Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Heart failure wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Electrocardiography wikipedia , lookup
Rheumatic fever wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Congenital heart defect wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Evaluation for Congenital Heart
Diseases
Seoul National University Hospital
Department of Thoracic & Cardiovascular Surgery
Heart Diseases in Children
Congenital heart diseases
Rheumatic heart disease : Rheumatic fever
Other acquired diseases: Kawasaki
Cardiomyopathy
Arrhythmia
Effects of CHD
• No effect on a child
• Decreased function when stressed
• Decreased cardiopulmonary function
• Other organ/system manifestation
Presentation of CHD
•
•
•
•
•
Shock like symptoms
Cyanosis
Congestive symptoms
Exercise intolerance
Asymptomatic heart murmur
•
•
•
•
Abnormality in routine chest PA
Chest pain
Syncope/ seizure/ fainting
Airway obstruction/ dysphagia
Shock like Symptoms
• Non-specific: collapse, pallor, cold clammy
skin, hypotension, oligouria, acidosis
• HLHS, critical AS, IAA, COA unable
to maintain systemic output during transitional
circulation
• Most common in neonate / infancy
• Very important to recognize
Cyanosis
• Cyanosis: more than 5.0g% of reduced Hb.
• Central versus Peripheral cyanosis
• Central cyanosis: CNS, heart, lung
• Pathophysiology: TGA, TOF, CML, DDPC
Congestion
• Symptoms: dyspnea on feeding, sweating,
poor weight gain, frequent respiratory infection
• Most common mode in infancy
• Obligatory shunt lesions/ Left to right
shunt lesions/ CML with no PS/
Myocarditis/ Arrhythmia
Asymptomatic Murmur
• Heart murmur noted in routine examination
• ASD, VSD, PS, AS, Bicuspid AV
• Common mode in childhood
• Murmur does not mean there is a CHD
• No murmur does not mean there is no CHD
Abnormality in Chest PA
Corrected TGA/ Pericardial Defect/ Cardiac Tumor
Chest Pain
* Anomalous origin of left coronary artery from pulmonary artery
* Aortic stenosis(severe) / Hypertrophic cardiomyopathy
Syncope/ Seizure/ Fainting
• Anoxic spell of acyanotic TOF
• Arrhythmia : VT, SVT, long QT syndrome
• Syncope on exercise : AS, SAS, IHSS
Airway Obstruction/ Dysphagia
Airway Obstruction / Dysphagia
Abnormal PA Branching
Mode of / Age at Presentation
• Collapse
: within 3-4 days
• Cyanosis
: usually within a month
• Congestion : 1-5 months
• Murmur
: any time
Diagnosis of Cardiac Diseases
• Anatomic Diagnosis
• Hemodynamic Evaluation
• Total assessment / Prognosis
• Etiologic Diagnosis
Diagnostic Tools
• History and physical examination
• Chest X ray / EKG / Blood study
• Echocardiography/ Other imaging tools
• Catheterization/ Other invasive tools
Accuracy of Tools
• History/PE : important, rarely specific
• X-ray/EKG : not-confirmative
• Echocardiography:
confirmative, but non-invasive
• Cardiac catheterization :
confirmative, but invasive
History Taking
• Cyanosis: onset, progression, anoxic spell
• Congestion: feeding, wt. gain, respiratory
infection, sweating, tachy-dyspnea
• Exercise tolerance: easy fatigability, DOE
• Possible Causes: maternal diseases, drug,
infection, family history
Physical Examination
• Inspection : general appearance, nutrition,
syndrome?, facial morphology, jugular venous pulse,
respiratory pattern, rate, chest retraction, alae nasi
flaring, dyspnea, precordial bulging, cyanosis,
clubbing
• Palpation: apical pulse, precordial activity, thrill,
arterial pulse, location and size of liver and spleen
• Auscultation: S1, S2, abnormal sounds, murmur
• Please do not pull out stethoscope before
you observe patients carefully
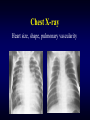
Chest X-ray
Heart size, shape, pulmonary vascularity
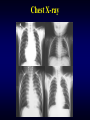
Chest X-ray
Electrocardiography
Purposes of Imaging
• Anatomic-pathologic diagnosis
• Hemodynamic assessment
(velocity, flow, pressure, stress-strain)
• Volume, function, wall motion, torsion
• Coronary perfusion / Metabolism
• Tissue characterization
Echocardiography
• Easy, non-invasive, accurate, real-time
• Anatomic and physiologic information
• Changed practice of pediatric cardiology
Echocardiograhy - Modalities
• M-mode / 2-D / 3-D
• Doppler / color Doppler
• Trans-thoracic, trans-esophageal,
trans-abdominal, trans-vaginal,
intra-cardiac, intra-vascular
Echocardiograhy
Echocardiograhy
M-mode Echocardiograhy
3-D Echocardiograhy
New Development in Echo
• Imaging: edge detection/auto-measurement
• Doppler: 3-D flow / stress-strain
• Contrast echo: coronary perfusion
Other Imaging Tools
• Magnetic Resonance Imaging (MRI)
• CT / Electron-beam CT (EBCT)
• Radionuclide / SPECT
• Positron Emission Tomography
Magnetic Resonance Imaging
Spin echo
Gradient echo Velocity encoded
Magnetic Resonance Imaging
• Sectional still image/ cine image/ 3-D
• Flow information / volume flow
• Less window dependant / post-op
study, older age / functional
evaluation
Magnetic Resonance Imaging
Magnetic Resonance Imaging
Computerized Tomography
Computerized Tomography
Radionuclide Study
Radionuclide Study
Positron Emission Tomography
Purposes of Catheterization
• Anatomic diagnosis
• Hemodynamic assessment
• Interventional procedure
Equipment
• Biplane monitor / Cine with digital subtraction
• Patient monitoring : EKG, BP, pulse oximeter
• Physiologic signal amplifier and recording device
• Blood gas, O2 consumption, Dye/ Thermodilution
• Emergency treatment tools :
• Room for Others : anesthesia, echo, exercise
Catheterization Room
Fluoroscopic Monitor
Physiologic Signal - Display & Recording
Catheterization vs Echocardiograpy
• How accurate non-invasive tests are
• Risk of cardiac catheterization
• How to obtain necessary information
during catheterization or surgery
• Nature of surgical correction
• Risk of possible undiagnosed diseases
Electrophysiologic Study
How to Approach to CHD
- as a Clinician Does this baby have a CHD?
– Which baby should be referred to pediatric cardiologist
– The urgency with which that referral should be made
– If not, what tests and in what order to make diagnosis
Babies with Suspected CHD
• Clinical assessment
– Mode of / age at presentation
– Physical examination
• Laboratory test
– CBC, ABGA, hyperoxic test
– Chest PA, EKG
– Echocardiography if available
Suspected CHD without Confirmation
Any magic bullet for all?
– IV inotropics
– PGE 1
– Decrease oxygen consumption
– General supportive care
Incidence of CHD
• Incidence of total CHD among races:
– the same in all races ; about 5 - 8 /1,000
• Ethnic difference in incidences of
individual anomalies and subtypes
• Associated non-cardiac malformation
Racial Difference of CHD
• Left sided lesions seem to be lower in Asians
• Right isomerism seems to be higher in Asians
• Subpulmonic VSD is higher in Asians
Classification of CHD
• Why classify : the sameness, differences
• How to classify : view point, purpose
Classification of CHD
• Clinical viewpoint
cyanotic versus acyanotic
shunts/obstruction/regurgitation
• Pathology viewpoint
normal vs abnormal connection
segmental approach
• Developmental viewpoint
Classification of CHD
Developmental viewpoint
• Ectomesenchymal tissue migration
abnormalities
• Abnormal intra-cardiac flow
• Cell death abnormalities
• Extra-cellular matrix abnormalities
• Abnormal targeted growth
• Abnormal situs and looping
Naming of CHD
• Unambiguous, accurate, and succinct
• Capable of describing any combination of
defects
• Allows for precise classification of
malformations to be made during patient’s life
• Useful both for anatomical, clinical, and
etiologic studies
Naming : Unambiguous?
• Different names for the same thing
• The same name for different things
Ambiguity
Different names for the same thing
–
–
–
–
–
L-transposition
ventricular inversion
{S,L,L} corrected transposition
(physiologically) corrected transposition
Atrial solitus, discordant AV/ VA connection
Ambiguity
The same names for different things
D- transposition
– a term for GA relationship
– a term for VA connection
– a term for specific diagnosis
Naming : Simple, Specific ?
• In most, simple : VSD, ASD, PDA, TOF
• In a few, not simple or specific : TA
• Rarely, complex : isomerism
Tricuspid Atresia
Right Isomerism
• Dextrocardia
• Bilateral SVC
• Separate hepatic vein
• TAPVR
• Complete AVSD
• LV hypoplasia
• Transposition
• PS or pul. Atresia
Fetal Circulation
• Is adapted to a special situation
• Depends on placenta for O2/nutrients
• Is rarely overloaded,
but if overloaded little reserve
Flow Pathway & Distribution
(% indicates the proportion of combined output )
SVC-RV-MPA-Duct-Des. Ao
IVC-PFO-LA-LV-Asc. Ao
* ductus arteriosus, ductus venosus,
atrial communication
Oxygen Saturation %
Fetal Circulation
• Parallel circulation (combined output)
• Communications between R & L heart
• Pulmonary circulation is redundant
Congenital Heart Diseases in Fetus
• Often silent :
– TGA : has little effect
– HLHS : RV is slightly overloaded
– PA + IVS : no effect at all
• When CHD causes volume overload,
heart fails and hydrops ensues
Transitional Circulation
Dramatic changes in circulation at the
moment of birth and onwards :
– Air breadth - lung expansion - Rp ↓
– Qp ↑ - LA pressure ↑ - PFO ↓
– P O2 ↑ - ductus arteriosus and venosus ↓
– Obliteration of placental circulation - Rs ↑
– IVC pressure ↓ - PFO ↓
Transitional Circulation & CHD
• As circulation separates, TGA can not
supply enough oxygen to the body
• Obstructed pathway in either side hardly
tolerate
– right : PA or critical PS in any CHD
– left : Aortic atresia or critical AS, IAA, COA
– mitral atresia + small PFO; obstructed TAPVR
Neonatal Circulation & CHD
• Neonatal circulation
– potential of increased Rp
– potential of atrial communication
– compliance of two ventricles is nearly equal
• CHD and neonatal circulation
– VSD, PDA : usually not symptomatic
– ASD : usually not symptomatic