Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
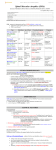
REVIEW REQUEST FOR SPINRAZA™ (Nusinersen) Provider Data Collection Tool Based on Medical Policy DRUG.00104 Policy Last Review Date: 02/02/2017 Request Date: / Initial Request Buy and Bill Policy Effective Date: 02/16/2017 Provider Tool Effective Date: 01/21/2017 / Subsequent Request Individual’s Name: Date of Birth: / / Individual’s Phone Number: Insurance Identification Number: Primary Diagnosis: Diagnosis Code(s) (if known): Ordering Provider Name & Specialty: Individual’s Weight (lbs) (kg) Provider ID Number (if known): Office Address: Office Phone Number: Office Fax Number: Servicing Provider Name & Specialty (If different than Ordering Provider): Provider ID Number (if known): Office Address: Office Phone Number: Office Fax Number: Place of Service: Home Office Dialysis Center Outpatient Hospital Ambulatory Infusion Ambulatory Infusion Center Other: Drug Name/HCPCS Code (if known) Dose to be administered: (mg) SPINRAZA™ (Nusinersen) J3490 Other Other: When did the individual first start this drug? Frequency (Days, Wks, Months) / / Duration: Start Date For This Request: (Weeks) / / This data collection tool is intended to facilitate a medical necessity review request for initial and continued use of Nusinersen (SPINRAZA™) in the treatment of spinal muscular atrophy. 1) Initial Request for Treatment Request is for an initial 6 months of Nusinersen (SPINRAZA™) treatment of an individual diagnosed with confirmed spinal muscular atrophy If checked, please mark all of the following that apply: Individual’s spinal muscular atrophy diagnosis has been confirmed and documented by: SMA diagnostic test results confirming 0 copies of SMN1 Molecular genetic testing of 5q SMA for homozygous gene deletion Molecular genetic testing of 5q SMA for homozygous conversion mutation Molecular genetic testing of 5q SMA for compound heterozygote Genetic testing confirming no more than 2 copies of SMN2 SMA-associated symptoms before 6 months of age Other: (if checked please list the confirming test) 1 REVIEW REQUEST FOR SPINRAZA™ (Nusinersen) Provider Data Collection Tool Based on Medical Policy DRUG.00104 Policy Last Review Date: 02/02/2017 Policy Effective Date: 02/16/2017 Provider Tool Effective Date: 01/21/2017 2) Request for Continued Treatment Request is for an additional 6 months of Nusinersen treatment, beyond the initial 6 months of treatment, of an individual diagnosed with confirmed spinal muscular atrophy Request is for continued Nusinersen treatment at 6 month intervals If either of the above is checked, please mark all of the following that apply: A clinically significant improvement in the individual’s spinal muscular atrophy symptoms, compared to the predicted natural history trajectory of disease, has been documented Individual’s diagnosis of spinal muscular atrophy has been confirmed and documented by: (Check all that apply) SMA diagnostic test results confirming 0 copies of SMN1 Molecular genetic testing of 5q SMA for homozygous gene deletion Molecular genetic testing of 5q SMA for homozygous conversion mutation Molecular genetic testing of 5q SMA for compound heterozygote Genetic testing confirming no more than 2 copies of SMN2 SMA-associated symptoms before 6 months of age Other: (if checked please list the confirming test) 3) Other Use(s) (Please submit all supporting documents including labs, progress notes, imaging, etc., for review.) This request is being submitted: Pre-Claim Post–Claim. If checked, please attach the claim or indicate the claim number I confirm that the information entered on this form is accurate and complete based on the records available at the time of this request. I understand the health plan or its designees may request medical documentation to verify the accuracy of the information reported on this form. / / Name & Title of Provider or Provider Representative Completing Form Date & attestation (Please Print)* *The attestation fields must be completed by a provider or provider representative in order for the tool to be accepted Anthem UM Services, Inc., a separate company, is the licensed utilization review agent that performs utilization management services on behalf of your health benefit plan or the administrator of your health benefit plan. 2