Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neonatal Abstinence Syndrome: Improving short term outcomes by modifying the treatment protocol
Lori Devlin, DO, MHA, Timothy Lau, MS
Introduction
Opiate use and abuse during pregnancy is a rapidly growing public health concern, which has
considerably increased healthcare utilization and healthcare costs. Neonatal Abstinence Syndrome
(NAS) is a drug withdrawal syndrome classically associated with the abrupt cessation of maternal opiates
after birth and accounts for a substantial proportion of the health care burden {1}{2}. The national
incidence of NAS increased from 3.4 per 1000 live births in 2009 to 5.8 per 1000 hospital births in 2012
and neonatal intensive care (NICU) admissions for NAS increased 4 fold between 2004 and 2013 {1}{3}.
Regional variation in the incidence of NAS has been noted. The East South Central Region of the United
States, which includes Kentucky, Tennessee, Mississippi and Alabama, represents the largest proportion
of affected infants at 16% of the national incidence {3}. In Kentucky hospital discharge records indicate
that the number of newborns hospitalized with NAS has increased 23-fold over the last decade (46 vs.
1,060 infants in 2001 and 2014, respectively) {4}.
Clinically significant symptoms appear in 55-94% of opiate exposed neonates {5}. The presentation of
NAS symptoms is variable from patient to patient. Clinical symptoms are impacted by the sum total of
fetal exposure, the type(s) and purity of drug(s) consumed during pregnancy, maternal and infant
metabolism, genetic and epigenetic factors, and variability in the kinetics of placental drug transfer
{6}{7{8}{9}{10}{11}
. Affected infants in many regions of the country are provided with pharmacological therapy
for drug withdrawal symptoms in the NICU. The percentage of NICU days attributed to NAS increased
from 0.6% in 2004 to 4% in 2013. The proportion of NAS infants who require pharmacotherapy has also
increased from 74% in 2004-2005 to 87% in 2012-2013{1}.
The severity of withdrawal is assessed with an observer rated scale. The most commonly used scale is
the Finnegan Score for Neonatal Abstinence Syndrome (FNAS) {5}. FNAS assesses 21 clinical symptoms of
drug withdrawal, which allows for a thorough assessment of withdrawal {6}. However, it is a lengthy tool
that requires extensive training and experience to ensure accurate scoring {12}. Lack of uniformity in
assessment of infants with NAS complicates care and prolongs hospitalization {13} {14} {15} {16}.
The surge in the number of infants diagnosed with NAS, variability in assessment of the severity of NAS
and the increased need for pharmacologic treatment for infants with NAS has intensified the financial
impact of the disease. National aggregate hospital charges reached $1.5 billion in 2012 {2}{3}.
Identification and implementation of measures to stunt the growing economic impact of NAS are
needed. The use of a standardized treatment protocol for neonatal withdrawal is an intervention that
has been associated with a decrease in the length of treatment (LOT) and length of stay (LOS) {5} {17} {18}
{19}
. Standardization of care became a local priority in 2005 when an increase in the number of infants
with NAS was noted in the NICU at the University of Louisville Hospital. At that time a multidisciplinary
group from the hospital reviewed the evidence and developed a treatment protocol. The details of the
protocol (SP1) are noted in figure 1. Decreases in LOT and LOS were noted with the initiation of SP1
(data not shown). Due to the small number of infants with NAS prior to 2005, the differences were not
statistically significant.
A steady increase in the national and statewide incidences of NAS has been seen over the last decade.
In 2013 the Governor of Kentucky cited perinatal drug exposure as a state public health priority. Public
health forums were held and committees were developed to address policy, resource integration and
standardization of treatment. In 2014 neonatologists, neonatal nurse practitioners and neonatal nurses
were brought together to reevaluate the literature and develop a unified NAS treatment protocol. A
standardized treatment plan was presented to hospitals throughout the state in 2015 as a standard
pharmacologic approach for NAS in Kentucky. Details of this protocol (SP2) are noted in Figure 2.
Notable differences between the protocols were the dosing intervals for morphine administration, the
frequency and duration of the morphine wean and the use of clonidine rather than phenobarbital as
adjunctive therapy.
The purpose of this study was to compare the impact of the two treatment protocols on the length of
treatment, length of hospitalization and need for adjunctive therapy in term infants with NAS. All
infants were treated with pharmacologic therapy in the NICU of a single inner-city hospital between
2005 and 2015.
Methods
The University of Louisville Institutional Review Board approved this retrospective cohort study prior to
study initiation. Data were derived from medical records of infants treated in the University of Louisville
Hospital Neonatal Intensive Care Unit (Louisville, KY) from 2005 to 2015. Diagnosis-related group codes
and NICU logbooks were used to identify term infants (greater than or equal to 37 0/7 weeks gestation)
with NAS. Records of infants who met the inclusion criteria were reviewed to determine if
pharmacological therapy was used. All infants not receiving pharmacological therapy were excluded.
Charts were reviewed for demographic information including sex, gestational age and birth weight.
Maternal drug history and maternal and infant toxicology screens were recorded. Pharmacological
intervention, including the length of morphine therapy and need for adjuvant drug therapy was noted.
Length of stay was derived from admission and discharge dates for each infant
Infants cared for in the NICU between 2005 and March 2014 (n= 146) were treated with the locally
generated standardized protocol (SP1 – Figure 1) and infants treated after March 2014 (n= 44) were
treated with the state generated protocol (SP2 – Figure 2). Both treatment protocols used morphine as
the first pharmacologic agent; however, morphine dosing was every 4 hours in SP1 and every 3 hours in
SP2 and weaning of the morphine differed between the studies. Additionally, infants treated with SP1
received phenobarbital as adjunctive therapy if symptoms were not well controlled on high dose oral
morphine. Infants treated with SP2 received clonidine as adjunctive therapy.
Differences in birth weight and gestational age between treatment groups were assessed with a student
T-test and differences in sex between groups were assessed with a Chi square test (goodness of fit) SPSS
version 22.
ANCOVA (R version 3.1.2) was used to evaluate the impact of each protocol on the length of morphine
therapy and length of hospital stay. The model controlled for birth weight, gestational age, sex, and
fetal exposure to heroin, methadone, buprenorphine, multiple opiates and benzodiazepines. Exposure
was determined by maternal history and/or maternal and infant toxicology screens. Interactions
between in-utero drug exposure and the protocol were evaluated with backwards elimination multiple
regression.
The need for adjunctive therapy in the infants treated with each protocol was assessed with a with a Chi
square test (goodness of fit) SPSS version 22.
Results
The primary outcome measure was length of morphine therapy for infants treated with protocol 1 (SP1)
vs. protocol 2 (SP2). Secondary outcomes were length of stay and need for adjunctive therapy.
Demographic data are presented in table 1 and no statistically significant differences were noted in the
gestational age, weight or sex between infants treated in protocol 1 or protocol 2.
The average length of morphine therapy was decreased by 23.7% (95% CI 12.5 - 33.3%) or 8.5 days (95%
CI 4.5 -12) for infants treated with SP2 when compared to infants treated with SP1 (p< 0.001). The
average length of stay for infants treated with SP2 was also decreased by 22.5% (95% CI 12.4% - 31.3%)
or 9.2 days (95% CI 5.1 to 13) when compared to infants treated with SP1 (p< 0.001) (Figure 3). The
need for adjunctive pharmacologic therapy was decreased by 24% in patients treated with SP2 vs. SP1
(p=0.004) (Figure 4). The decrease in length of stay resulted in an average reduction of hospital charges
by $27,090 per patient (adjusted 2015 US Dollars) using national averages for per day charges derived by
SW Patrick for infants pharmacologically treated for NAS {3}. The use of multiple opiates and
benzodiazepines, both of which are known to exacerbate symptoms of NAS, were not found to be
statistically significant between protocols.
One relevant and significant interaction was noted within the backwards elimination multiple
regression, between methadone and protocol. While the average difference in length of stay for all
infants was 8.5 days when comparing SP2 vs. SP1, infants exposed to methadone in-utero had a 1-day
reduction in the benefit (e.g., an average difference of 7.5 days instead of 8.5 days).
Discussion
In this cohort of infants from a single inner-city hospital, we found clinical and statistically significant
differences in outcomes (LOT, LOS and need for adjunctive therapy) for infants who received treatment
from two distinct standardized protocols. Implementation of each of the standardized protocols
improved outcomes compared to an individualized treatment approach. This finding lends additional
support to the efficacy and cost effectiveness of a standardized treatment protocol for infants with NAS.
The data also suggest that collaborative review of treatment protocols for NAS by a regional
multidisciplinary group will enhance short-term outcomes and reduce hospital costs for infants with
NAS.
When SP1 was developed, there was a significant concern that daily weaning of oral morphine would
lead to rebound symptoms and the need for escalation of pharmacologic therapy. This was addressed
by restricting morphine weans to every 48-72 hours despite low Finnegan scores. We found after
implementation of SP2 that our concerns were not substantiated and many infants may have tolerated
more aggressive weaning. We also determined that interval weaning of morphine, which we believed
was important to prevent rebound symptoms when SP1 was developed, was not effective and led to
prolonged opiate exposure.
Prenatal exposure to opiates, especially long acting opiates such as methadone, has been shown to
decrease myelination in the developing rat brain and in a small cohort of exposed infants {20} {21}.
Myelination is essential for efficient conduction of neuronal impulses. Myelination begins in the third
trimester of fetal development and continues through puberty {22}. The endogenous opioid system is
crucial to ensure appropriate oligodendrocyte development and proper myelination. Exposure of the
fetus and infant to exogenous opiates inhibits endogenous opioid production and could disrupt
myelination and impact long-term developmental outcome {20} {23}. Minimal information is available on
the effects of postnatal opioid administration on the developing brain. Given the potential impact of
exogenous opioids on myelination of the neonatal brain, every effort should be made to decrease
postnatal exposure. The implementation of SP2 decreased the need for morphine by an average of 8.5
days. Additional studies are needed to determine the physiologic and developmental impact of
decreased opioid exposure in the postnatal period.
Although all infants in this cohort were exposed in-utero to opioids, the type(s) used during pregnancy
was variable as depicted in Table 2. Total fetal exposure varied significantly between opiate dependent
women and was nearly impossible to quantify. Fetal exposure to multiple opiates and multiple drugs of
abuse, specifically benzodiazepines and tobacco, exacerbate the severity of withdrawal {24}. In our data
set the use of multiple opiates and benzodiazepines were controlled for and were not found to have a
statistically significant impact on the effectiveness of the protocol.
Previous studies have shown that infants exposed to methadone require a longer length of treatment
than those exposed to buprenorphine and other short acting opiates such as heroin {13}. In our study,
infants exposed to methadone in-utero and then treated with SP2 vs. SP1 had an average LOT and LOS
that was 1 day greater than infants exposed to other opiates during pregnancy (p=0.003). In other
words, infants exposed to methadone do not benefit as greatly by the new protocol as infants not
exposed to methadone. While the average decrease in length of stay was 8.5 days when comparing the
two protocols, for infants on methadone, the decrease was only 7.5 days.
Adjunctive therapy with phenobarbital has been noted to decrease the severity of opioid withdrawal
and reduce length of stay and cost of hospitalization {19} {25} {26}. Surran et al. {19} in a prospective analysis
of phenobarbital vs. clonidine found that the use of phenobarbital as second line therapy led to a
significant decrease in the length of morphine treatment and the length of stay when compared to
clonidine. Infants in the study by Surran et al. and in other studies that used phenobarbital as adjunctive
therapy were often discharged home on the phenobarbital. Many infants remained on the medication
for weeks to months after the initial hospital discharge {19} {25 {27}. Phenobarbital acts on the gammaaminobutyric acid receptors in the central nervous system inducing sedative effects. Extended
treatment with phenobarbital may negatively impact neurodevelopmental and behavioral outcomes
{28}
. Although adjunctive therapy with clonidine was associated with 5 additional days of morphine
therapy in the study by Surran et al., patients left the hospital medication free.
Clonidine, an alpha2-adrenergic receptor agonist, reduces sympathetic outflow, which has been shown
to be upregulated in infants with NAS {29}. Clonidine inhibits noradrenaline release in the locus coeruleus
resulting in a decrease in withdrawal symptoms. Clonidine has been evaluated in several small studies
and has been shown to be a safe and efficacious adjunctive therapy for infants with NAS although the
effect on long-term outcome is unknown. The use of clonidine in the pharmacologic management of
NAS has been associated with a decrease in the duration of treatment and length of stay
{29} {30} {31} {32}
.
Unlike phenobarbital, clonidine comes in an ethanol-free suspension that has exceptional bioavailability
{33} {34}
. Although rare, potential side effects with clonidine include bradycardia, hypotension and
sedation. Abrupt cessation of clonidine may result in sympathetic over-activity. Clinical symptoms
include increased blood pressure, heart rate, tremors, agitation and diaphoresis. Side effects can be
prevented by tapering the dose prior to discontinuation of the medication {33}. In our study, infants
treated with SP2, which stipulated that clonidine be used as an adjunctive therapy had a shorter LOT
and LOS than those treated with SP1 that specified phenobarbital as a second line therapy. The longterm effect of treatment with clonidine on developmental outcomes remains unknown at this time.
Minimizing side effects by reducing the need for adjunctive pharmacologic therapy is essential. We
found that the simple transition of morphine administration from every 4 hours to every 3 hours led to a
24% reduction in the need for adjunctive therapy. We also found that an aggressive morphine wean did
not result in the need for additional adjunctive therapy.
The exorbitant growth of in-utero opiate exposure and NAS over the last decade has overwhelmed
health care resources and escalated health care costs. Between 2000 and 2009, national estimates for
total hospital charges attributed to NAS increased from $190 million dollars to $720 million dollars {2}.
Inflation adjusted mean hospital charges for infants requiring pharmacologic therapy for NAS in 2012
reached $93,400 per patient. State Medicaid programs bear the majority of the financial burden of this
disease covering eighty percent of affected infants treated in the United States {3}. Measures to control
costs are essential as the number of affected infants continue to climb. Using data from Patrick et al {3}
a mean extrapolated daily charge for NAS pharmacologic treatment is approximately $3,010.00 (2015
adjusted dollars). The resulting savings using SP2 in our population may be as much as $27,090 per
patient. When applied to the 44 patients treated with SP2 in the study, the average decrease in hospital
charges would have been $ 1.19 million (2015 adjusted dollars).
The clinical presentation of NAS and each infant’s response to postnatal opioid therapy are complex and
highly variable between patients. As the NAS reaches epidemic proportions it is essential that efforts be
made to minimize postnatal opioid therapy, decrease length of stay and control the cost of medical care.
In this study we demonstrated that not all treatment protocols are equal. Morphine administration
every 3 hours with the implementation of an aggressive weaning strategy and adjunctive therapy with
clonidine reduced length of treatment, length of stay, need for adjunctive therapy and cost of
hospitalization in a diverse group of term infants with NAS.
Limitations
We acknowledge that the study is limited in its retrospective design and thus is subject to bias and
inaccuracies in the medical record. We also realize that only the impact of the entire treatment protocol
can be assessed with this study design. The impact of each difference between SP1 and SP2 cannot be
assessed. Additionally patients treated with SP1 were collected over a 9-year period during which
trends in maternal usage and drugs of abuse could have been significantly varied from current patterns
of abuse during pregnancy. Subtle changes in neonatal care over the last 11 years could have also had
an unmeasured impact on the short-term outcomes for affected infants.
References
1. Tolia VN, Patrick SW, Bennett MM, Murthy K, Sousa J, Smith PB, et al. Increasing incidence of the
neonatal abstinence syndrome in U.S. Neonatal icus. N Engl J Med 2015, May 28;372(22):2118-26.
2. Patrick SW, Schumacher RE, Benneyworth BD, Krans EE, McAllister JM, Davis MM. Neonatal
abstinence syndrome and associated health care expenditures: United states, 2000-2009. JAMA 2012,
May 9;307(18):1934-40.
3. Patrick SW, Davis MM, Lehmann CU, Lehman CU, Cooper WO. Increasing incidence and geographic
distribution of neonatal abstinence syndrome: United states 2009 to 2012. J Perinatol 2015,
Aug;35(8):650-5.
4. Neonatal Abstinence Syndrome in Kentucky Annual Report. Frankfort: Kentucky Department for
Public Health Division of Maternal and Child Health; Dec 2015
5. Hudak ML, Tan RC, American Academy of Pediatrics. Neonatal drug withdrawal. Pediatrics 2012,
Feb;129(2):e540-60.
6. Finnegan LP, Kron RE, Connaughton JF, Emich JP. Assessment and treatment of abstinence in the
infant of the drug-dependent mother. Int J Clin Pharmacol Biopharm 1975, Jul;12(1-2):19-32.
7. Hoekelman RA, Blatman S, Friedman SB, Nelson NM, Seidel HM. Primary Pediatric Care. 2e ed. St.
Louis: Mosby; 1992b.
8. Desai RJ, Huybrechts KF, Hernandez-Diaz S, Mogun H, Patorno E, Kaltenbach K, et al. Exposure to
prescription opioid analgesics in-utero and risk of neonatal abstinence syndrome: Population based
cohort study. BMJ 2015;350:h2102.
9. Jones HE, Harrow C, O'Grady KE, Crocetti M, Jansson LM, Kaltenbach K. Neonatal abstinence scores in
opioid-exposed and nonexposed neonates: A blinded comparison. J Opioid Manag 2010;6(6):409-13.
10. Wachman EM, Hayes MJ, Brown MS, Paul J, Harvey-Wilkes K, Terrin N, et al. Association of OPRM1
and COMT single-nucleotide polymorphisms with hospital length of stay and treatment of neonatal
abstinence syndrome. JAMA 2013, May 1;309(17):1821-7.
11. Wachman EM, Hayes MJ, Lester BM, Terrin N, Brown MS, Nielsen DA, Davis JM. Epigenetic variation
in the mu-opioid receptor gene in infants with neonatal abstinence syndrome. J Pediatr 2014,
Sep;165(3):472-8.
12. Bagley SM, Wachman EM, Holland E, Brogly SB. Review of the assessment and management of
neonatal abstinence syndrome. Addict Sci Clin Pract 2014;9(1):19.
13. Jones HE, Kaltenbach K, Heil SH, Stine SM, Coyle MG, Arria AM, et al. Neonatal abstinence syndrome
after methadone or buprenorphine exposure. N Engl J Med 2010, Dec 9;363(24):2320-31.
14. Orlando S. An overview of clinical tools used to assess neonatal abstinence syndrome. J Perinat
Neonatal Nurs 2014;28(3):212-9.
15. Zahorodny W, Rom C, Whitney W, Giddens S, Samuel M, Maichuk G, Marshall R. The neonatal
withdrawal inventory: A simplified score of newborn withdrawal. J Dev Behav Pediatr 1998,
Apr;19(2):89-93.
16. Maguire D, Cline GJ, Parnell L, Tai CY. Validation of the finnegan neonatal abstinence syndrome toolshort form. Adv Neonatal Care 2013, Dec;13(6):430-7.
17. Hall ES, Wexelblatt SL, Crowley M, Grow JL, Jasin LR, Klebanoff MA, et al. Implementation of a
neonatal abstinence syndrome weaning protocol: A multicenter cohort study. Pediatrics 2015,
Oct;136(4):e803-10.
18. Asti L, Magers JS, Keels E, Wispe J, McClead RE. A quality improvement project to reduce length of
stay for neonatal abstinence syndrome. Pediatrics 2015, Jun;135(6):e1494-500.
19. Surran B, Visintainer P, Chamberlain S, Kopcza K, Shah B, Singh R. Efficacy of clonidine versus
phenobarbital in reducing neonatal morphine sulfate therapy days for neonatal abstinence syndrome. A
prospective randomized clinical trial. J Perinatol 2013, Dec;33(12):954-9.
20. Vestal-Laborde AA, Eschenroeder AC, Bigbee JW, Robinson SE, Sato-Bigbee C. The opioid system and
brain development: Effects of methadone on the oligodendrocyte lineage and the early stages of
myelination. Dev Neurosci 2014;36(5):409-21.
21. Walhovd KB, Westlye LT, Moe V, Slinning K, Due-Tønnessen P, Bjørnerud A, et al. White matter
characteristics and cognition in prenatally opiate- and polysubstance-exposed children: A diffusion
tensor imaging study. AJNR Am J Neuroradiol 2010, May;31(5):894-900.
22. Snell RS. Clinical neuroanatomy. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins;
2010a.
23. Konijnenberg C, Melinder A. Prenatal exposure to methadone and buprenorphine: A review of the
potential effects on cognitive development. Child Neuropsychol 2011;17(5):495-519.
24. Patrick SW, Dudley J, Martin PR, Harrell FE, Warren MD, Hartmann KE, et al. Prescription opioid
epidemic and infant outcomes. Pediatrics 2015, May;135(5):842-50.
25. Coyle MG, Ferguson A, Lagasse L, Oh W, Lester B. Diluted tincture of opium (DTO) and phenobarbital
versus DTO alone for neonatal opiate withdrawal in term infants. J Pediatr 2002, May;140(5):561-4.
26. Sarkar S, Donn SM. Management of neonatal abstinence syndrome in neonatal intensive care units:
A national survey. J Perinatol 2006, Jan 1;26(1):15-7.
27. Backes CH, Backes CR, Gardner D, Nankervis CA, Giannone PJ, Cordero L. Neonatal abstinence
syndrome: Transitioning methadone-treated infants from an inpatient to an outpatient setting. J
Perinatol 2012, Jun;32(6):425-30.
28. Meador KJ, Baker G, Cohen MJ, Gaily E, Westerveld M. Cognitive/behavioral teratogenetic effects of
antiepileptic drugs. Epilepsy Behav 2007, Nov;11(3):292-302.
29. Agthe AG, Kim GR, Mathias KB, Hendrix CW, Chavez-Valdez R, Jansson L, et al. Clonidine as an
adjunct therapy to opioids for neonatal abstinence syndrome: A randomized, controlled trial. Pediatrics
2009, May;123(5):e849-56.
30. Hoder EL, Leckman JF, Ehrenkranz R, Kleber H, Cohen DJ, Poulsen JA. Clonidine in neonatal narcoticabstinence syndrome. N Engl J Med 1981, Nov 19;305(21):1284.
31. Leikin JB, Mackendrick WP, Maloney GE, Rhee JW, Farrell E, Wahl M, Kelly K. Use of clonidine in the
prevention and management of neonatal abstinence syndrome. Clin Toxicol (Phila) 2009, Jul;47(6):5515.
32. Bada HS, Sithisarn T, Gibson J, Garlitz K, Caldwell R, Capilouto G, et al. Morphine versus clonidine for
neonatal abstinence syndrome. Pediatrics 2015, Feb;135(2):e383-91.
33. Levinson ML, Johnson CE. Stability of an extemporaneously compounded clonidine hydrochloride
oral liquid. Am J Hosp Pharm 1992, Jan;49(1):122-5.
34. Xie HG, Cao YJ, Gauda EB, Agthe AG, Hendrix CW, Lee H. Clonidine clearance matures rapidly during
the early postnatal period: A population pharmacokinetic analysis in newborns with neonatal abstinence
syndrome. J Clin Pharmacol 2011, Apr;51(4):502-11.
Table 1 – Demographics of Study Infants
BW(kg)
GA(weeks)
Male (%)
Protocol 1
(SP1)
(n=146)
3.01 ± 0.46
39.0 ± 1.1
57.2%
Abbreviations: BW, birth weight; GA, gestational age.
a
P Values calculated with t test
b
P value calculated with X2 test of independence
Protocol 2
(SP2)
(n=44)
2.93 ± 0.39
38.7 ± 1.3
59.1%
P
Value
0.07a
0.21a
0.82b
Table 2 – Fetal drug exposure to opioids and other drugs of abuse
Opioids
Buprenorphine
Heroin
Hydrocodone
Hydromorphone
Methadone
Morphine
Oxycodone
Oxymorphone
Unspecified opiates
Other Drugs of Abuse
Amphetamines
Barbiturates
Benzodiazepines
Cocaine
Gabapentin
Marijuana
Methamphetamine
Total
Number (%)
(n=190)
Protocol 1
(SP1)
Number (%)
(n=146)
Protocol 2
(SP2)
Number (%)
(n=44)
18 (9)
24 (12)
29 (15)
4 (2)
74 (39)
11 (6)
47 (24)
5 (3)
88 (46)
9 (6)
13 (8)
28 (19)
2 (1)
61 (42)
3 (2)
43 (29)
4 (3)
67 (46)
9 (20)
11 (25)
4 (9)
2 (5)
13 (30)
8 (18)
4 (9)
1 (2)
21 (48)
11 (6)
2 (1)
20 (10)
26 (14)
2 (1)
18 (9)
4 (2)
8 (5)
2 (1)
18 (10)
19 (13)
2 (1)
14 (10)
2 (1)
3 (7)
0
2 (5)
7 (15)
0
4 (9)
2 (5)
Fetal exposure was determined through maternal history and urine toxicology screens combined
with neonatal urine and meconium toxicology screens.
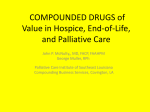
Figure 1 – Protocol 1 (SP1) for the initiation and treatment of Neonatal Abstinence Syndrome (NAS)
Initiation
3 consecutive Finnegan scores ≥ 8
or
2 consecutive Finnegan scores ≥ 12
Begin po morphine
0.05mg/kg/dose
For 2 consecutive Finnegan >
than 15 begin 0.1mg/kg IV q4hr
Capture
Weaning
If consecutive Finnegan scores are still
≥ 8 x 3 or ≥ 12 x 2
Increase morphine dose to
0.1mg/kg/dose q4hr
If Finnegan scores < 8 for 24hr wean morphine
If consecutive Finnegan scores are still
≥ 8 x 3 or ≥ 12 x 2
Start phenobarbital
2.5mg/kg/dose q12hr
Change to po dosing once score
consistently < 12 in 24hr period
If consecutive Finnegan scores remain
≥ 8 x 3 or ≥ 12 x 2
Increase morphine by 10% until scores
consistently < 8
Max dose 0.25mg/kg/dose q4hr due to
possibility of respiratory depression
Weaning Morphine
Finnegan scores < 8 wean morphine
by 10% q48hr
When morphine dose reaches
0.025 mg/kg/dose and Finnegan score < 8 in a
24hr period begin lengthening the dosing
interval
Every 6hr for 48 to 72hr then
Every 8hr for 48 to 72hr then
Every 12hr for 48 to 72hr then
Discontinue morphine
Once off morphine and Finnegan scores < 8 for
24hr wean discontinue phenobarbital
Monitor in the hospital for 48-72hr for rebound
withdrawal
Abbreviations: mg/kg, milligrams per kilogram; q, every; hr, hours; IV, intravenous; po, by mouth
Figure 2 – Protocol 2 (SP2) for the initiation and treatment of Neonatal Abstinence Syndrome (NAS)
Initiation
Capture
Weaning
3 consecutive Finnegan scores ≥ 8
or
2 consecutive Finnegan scores ≥ 12
If consecutive Finnegan scores are still
≥ 8 x 3 or ≥ 12 x 2
Increase morphine dose by 25% until
you reach a dose of 0.13mg/kg/dose
If Finnegan scores < 8 x 24hr wean morphine
Begin treatment with
po morphine
0.05mg/kg/dose q3hr
If consecutive Finnegan scores remain
≥ 8 x 3 or ≥ 12 x 2
Start clonidine 1 mcg/kg/dose q3hr
Weaning Morphine
Scores ≤ 6 wean morphine by 10-15% q24hr
Scores greater than 6 but < 8 wean 10-15% q48hr
BP should be obtained every 8hr
while on clonidine
3 Scores in 24hr ≥ 8 do not wean
(Increase dose or add an additional drug if
consecutive scores > 12 x 2 during weaning process)
If Finnegan consecutive scores still
≥ 8 x 3 or ≥ 12 x 2
Increase morphine by 25%
If consecutive Finnegan scores remain
≥ 8 x 3 or ≥ 12 x 2
Increase clonidine to 1.5mcg/kg q3hr
If consecutive Finnegan scores still
≥ 8 x 3 or ≥ 12 x 2
Continue to increase morphine by
25% until the infant is captured
Max dose 0.25mg/kg/dose q3hr
Discontinue morphine at a dose of 0.02mg q3hr
and Finnegan scores < 8
Off morphine and Finnegan scores < 8 for 24hr
wean clonidine
Weaning Clonidine
If dose is 1.5mcg/kg/dose q3hr then wean to
1mcg/kg/dose q3hr
In 24 hours wean to q6hr if scores < 8
Monitor BP every 8hr
D/C clonidine once scores < 8 for 24-48hr
Monitor in the hospital for at least 48hr off
clonidine to assure no rebound hypertension
Abbreviations: mg/kg, milligrams per kilogram; q, every; hr, hours; po, by mouth; BP, blood
pressure
Figure 3 – Length of treatment and length of stay for protocol 1 (PS1) vs. protocol 2 (PS2)
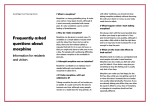
Figure 4 - Need for adjunctive therapy for Neonatal Abstinence Syndrome (NAS) by protocol
Protocol 1
Protocol 2
100%
0.63
0.39
63%
75%
*
39%
50%
25%
p=0.004
0%
Protocol 1
Protocol 2
Five neonates treated in protocol 1 (SP1) required triple therapy with morphine, phenobarbital and
clonidine. No neonates treated in protocol 2 (SP2) required triple therapy.
Protocol 2 – No neonates required needed triple therapy