Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
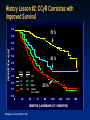
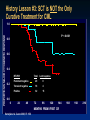
A CME-certified Oncology Exchange Activity METHOD OF PARTICIPATION Prior to the start of the program, please check your syllabus to ensure you have the following printed program materials: • Pre-activity Survey – Located at the front of your syllabus • CME Evaluation with Post-activity Survey – Located at the back of your syllabus Disclosures All relevant financial relationships with commercial interests reported by faculty speakers, steering committee members, non-faculty content contributors and/or reviewers, or their spouses/partners have been listed on page 5 of your program syllabus. Off-label Discussion Disclosure This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the Food and Drug Administration. PCME does not recommend the use of any agent outside of the labeled indications. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications and warnings. The opinions expressed are those of the presenters and are not to be construed as those of the publisher or grantors. Educational Objectives At the conclusion of this activity, participants should be able to demonstrate the ability to: • Identify changes in therapeutic indications and clinical practice guideline for CML • Understand practical aspects of monitoring responses in patients with CML • Identify the role of BCR-ABL mutations in making treatment decisions in CML • Review emerging data from ongoing studies of novel treatment regimens and evaluate ongoing clinical trials of investigational agents Pre-activity Survey • Please remove the Pre-activity Survey from the front of your packet • Your answers are vital to our understanding of the effectiveness of this CME program, and will help shape future educational activities and topics • Please fill in the most appropriate answer(s) for the questions below: – Degree: MD/DO Nursing Professional PharmD Other: _____________________________ – Specialty: Oncology/Hematology Internal Medicine Transplant specialist Other: ___________ Pre-activity Survey Question 1 Please rate your level of confidence in treating and managing patients with chronic myelogenous leukemia (CML): 1 Not confident 2 3 4 5 Expert Pre-activity Survey Question 2 Please rate your level of competence in individualizing treatment options for patients with CML based on patient and disease characteristics: 1 Not competent 2 3 4 5 Expert Pre-activity Survey Question 3 Six years after starting imatinib, a 53-year-old patient’s BCR-ABL/ABL has increased to 27.3%. After performing a bone marrow biopsy, the patient is still in chronic phase, has 75% Ph+ metaphases and an F317L mutation. The patient receives nilotinib at 400 mg for 12 months after which there is no cytogenetic response. The most suitable option for this patient would be to: a) Continue therapy unchanged b) Consider ponatinib, omacetaxine, or SCT c) Consider bosutinib or dasatinib d) None of the above, enroll in a clinical trial Pre-activity Survey Question 4 A 37-year-old male was diagnosed with CML and treated with imatinib 400 mg for 12 months. He was re-evaluated and found to be in hematologic and partial cytogenetic response. Which of the following options would NOT be appropriate at this point: a) Repeat mutational analysis b) Switch therapy c) Check patient’s compliance with medications d) Continue treatment e) None of the above Pre-activity Survey Question 5 Cytogenetic analysis at 6 months of a 45-year-old female patient, who received prior imatinib, shows Philadelphia chromosome in 45% of metaphases and a BCR-ABL/ABL of 0.15. According to the 2013 European LeukemiaNet recommendations for the management of CML, how would you characterize this response. a) Failure b) Warning c) Suboptimal response d) Optimal response Pre-activity Survey Question 6 Which of the following treatment options can be considered for a patient who has failed imatinib and dasatinib or nilotinib: a) Omacetaxine b) Bosutinib c) Ponatinib d) Any of the above Evolution of CML Therapy Signal Transduction Inhibition in CML The Beginning All seven individuals showed a similar minute chromosome. The findings suggest a causal relationship between the chromosome abnormality observed and chronic granulocytic leukemia. Nowell PC & Hungerford DA. Science 1960, 132: 1497 The Evolution of CML Therapy Chemotherapy SCT IFN TKI History Lesson #1: SCT is Curative (For Some) Leukemia-Free Survival Overall Survival 58% 50% Reprinted with permission. © (2013) American Society of Clinical Oncology. All rights reserved. Arora, M et al: J Clin Oncol 27(10): 1644-1652. History Lesson #2: CCyR Correlates with Improved Survival SURVIVAL BY CG RESPONSE 1.0 78 % 0.9 PROPORTION ALIVE 0.8 0.7 0.6 39 % 0.5 0.4 Total 0.3 0.2 0.1 Dead 140 38 CR 72 40 PR 110 86 Minor 180 138 Others (P < 0.0001) 25 % 0.0 0 24 48 72 96 120 144 168 MONTHS (LANDMARK AT 12 MONTHS) Kantarjian et al. Cancer 2003; 97: 1033 192 History Lesson #3: SCT is NOT the Only DURATION OF for MAJOR CG RESPONSE BY RT-PCR Curative Treatment CML PROPORTION IN MAJOR CYTOGENETIC RESPONSE 1.0 P < 0.001 0.8 0.6 0.4 RT-PCR 0.2 Total Lost response Persistent negative 20 0 Transient negative 18 4 Positive 32 15 0.0 0 24 48 72 96 120 144 MONTHS FROM FIRST CR Kantarjian et al. Cancer 2003; 97: 1033 168 192 216 Survival in Early Chronic Phase CML TKI Interferon Chemotherapy Kantarjian et al. Blood 2012; 119: 1981-7. Reproduced with permission of AMERICAN SOCIETY OF HEMATOLOGY. Is The Outcome Really That Good? MDACC event: progression to AP/ BP; loss of MCyR; loss of CHR; no response (ELN criteria); intolerance; or death (any cause, any time) Kantarjian et al. ASH 2010; Abstract 672. Or Is It Really That Bad? • 281 pts Rx with imatinib as initial therapy (73 SD, 208 HD) • CCyR 88% 75 stopped IM – 41 events 23 received subsequent TKI 14 (67%) CCyR 1.0 CEFS at 7 yrs = 88% Probability (%) 0.8 EFS at 7 yrs = 81% 0.6 0.4 0.2 0.0 0 12 Al-Kali et al. Cancer 2011; 117: 327-35 24 36 48 60 72 84 CEFS = Current event free survival; EFS = Event free survival Good Outcome: Just in Clinical Trials? • 65 pts treated off protocol & 71 on protocols • Imatinib 400 mg; Median f/u 51 mo Age, y High-risk Sokal 3-mo MCyR 12- mo CCyR 12-mo MMR 5-yr EFS 5-yr TFS 5-yr OS Median income, $ Education HS or less Uninsured Yilmaz et al. ASH 2012; Abstract #1693 Median [range], or Percentage On protocol Off protocol US Population 49 [15-79] 49 [15-84] 6 5 71 69 84 83 30 24 86 84 96 94 90 96 45,735 44,606 42,148 42 43 48 10 8 14 Clinical Case Discussions Case 1: Frontline Therapy in Newly Diagnosed Setting Case 1: History & Presentation • 37 year old male, manufacturing employee at a mechanical shop. Married with two children. • Presented with noted weight loss of 22 pounds in the last 12 months, with simultaneous onset of night sweats and fullness in the left side of his abdomen. • This patient did not have a PCP and had not been seen by a physician since his childhood days for routine checkups. Case 1: Work-up • The major clinical finding was splenomegaly at 14 cm below the costal margin. • Laboratory tests revealed: – WBC of 317,000/ml with 47% immature myeloid cells (meta myelocytes, myelocytes, promyelocytes) – 3% blast cells and 7% basophils in the peripherial blood – Blood chemistries were abnormal with elevated lactated dehydrogenase of 842 u/L – Platelet count was 916,000 – Hemoglobin was 9.3 – Other blood chemistries were WNL. Case 1 (continued) • CML is suspected and a test for bcr-abl revealed that the disease was bcr-abl positive leukemia with b3 a2 transcript consistent with CML. • A bone marrow test followed and revealed bone marrow with high cellularity of 100% with predominant but well matured myeloid series. The bone marrow had 4% myeloblasts • Bone marrow cytogenetic test revealed 20/20 cells with Ph+ and no evidence of additional chromosomal abnormalities was noted. • With the diagnosis of CML in the chronic phase the patient was placed on imatinib 400 mg daily. Case 1: Question 1 Is this the correct treatment decision? 1. Imatinib is approved as first line treatment for CML and it is the correct choice 2. The patient has high risk CML and he would have benefited from starting nilotinib or dasatinib 3. With high-risk disease the patient should have been placed on ponatinib 4. All are correct 5. Only 1 & 2 are correct 6. Only 2 & 3 are correct Case 1: Answer Is this the correct treatment decision? 1. Imatinib is approved as first line treatment for CML and it is the correct choice 2. The patient has high risk CML and he would have benefited from starting nilotinib or dasatinib 3. With high-risk disease the patient should have been placed on ponatinib 4. All are correct 5. Only 1 & 2 are correct 6. Only 2 & 3 are correct IRIS 8-Year Update No CCyR 17% Safety 5% Sustained CCyR on study 53% Lost CCyR 15% Lostregained CCyR 3% At least 37% Unacceptable Outcome CCyR Other 7% • EFS = 81%; Freedom from progression to AP/BC = 92%; OS = 85% Deininger M, et al. Blood . 2009;114(22): 1126. Imatinib Toxicities Imatinib: Common or Frequent Complaints Neutropenia Musculoskeletal complaints Thrombocytopenia – mainly during yr 1 Hypophosphatemia GI disturbances / Diarrhea Rash Edema and fluid retention Pediatrics: growth retardation Occasional bone mineral metabolism problem Long Term Toxicities of Imatinib Liver, kidney, cardiac toxicity and immunosuppression. CHF: • 1276 patients at MDACC were studied with median follow up at 47 mos • 22 patients, or 1.7% have CHF, however 13/22 had received cardio toxic drugs in the past. Management of Acute Toxicities Management of anemia and neutropenia includes use of erythropoietin and filgrastim Atallah et al, Blood 2007; 110: 1233–1237; Gleevec prescribing information, 2013.; NCCN Guidelines v4.2013. ENESTnd 3-year update: OS and PFS OS 3-yr OS, % HR (95% CI) vs imatinib P value vs imatinib PFS 3-yr PFS, % HR (95% CI) vs imatinib P value vs imatinib Nilotinib 300 mg BID (n = 282) Nilotinib 400 mg BID (n = 281) Imatinib 400 mg QD (n = 283) 95.1 97.0 94.0 0.75 (0.37-1.55) 0.46 (0.20-1.07) -- .4413 .0639 -- Nilotinib 300 mg BID (n = 282) Nilotinib 400 mg BID (n = 281) Imatinib 400 mg QD (n = 283) 96.9 98.3 94.7 0.44 (0.17–1.15) 0.30 (0.10–0.92) -- . 0.0842 0.0260 -- BID, twice daily; CI, confidence interval; HR, hazard ratio; OS, overall survival; PFS, progressionfree survival; QD, once daily. Larson RA, et al. Leukemia 2012; 26: 2197-2203.; Kantarjian et al , ASH 2012 Abstract 1676. ENESTnd 3-yr Update Nilotinib 300 mg BID (n = 282) Nilotinib 400 mg BID (n = 281) Imatinib 400 mg QD (n = 283) MMR 73; P < .0001 70; P < .0001 53 MR4 50; P < .0001 44; P < .0001 26 MR4.5 32; P < .0001 28; P = .0003 15 (Larson et al 2012, Leukemia 2197-2203.) Response by 3 yrs, % 3-mo landmark analysis: BCR-ABL transcript levels*, % MMR by 1 yr/2 yrs, % ≤ 1% (n = 120, 123, 41) 76/89 72/91 > 1 to ≤ 10% (n = 89, 95, 133) 40/67 38/54 > 10% (n = 24, 28, 88) 4/29 14/29 Freedom from progression to AP/BC, % 71/78 31/52 2/20 Estimated 3-yr rate on core treatment 99.3; P = .0059 98.7; P = .0185 95.2 Including events after discontinuation OS, % 96.7; P = .0496 98.1; P = .0076 93.5 95.1; P = .4413 97.0; P = .0639 94.0 98.1; P = .0356 98.5; P = .0159 95.2 11 3 11 2 21 3 Estimated 3-yr OS rate Only CML-related deaths Patients with BCR-ABL mutation, n Any mutation T315I ENESTnd 3-Yr Update Hematologic AEs and Biochemical Abnormalities Grade 3/4 AEs, % Nilotinib 300 mg BID Nilotinib 400 mg BID (n = 279) (n = 277) Imatinib 400 mg QD (n = 280) Neutropenia 11.8 10.8 21.4 Thrombocytopenia 10.4 12.3 8.9 Anemia 3.9 4.7 5.7 Lipase increase 7.5 7.9 3.9 ALT increase 4.3 9.4 2.5 Total bilirubin increase 3.9 7.9 0.4 Hyperglycemia 6.1 5.4 0 Nilotinib Toxicities • Prolongation of QTC and vascular adverse events • Coronary events • Peripheral Arterial Occlusive Disease – PAOD Larson RA, et al. Leukemia 2012;26; Tasigna prescribing information, 2013; NCCN Guidelines v4.2013. DASISION 3-Yr Update Cumulative Molecular Responses Outcome, % Dasatinib 100 mg QD (n = 259) Imatinib 400 mg QD (n = 260) 1 yr 46* 23 2 yrs 64* 46 3 yrs 68* 55 Cumulative MR4 3 yrs 35† 22 Cumulative MR4.5 3 yrs 22‡ 12 Cumulative MMR *P < .0001 vs imatinib. †P = .00635 vs imatinib. ‡P = .00069 vs imatinib. OS and PFS 3-Yr Survival Outcome Dasatinib (n = 259) Imatinib (n = 260) HR (95% CI) PFS, % 91.0 90.9 1.00 (0.55-1.80) OS, % 93.7 93.2 0.86 (0.45-1.65) 17 20 - Deaths, n Hochhaus A, et al. ASCO 2012. Abstract 6504. DASISION 3-Yr Update Hematologic AEs and Biochemical Abnormalities Grade 3/4 AEs, % Toxicities Dasatinib 100 mg BID (n = 281) Imatinib 400 mg QD (n = 283) Neutropenia 24.0 20.9 Thrombocytopenia 19.4 11.2 Anemia 11.6 8.5 Decreased phosphorus 7.0 28.3 Decreased calcium 3.1 1.9 Elevated creatinine 1.2 0.8 Elevated total bilirubin 1.2 0 Elevated ALT 0.4 1.6 Elevated AST 0.4 1.2 0 2.3 Decreased potassium • Impaired platelet aggregation and bleeding • Pleural effusion (up to 29% of pts) • Reversible pulmonary arterial HTN • Dose interruption in 83% of pts • Dose reduction in 71% of pts Hochhaus A, et al. ASCO 2012. Abstract 6504; Sprycel Prescribing information 2013; NCCN Guidelines v4.2013. Case 1 (continued) • The patient responded rapidly to imatinib with resolution of his symptoms: weight gain and splenomegaly. • The WBC returned to normal as did the platelet count, and the anemia resolved. • Repeat quantitative bcr-abl test after 3 months of treatment revealed bcr-abl/abl ratio by international scale of 11%. • A FISH test for bcr-abl was 22% positive. • With these improved results the physician elected to continue imatinib at 400 mg daily. NCCN Guidelines v4.2013 Case 1: Question 2 Is continuation of imatinib an appropriate option? 1. No, the patient failed to achieve a bcr-abl/abl ratio of <10% and should be a candidate for allogeneic bone marrow transplant. 2. It is the correct treatment. The patient has achieved a hematologic response and a partial cytogenetic response 3. The response is inadequate and the patient should have been switched to a 2nd generation TKI inhibitor, either nilotinib or dasatinib 4. A mutation analysis should have been performed first and if there was no bcr-abl mutation, then the decision to continue with the same treatment could have been made NCCN Guidelines v4.2013 Case 1: Answer Is continuation of imatinib an appropriate option? 1. No, the patient failed to achieve a bcr-abl/abl ratio of <10% and should be a candidate for allogeneic bone marrow transplant. 2. It is the correct treatment. The patient has achieved a hematologic response and a partial cytogenetic response 3. The response is inadequate and the patient should have been switched to a 2nd generation TKI inhibitor, either nilotinib or dasatinib 4. A mutation analysis should have been performed first and if there was no bcr-abl mutation, then the decision to continue with the same treatment could have been made NCCN Guidelines v4.2013 Case 1 (continued) • After six months of therapy the patient started to complain of worsening diarrhea – up to 6x daily, poorly controlled with Imodium. • The patient states that it has been embarrassing at times because of an inability to control it and that it is interfering with his work and social activities. • At this juncture the hematologist lowered the imatinib to 200 mg daily Adverse Event Management: Diarrhea • Imatinib’s most frequently reported drug-related adverse events were edema, nausea and vomiting, muscle cramps, musculoskeletal pain, diarrhea and rash • Important to listen to patients and acknowledge that diarrhea can be debilitating and may seriously affect their daily activities. • Physicians should discuss diet and explain to patients that certain foods, like spicy ones, can worsen diarrhea. • Patients should be prescribed anti-diarrheal medications as needed. • TKI dosage should be adjusted accordingly. Gleevec prescribing information 2013; DeAngelo, 2012; Kurtin, 2010. NCCN Guidelines for CML Treatment Continuation or Change Time 3 mo. Response Recommendation Bcr/abl: ≤ 10 % Continue treatment Bcr/abl: > 10% Evaluate compliance ; Mutation Analysis; Change Therapy 12 mo. CCYR ≤ PCYR 18 mo. CCYR ≤ PCYR NCCN Guidelines v4.2013 Continue Treatment Evaluate compliance ; Mutation Analysis; Change Therapy /Evaluate for HSCT Continue Treatment Evaluate compliance ; Mutation Analysis; Change Therapy /Evaluate for HSCT Case 1: Outcome • The patient continued on imatinib 200 mg daily for an additional 9 months. • At 12 months was found to be in hematologic response and partial cytogenetic response. • Overall, he tolerated this change in treatment reasonably well and his diarrhea was moderately well controlled. Clinical Case Discussions Case 2: Relapsed/Refractory Setting Case Study 2 A 54-year old man has been receiving therapy with imatinib 400 mg daily for 6 months. Cytogenetic analysis shows Philadelphia chromosome in 25% of metaphases. Question 1 How would you label this response: 1. Failure 2. Secondary resistance 3. Suboptimal response 4. Optimal response 5. Warning 6. None of the above Case Study 2: Answer How would you label this response: 1. 2. 3. 4. 5. 6. Failure Secondary resistance Suboptimal response Optimal response [ELN 2009 criteria] Warning [ELN 2013 criteria] None of the above Criteria for Failure and Suboptimal Response to Imatinib – ELN 2009 Time (mo) Failure Response Suboptimal No CgR >95% Ph+ Optimal 3 No CHR 6 No CgR >95% Ph+ >35% Ph+ 12 >35% Ph+ 1-35% Ph+ 18 ≥5% Ph+ Loss of CHR; Loss of CCgR; Mutation; CCA/Ph+ No MMR CCgR 0% Ph+ MMR Loss of MMR; Mutation Stable or improving MMR Any ≤65% Ph+ ≤35% Ph+ Acronyms: Ph = Philadelphia chromosome; CHR = complete hematologic response; CgR = cytogenetic response; MMR = major molecular response; CCgR = complete cytogenetic response; CCA = clonal chromosome abnormalities. Baccarani et al. JCO 2009; 27: 6041-51 Criteria for Failure and Suboptimal Response to Imatinib – ELN 2013 Time (mo) 3 6 12 Any Failure No CHR, and/or Ph+ >95% BCR-ABL1 >10% and/or Ph+ >35% BCR-ABL1 >1% and/or Ph+ >0% Loss of CHR Loss of CCgR Confirmed loss of MMR Mutations CCA/Ph+ Response Warning BCR-ABL1 >10%, and/or Ph+ 36-95% BCR-ABL1 1-10%, and/or Ph+ 1-35% Optimal BCR-ABL ≤10%, and/or Ph+ ≤35% BCR-ABL <1%, and/or Ph+ 0% BCR-ABL1 >0.1-1% BCR-ABL1 ≤0.1% CCA/Ph(-7, or 7q-) BCR-ABL1 ≤0.1% Acronyms: Ph = Philadelphia chromosome; CHR = complete hematologic response; CgR = cytogenetic response; MMR = major molecular response; CCgR = complete cytogenetic response; CCA = clonal chromosome abnormalities. Baccarani et al. Blood 2013; 122: 872-84. Reproduced with permission of AMERICAN SOCIETY OF HEMATOLOGY. Case Study 2: Question 2 The patient has occasional muscle cramps, and no other toxicity. Your treatment recommendation: 1. Continue therapy unchanged 2. Increase the dose of imatinib to 400mg BID 3. Change therapy to nilotinib 400mg BID 4. Change therapy to dasatinib 100mg QD 5. SCT Case Study 2: Answer The patient has occasional muscle cramps, and no other toxicity. Your treatment recommendation: 1. Continue therapy unchanged 2. Increase the dose of imatinib to 400mg BID 3. Change therapy to nilotinib 400mg BID 4. Change therapy to dasatinib 100mg QD 5. SCT Treatment Discontinuation for Frontline TKIs in CML Percentage F/U IM400 IM800 Nilotinib Dasatinib Bosutinib (mo) ENESTnd*¥ >36 38 DASISION >36 31 BELA >24 29 MDACC >36 29 29 30 37 24 18 8 * Nilotinib 300mg BID shown. ¥ Includes patients who discontinued into extension study; rates are 26% imatinib and 22% nilotinib if all excluded Alattar et al. ASH 2011; Abstract #745; Saglio et al. ASH 2011; Abstract #452; Kantarjian et al. ASCO 2011; Abstract #6510; Cortes et al. ASH 2011; Abstract #455 Factors Influencing Early Discontinuation of 2nd Generation TKI • Adverse events • Lack of efficacy • Availability of alternative options • Decrease tolerance to adverse events • Unreasonable expectations regarding toxicity • Suboptimal management of AEs • Lack of familiarity Baccarani et al. Blood 2013; 122: 872-84 Case Study 2: Question 3 The patient has been on imatinib therapy now for 48 months. He had achieved an MMR (BCR-ABL/ABL <0.1% IS) that had been sustained for the last 18 months, most recently at 0.05 at 36 months and 0.03 at 42 months. A routine follow up assessment shows a normal CBS with a BCR-ABL/ABL of 0.09. Question 3 What additional tests would you request: 1. 2. 3. 4. 5. 6. 7. 8. Obtain FISH Repeat PCR in 3 months Assess for mutations Repeat cytogenetic analysis Perform a bone marrow aspiration All of the above 1&3 3&5 Case Study 2: Answer What additional tests would you request: 1. Obtain FISH 2. Repeat PCR in 3 months 3. Assess for mutations 4. Repeat cytogenetic analysis 5. Perform a bone marrow aspiration 6. All of the above 7. 1&3 8. 3&5 Significance of KD Mutations in Patients Responding to Imatinib • 10 of 214 (5%) pts who achieved CCyR had mutation – 4 before CCyR • Median time from mutation to loss CCyR 20.7 months • Median time from detection of mutation to 2-fold PCR 12 mo • KD mutation predictive of loss of CCyR PFS by Mutation at 2 Yrs Reprinted with permission. © (2013) American Society of Clinical Oncology. All rights reserved. Khorashad, JS et al: J Clin Oncol 26(29): 4806-4813. When to Look For Mutations? Mutation analysis in 1301 pts receiving imatinib or 2nd generation TKI (GIMEMA) Clinical condition Failure No CHR @ 3 mo No CyR @ 6 mo No PCyR @ 12 mo No CCyR @ 18 mo Loss CCyR Loss CHR Suboptimal No CyR @ 3 mo No PCyR @ 6 mo No CCyR @ 12 mo No MMR @ 18 mo Loss MMR Soverini et al. ASH 2011; Abstract #112 % Positive 27 19 11 17 17 31 50 5 7 5 8 0 4 Molecular Response in CML TFS and OS by MR at 24 months Survival (%) TFS OS p=.50 Response p=.52 Total AP/BP P-value (vs. UND) 66 113 37 72 25 1 0 0 0 0 Response n/a .25 .38 .33 .56 Time (months) Falchi et al. Am J Hematol 2013: (In press) Total Died P-value (vs. UND) 66 113 37 72 25 3 4 2 2 3 n/a .89 .94 .70 .22 Criteria for Failure and Suboptimal Response to Imatinib – ELN 2013 Time (mo) Response Failure Warning Optimal 3 No CHR, and/or Ph+ >95% BCR-ABL1 >10%, and/or Ph+ 36-95% BCR-ABL ≤10%, and/or Ph+ ≤35% 6 BCR-ABL1 >10% and/or Ph+ >35% BCR-ABL1 1-10%, and/or Ph+ 1-35% BCR-ABL <1%, and/or Ph+ 0% 12 BCR-ABL1 >1% and/or Ph+ >0% BCR-ABL1 >0.1-1% BCR-ABL1 ≤0.1% Any Loss of CHR Loss of CCgR Confirmed loss of MMR Mutations CCA/Ph+ CCA/Ph(-7, or 7q-) BCR-ABL1 ≤0.1% Baccarani et al. Blood 2013; 122: 872-84 Criteria for Failure and Suboptimal Response to Imatinib – ELN 2013 Time (mo) Response Failure Warning Optimal 3 No CHR, and/or Ph+ >95% BCR-ABL1 >10%, and/or Ph+ 36-95% BCR-ABL ≤10%, and/or Ph+ ≤35% 6 BCR-ABL1 >10% and/or Ph+ >35% BCR-ABL1 1-10%, and/or Ph+ 1-35% BCR-ABL <1%, and/or Ph+ 0% 12 BCR-ABL1 >1% and/or Ph+ >0% Any Loss of CHR Loss of CCgR Confirmed loss of MMR Mutations CCA/Ph+ CCA/Ph(-7, or 7q-) BCR-ABL1 ≤0.1% Baccarani et al. Blood 2013; 122: 872-84 Lack of MMR is not a criterionBCR-ABL1 for BCR-ABL1 >0.1-1% ≤0.1% failure; confirmed loss of MMR is Criteria for Failure and Suboptimal Response to Imatinib – ELN 2013 Time (mo) Response Failure Warning Optimal 3 No CHR, and/or Ph+ >95% BCR-ABL1 >10%, and/or Ph+ 36-95% BCR-ABL ≤10%, and/or Ph+ ≤35% 6 BCR-ABL1 >10% and/or Ph+ >35% BCR-ABL1 1-10%, and/or Ph+ 1-35% BCR-ABL <1%, and/or Ph+ 0% 12 BCR-ABL1 >1% and/or Ph+ >0% BCR-ABL1 >0.1-1% BCR-ABL1 ≤0.1% Any Loss of CHR Loss of CCgR Confirmed loss of MMR Mutations CCA/Ph+ CCA/Ph(-7, or 7q-) BCR-ABL1 ≤0.1% Baccarani et al. Blood 2013; 122: 872-84 Case Study 2: Question 4 Six years after the start of therapy, on a routine follow-up assessment you find the BCR-ABL/ABL has increased to 27.3% (IS). You perform a bone marrow and confirm that the patient is still in chronic phase but has 75% Ph+ metaphases. A mutation analysis shows a mutation F317L. Question 4 Your choice now is: 1. Increase the dose of imatinib to 400mg BID 2. Change therapy to nilotinib 400mg BID 3. Change therapy to dasatinib 100mg QD 4. Change to bosutinib 500 mg BID 5. Change to ponatinib 45 mg daily 6. Proceed to SCT Case Study 2: Answer Your choice now is: 1. 2. 3. 4. 5. 6. Increase the dose of imatinib to 400mg BID Change therapy to nilotinib 400mg BID Change therapy to dasatinib 100mg QD Change to bosutinib 500 mg BID Change to ponatinib 45 mg daily Proceed to SCT 2nd Generation TKI in CML Parameter Potency (fold vs IM) Target BCR-ABL binding Resistant mutations Mutations with intermediate sensitivity Standard dose (CP) Grade 3-4 neutropenia & thrombocytopenia Dasatinib 325 Src & Abl Active + Inactive T315I E255K/V, V299L, F317L 100mg QD Nilotinib 30 Abl Inactive T315I E255K/V, Y253F/H, Q252H, F359V 400mg BID Bosutinib 20-50 Src & ABL Intermediate T315I E255V/K, V299L, F317L 500mg QD 33% / 22% 31% / 33% 12% / 21% Pleural effusion, bleeding Bilirubin, lipase elevation Diarrhea, rash C-kit inhibition (vs imatinib) Increased Similar None PDGFR inhibition (vs imatinib) Increased Similar None Highly active Highly active Highly active Other notable toxicities Clinical activity Sprycel®, Tasigna®, Bosulif® prescribing information (2013). 2nd Generation TKI in CML CP Post-Imatinib Resistance Response Percentage Dasatinib Nilotinib Bosutinib FU (mo) >24 >24 24* CHR 89 77 86 MCyR 59 56 54 CCyR 44 41 41 24 mo PFS** 80% 64% 79% 24 mo OS** 91% 87% 92% * Median ** All patients Shah et al. Haematologica 2010; 95: 232-40; Kantarjian et al. Blood 2011; 117: 1141-45; Cortes et al. Blood 2011; 118; 4567-76 2nd Generation TKI in CML CP Post-Imatinib Intolerance Percentage Response Dasatinib Nilotinib Bosutinib CHR 100 NR 85 MCyR 77 66 49 CCyR 67 51 41 Shah et al. Haematologica 2010; 95: 232-40; Kantarjian et al. Blood 2011; 117: 1141-45; Cortes et al. Blood 2011; 118; 4567-76 2nd-Generation TKI in CML CP Post- Imatinib Failure Toxicity Pleural effusion Liver Dasatinib ++ + Nilotinib + Bosutinib + + + ++ + ++ + ++ Diarrhea Lipase Glucose - (+) - ++ ++ ++ - Hypophosphatemia ++ ++ + Bleeding QTc + ++ ++ - Transaminases Bilirubin Rash 2nd-Generation TKI in CML CP Post- Imatinib Failure Toxicity Dasatinib Nilotinib Bosutinib Anemia 13 11 13 Neutropenia 35 31 18 Thrombocytopenia 23 30 24 Shah et al. Haematologica 2010; 95: 232-40; Kantarjian et al. Blood 2011; 117: 1141-45; Cortes et al. Blood 2011; 118; 4567-76 Sensitivity of Mutations to TKI IC50-fold increase (WT=1) WT L248V G250E Q252H Y253F E255K E255V D276G E279K V299L T315I F317L M351T F359V L384M H396P H396R G398R F486S Imatinib 1 3.54 6.86 1.39 3.58 6.02 16.99 2.18 3.55 1.54 17.50 2.60 1.76 2.86 1.28 2.43 3.91 0.35 8.10 Highly Resistant / Resistant / Sensitive Bosutinib 1 2.97 4.31 0.31 0.96 9.47 5.53 0.60 0.95 26.10 45.42 2.42 0.70 0.93 0.47 0.43 0.81 1.16 2.31 Dasatinib 1 5.11 4.45 3.05 1.58 5.61 3.44 1.44 1.64 8.65 75.03 4.46 0.88 1.49 2.21 1.07 1.63 0.69 3.04 Nilotinib 1 2.80 4.56 2.64 3.23 6.69 10.31 2.00 2.05 1.34 39.41 2.22 0.44 5.16 2.33 2.41 3.10 0.49 1.85 Redaelli et al. JCO 2009; 27: 469-71 CCyR by Mutations in CML Treated with 2nd Generation TKI after IM Failure • 86/169 (51%) pts treated had mutation – CP 30/59 (51%), AP 41/71 (58%), BP 15/39 (38%) • IC50 for mutation with dasatinib, nilotinib predictive for response in CP and AP Chronic Phase Accelerated Phase Jabbour et al, Blood 2009; 114: 2037-43. . Reproduced with permission of AMERICAN SOCIETY OF HEMATOLOGY. Case Study 2: Question 5 The patient has received nilotinib for 12 months with no cytogenetic response. You elect now to: 1. 2. 3. 4. 5. 6. Continue therapy unchanged Change therapy to dasatinib 100mg QD Change therapy to bosutinib 500 mg QD Change therapy to ponatinib 45 mg QD Change to omacetaxine SCT Case Study 2: Answer The patient has received nilotinib for 12 months with no cytogenetic response. You elect now to: 1. 2. 3. 4. 5. 6. Continue therapy unchanged Change therapy to dasatinib 100mg QD Change therapy to bosutinib 500 mg QD Change therapy to ponatinib 45 mg QD Change to omacetaxine SCT Are Responses Less Than CCyR Clinically Meaningful in 2nd Line Therapy for CML? • 165 pts treated with ≥2nd line TKI after imatinib failure • Best response: CCyR 52%, PCyR 7%, mCyR 14%, CHR 14%, no response 17% Survival Survival free from transformation Overall responses % 95% C.I. % 95% C.I. CCyR 98 94-100 95 90-100 PCyR 89 71-100 73 47-100 MinCyR 85 71-100 84 69-100 CHR only 72 52-100 88 67-100 No response 67 45-100 0 NA • Responses inferior to CCyR still confer a long-term clinical benefit to patients treated with ≥2nd line TKI in CML CP compared to no response Cortes et al. Clin Lymphoma Myeloma Leuk 2011; 11: 421-6 Response to Bosutinib 3rd Line Therapy • 114 pts who failed imatinib (600mg) & dasatinib or nilotinib • Minimum 24 mo F/U Response, % CHR MCyR CCyR PCyR MMR 2-yr progression or death IM, imatinib; D, dasatinib; NI, nilotinib. Khoury et al. ASH 2012; Abstract #3785 IM + D resistant (n = 37) 62 33 19 14 3 IM + D intolerant (n = 49) 80 48 43 5 25 IM + NI resistant (n = 27) 76 39 27 12 11 21 12 49 Ponatinib Phase 2 Study - PACE Response Characteristics CP-CML • 93% failed ≥2 TKI, 58% failed ≥3 TKI Response Rate, n (%) Any Cytogenetic Response MCyR CCyR MMR MR4.5 BCR-ABL ≤10% at 3 months, n/N(%) 1 prior approved TKI Median Time to Response*, months [range] MCyR MMR • 91% MCyR sustained at 12 months (K-M) Cortes et al. ASH 2012; Abstract #163 N=267 180 (67) 149 (56) 124 (46) 91 (34) 39 (15) 142/240 (59) 14/16 (88) 2.8 [1.6 – 11.3] 5.5 [1.8 – 19.2] Omacetaxine for CML CP After Failure to ≥2 TKI • 122 pts with CML CP (n=81) or AP (n=41) with ≥2 prior TKI • Omacetaxine 1.25 mg/m2 BID x14d, then x7d CP N=81 Primary endpoint MCyR 20% CCyR 10% Median duration, mo 17.7 Median PFS, mo 9.6 Median OS, mo 33.9 • 11 pts (9 CP, 2 AP) ongoing response • Median 35 cycles over median 39 months • Median response duration: 14 mo CP, 24 mo AP Response, % Cortes et al. Clin Lymphoma Myeloma Leuk 2013 [Epub ahead of print] AP N=41 MaHR 27% CHR 24% 9 4.7 16 Management of Failure After TKI • Close monitoring per standard recommendations (ELN) required • Indication to change therapy when failure (not warning/suboptimal) • Mutation analysis when failure; informative in some patients • Avoid rapid succession of TKI • Manage adverse events effectively • Consider all your options Participant Post-activity Survey • Please remove the Participant Post-survey & CME Evaluation from the end of your packet • By completing both the Pre- and Post-survey forms, you will help provide benchmarks and feedback that are vital to our understanding of the effectiveness of this CME program, and will help shape future educational activities and topics Post-activity Survey • Please fill in the most appropriate answer(s) for the questions below: – Degree: MD/DO Nursing Professional PharmD Other: _____________________________ – Specialty: Oncology/Hematology Transplant specialist Internal Medicine Other: ___________ – Approximately, how many patients with CML do you treat/diagnose every month? _________ Post-activity Survey Question 1 As a result of attending the educational activity, please rate your level of confidence in treating and managing patients with CML: 1 Not confident 2 3 4 5 Expert Post-activity Survey Question 2 As a result of attending the educational activity, please rate your level of competence in individualizing treatment options for patients with CML based on patient and disease characteristics: 1 Not competent 2 3 4 5 Expert Post-activity Survey Question 3 Six years after starting imatinib, a 53-year-old patient’s BCR-ABL/ABL has increased to 27.3%. After performing a bone marrow biopsy, the patient is still in chronic phase, has 75% Ph+ metaphases and an F317L mutation. The patient receives nilotinib at 400mg for 12 months after which there is no cytogenetic response. The most suitable option for this patient would be to: a) Continue therapy unchanged b) Consider ponatinib, omacetaxine, or SCT c) Consider bosutinib or dasatinib d) None of the above, enroll in a clinical trial Post-activity Survey Question 4 A 37-year-old male was diagnosed with CML and treated with imatinib 400 mg for 12 months. He was re-evaluated and found to be in hematologic and partial cytogenetic response. Which of the following options would NOT be appropriate at this point: a) Repeat mutational analysis b) Switch therapy c) Check patient’s compliance with medications d) Continue treatment e) None of the above Post-activity Survey Question 5 Cytogenetic analysis at 6 months of a 45-year-old female patient, who received prior imatinib, shows Philadelphia chromosome in 45% of metaphases and a BCR-ABL/ABL of 0.15. According to the 2013 European LeukemiaNet recommendations for the management of CML, how would you characterize this response. a) Failure b) Warning c) Suboptimal response d) Optimal response Post-activity Survey Question 6 Which of the following treatment options can be considered for a patient who has failed imatinib and dasatinib or nilotinib: a) Omacetaxine b) Bosutinib c) Ponatinib d) Any of the above Thank you for joining us today! Please remember to turn in your evaluation form. Your participation will help shape future CME activities.