunately, opiates “turn off” the whole system due to sedative effects which makes rehabilitation therapies very difficult. KEY POINT: Many brain injured patients will require an opiate and/or benzodiazepine wean after prolonged sedation (for example after prolonged intubation in the intensive care unit). [click] Keep in mind that what may appear to be symptoms of withdrawal could actually be the unmasking of dysautonomia, particularly if the patient is on a slow wean. If this is suspected, consider adding another medication that treats dysautonomia while continuing to wean the other medications. Because most drugs used to treat dysautonomia have cognitive suppressive side effects and because dysautonomia should improve over time with recovery from the brain injury, careful attention should be paid to the potential for weaning these medications. Wean the medications that cause the [click] most cognitive suppression first and continue to wean all medications as tolerated. Complex Care Curriculum DYSAUTONOMIA TIPS: Multiple categories Consider sleep habits Complex Care Curriculum DYSAUTONOMIA Do you think this is dysautonomia? I tried bromocriptine, what else can I try? [click] Aggressive early management with medications from multiple categories will aid in preventing secondary brain injury and further consequences of uncontrolled dysautonomia as discussed earlier. Once a patient is controlled you can slowly wean off medications as tolerated [click] When considering dosing schedule remember that patients should not be storming when asleep --If your patient is sleeping well, dosing can be during the daytime (BID, TID, QID) --If not sleeping well then give around the clock dosing (q12, q8, q6) Pediatric physical medicine and rehabilitation physicians specialize in managing patients with dysautonomia. Call them early for expert help when you suspect dysautonomia and need help managing it. As a hospitalist, you can start and titrate meds on your own based on your comfort level, but always call PM&R for assistance when needed. Be sure to have vital signs and patterns to report. How soon can I titrate the dose? Complex Care Curriculum DYSAUTONOMIA In this final section, I will summarize the key points presented in this module. [click] Dysautonomia occurs when the control mechanism or regulation of the autonomic nervous system is broken resulting in [click] metabolic overdrive. Any patient with brain injury is at risk. HR RR BP Temp Sweating Agitation [click] The most prominent symptoms are tachycardia, tachypnea, hypertension, hyperthermia, diaphoresis, agitation—they occur together as a constellation of symptoms. Complex Care Curriculum DYSAUTONOMIA Diagnosis of Exclusion High Index of Suspicion Non-pharmacologic Pharmacologic • Decrease external stimulation • Remove internal noxious stimuli • Diazepam Acute • Propranolol and BromocriptineChronic Complex Care Curriculum DYSAUTONOMIA [click] Remember that dysautonomia is a diagnosis of exclusion and requires a high index of suspicion. [click] Treatment is both nonpharmacologic and pharmacologic. Diazepam is the best choice for acute management. Propanolol and Bromocriptine are the best choices for long term management. [click] Remember, difficult cases may require medications from multiple categories. [click] When the patient is stabilized, always wean off the most cognitive suppressive medications first. [click] Finally, call your friendly neighborhood pediatric physiatrist early! And always have vital signs and patterns to report. Wean meds based on cognitive supression Complex Care Curriculum DYSAUTONOMIA Baguley IJ, Heriseanu RE, Cameron ID, Nott MT, SlewaYounan S: A Critical Review of the Pathophysiology of Dysautonomia Following Traumatic Brain Injury. Neurocrit Care 2008; 8(2):293-300. Baguley IJ, Cameron ID, Green AM, Slewa-Younan S, Marosszeky JE, Gurka JA: Pharmacological management of Dysautonomia following traumatic brain injury. Brain Inj 2004 May; 18(5):409-17. Hendricks HT, Heeren AH, Vos PE.: Dysautonomia after severe traumatic brain injury. Eur J Neurol 2010 Sep;17(9):1172-7. Taketomo, Carol K, Jane H Hodding, and Donna M Kraus. Pediatric Dosing Handbook. Hudson: Lexi-Comp, 2010. Print. To generate audience discussion consider using the following reflective questions: Have you ever take care of a patient with dysautonomia? -Describe that experience. -Describe your management of that patient. What can you take away from this session that will change your management of dysautonomia in the future?