Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
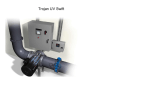
Safe water in the home: household water treatment and safe storage October 2008 Globally, poor water quality poses a major threat to human health. This leaflet has been put together to provide background information on waterborne infectious diseases and the methods which can be used in order to treat domestic water to make it, and keep it, safe for drinking during home storage. This briefing material has been produced for healthcare professions, the media and others who are looking for background understanding and/or are responsible for informing the public about infectious diseases in the home and their prevention through good hygiene practice. Poor water quality poses a major threat to human health. Globally diarrhoeal disease amounts to an estimated 4.1% of the total DALY burden of disease and is responsible for the deaths of 1.8 million people every year. The burden of disease attributable to unsafe water is mostly concentrated on children in developing countries. A significant amount of this disease could be prevented especially in developing countries through better access to safe water supply. A key argument for promoting household water treatment and safe storage in developing countries is that it can provide safe water to under-served populations much more quickly and affordably than it takes to design, install and deliver piped community supplies. Promotion of “point of use” water treatment has the potential to provide immediate benefit to at risk populations until the long-term goal of providing community water supplies can be achieved. Drinking water quality is a problem, not only in developing countries but also in developed countries, most particularly Eastern European countries, but also in North America and elsewhere. Developed countries tend to take access to safe water for granted, but situations may arise where families either intermittently (e.g. in emergencies during a breakdown in supply) or constantly (where families rely on small local water systems) where the family needs to take responsibility for purification of their water supply. How water can make you ill Diarrhoeal disease resulting from consumption of contaminated water is due to a number of waterborne pathogens including: Bacterial Cholera (Vibrio cholera) Typhoid (Salmonella typhii) Viral hepatitis A poliovirus Protozoa Cryptosporidiosis (Cryptosporidium Helminths Roundworms: Guinea worm Bacillary dysentery (Shigella spp) Campylobacter spp Salmonella spp. Escherichia coli O157 norovirus parvum) Giardiasis (Giardia lamblia) Flatworms: Contaminated water supplies have the potential to cause large and explosive epidemics of diarrhoeal disease (e.g. cholera). The non-availability of specific treatment for viral diseases such as hepatitis, and the increasing problem of antibiotic resistance, which makes bacterial diseases such as typhoid and dysentery more difficult to treat, underlines the importance of preventing water-borne disease through effective hygiene. What is the extent of the problem? Universal access to safe water is seen as an essential step in reducing the burden of infectious disease. It is estimated however, that up to 1.1 billion people still do not have access to microbiologically safe sources of water for drinking. Even for the remaining 5.2 billion people who have access to an “improved water source”, a significant proportion are still drinking water which is grossly contaminated. Even in the European region it is estimated that 120 million people do not have access to safe drinking water. Obtaining reliable data on the extent of diarrhoeal illness, the causative organisms, and the extent to which this illness is water-borne is difficult. Although mortality from diarrhoeal disease in developing countries has declined, there is little change in morbidity rates compared with previously described incidences. It is estimated that residents of developing nations may experience between 5 and 20 episodes of diarrhoea per year whilst residents of developed countries experience 1 episode of diarrhoeal illness every 2 years. In European countries and North America, there are now fewer risks of epidemics from water contaminated with pathogens such as cholera and typhoid or viral hepatitis, but a significant amount of disease resulting from contaminated drinking water is still reported. Even in developed countries, as much as 15-30% of community gastroenteritis may be attributable to municipal drinking water, despite state-of-the-art technology for water treatment and no conventional evidence of unacceptable microbial contamination levels. Developing countries situation Although water-borne diseases are of immense public health importance in developing countries, there is relatively little systematic data available on the overall incidence and prevalence of diarrhoeal disease in these areas, and on what proportion of this disease is water-borne. Although significant advances have been made in the provision of community water supplies, there is concern that the health gains from investment in water supply are being significantly compromised by the fact that: Many communities have access to water that is microbiologically safe when collected or when it leaves a treatment plant. However, substandard water distribution systems and intermittent water pressure often lead to the introduction of faecal contamination resulting in microbiologically contaminated water at the consumer's tap or collection point. Water can become contaminated by unsafe consumer storage and handling practices at the household level. Page 2/7 European situation In 2002, WHO published a report entitled “Water and Health in Europe”. Although water quality standards are high in most European countries, outbreaks of waterborne disease continue to occur. For 1986–1996, data from 17 countries in the European region indicated a total of 2,567,210 cases of infectious intestinal disease, 2% of which were linked to drinking water. These 17 countries (estimated population 220 million), on average, reported 233,383 cases of gastrointestinal disease per year. It appears that the number of outbreaks of waterborne diseases has been increasing in countries which have experienced recent breakdown in infrastructure, although reliable data on drinking water quality and the incidence of disease in most countries are lacking. North American situation Despite the fact that most USA citizens expect to have low cost, high quality water available in their domestic water tap, waterborne disease outbreaks still occur. Over the periods 1999-2000 and 2001-2002 respectively 36 outbreaks (2068 cases) and 20 (1020 cases) of waterborne infectious diseases were reported. In the USA most of the population receive their water from community systems, but these vary considerably in the number of people they serve. A particular problem in the USA arises from “small water systems” (i.e. systems serving 10,000 or fewer people). The infectious disease risk from contaminated water is considered to be greater for the water supplies of smaller communities than the larger ones. Small communities face the greatest difficulties in supplying water of adequate quality and quantity because they have small customer bases and often lack the resources needed to maintain and upgrade facilities. Small water systems are also less likely to be adequately chlorinated and routinely monitored for contaminants. Interruptions in supply as well as violations of drinking water standards are problems for some of these systems. Treating water in the home to make it safe for drinking A range of different simple, low-cost physical and chemical treatment methods have been developed which can be used to improve household water quality. Systems which make use of two or more treatments in combination or in succession as a means of optimising water quality are also available. 1. Chemical disinfection Where chlorine or iodine tablets are available, they should be used as directed by the manufacturer. Alternatively water should be disinfected with hypochlorite in the form of bleaching powder or hypochlorite solution for 30 mins. The final concentration of chlorine should be 0.5-1mgm/l available chlorine after 30 mins. The amount of chlorine needed depends mainly on the concentration of organic matter in the water and should ideally be determined for each situation using a test kit. If this is not available, a slight smell of chlorine is a crude indicator. For more details on preparing chlorine solutions consult: http://www.who.int/household_water/resources/emergencies.pdf Page 3/7 For disinfection with iodine a concentration of 3.7 mg/l, contact time 10 mins, is required (6.3 mg/l if virucidal contamination is suspected). 2. Boiling Bringing water to a rolling boil will kill pathogens effectively except at high altitudes. A holding period of 3-5 mins will ensure that water is safe, except in situations where contamination with spore-forming bacteria, fungal or protozoal cysts or hepatitis virus is suspected, in which case 10 mins is advised. 3. Filtration Ceramic filters with small pores, often coated with silver, have been shown to be effective at removing microbes and other suspended solids. Filters need to be cleaned regularly to avoid them becoming reservoirs of micro-organisms. Monthly maintenance involves scrubbing the filter to unclog pores and washing the receptacle tank and spigot. If properly maintained, they have a long life. For further information, see www.potpaz.org/ or www.purifier.com.np. 4. Solar disinfection Solar disinfection is an effective method, especially when no chemical disinfectants are available. Ultra-violet rays from the sun inactivate pathogens present in water. Water should be filled to three quarters full in clear plastic bottles and shaken thoroughly 20 times, before being filled completely. Bottles are then exposed to sunlight (e.g. on the roof of a house) for 6 hours (or for 2 days if the days are cloudy). The water should be consumed directly from the bottle or transferred to a clean glass for drinking. To be effective, solar disinfection must be applied to relatively clear water. For further information, see www.sodis.ch or www.who.int/water_sanitation_heal th/dwq/wsh0207/en/. 5. UV irradiation UV light has received renewed interest following the realisation that Cryptosporidium or Giardia cysts are relatively resistant to chlorination but sensitive to quite low (<10mJ/cm2) doses of UV. Most small scale (community or household) UV systems use low pressure Mercury lamps which provide UV at 254nm wavelength. UV systems may be batch or flow-though and the lamps can be suspended above the water channel or submerged in the water flow. 6. Combined floculation/disinfection systems Commercially produced sachets of powder are available which act by coagulating and flocculating sediments in water followed by a timed release of chlorine. These typically treat 10l of water. The water is normally stirred for few minutes, strained, and allowed to stand for a half hour. 7. Multibarrier methods Systems which use of two or more of the above treatment in combination or in succession as a means of optimising water quality are now available. Page 4/7 Pre-treatment of turbid water If water is turbid it must be pre-treated before disinfection. Water can be treated by a number of methods. The "best" option should be selected according to what is most applicable to the community in question. Turbid water can be clarified by filtration through a cotton cloth to remove any solid materials, treated with alum and bleaching powder, stored for at least 2h and then decanted or filtered through a clean cloth. For pre-treatment add 10g alum and 5g lime per 100l of turbid water. The "best" option for treatment of contaminated water should be selected according to what is most applicable and acceptable to the community in question. The following is an assessment of the relative characteristics of the various systems: Treatment Availability & Technical practicality difficulty Cost Microbial efficacy Boiling at 100ºC high* low-moderate varies high chemical treatment high(chlorine or iodine) moderate low-moderate moderate high** solar disinfection high*** low-moderate low moderate UV lamp treatment varies**** low-moderate moderate to high high coagulation/flocculation /sedimentation/filtration varies low-moderate varies varies *provided a fuel source is available; **Cryptosporidium (and to a lesser extent Giardia) are resistant; *** requires 6h exposure time, difficult to treat large volumes; ****requires a power source For further advice on treatment of water consult: Emergency treatment of drinking water at point-of-use. WHO technical note for emergencies No. 5 http://www.who.int/water_sanitation_health/hygiene/envsan/tn05/en/index.html Household Water Treatment and Safe Storage Following Emergencies and Disasters http://www.who.int/household_water/resources/emergencies.pdf Keeping water clean in the home Even in communities where an adequate supply of microbiologically safe water is available, this water can become contaminated by unsafe consumer storage and handling practices at the household level: For those in rural and peri-urban areas, who do not have piped water in the home, water has to be collected from the community supply and stored in jars, buckets or other vessels in the home. Many people continue to obtain their water on a daily or other frequent basis from any available source and either carry it or otherwise have it delivered to the home for personal use. For communities where the municipal water supply is intermittent, water has to be stored for significant periods in the home in a container or tank of sufficient size. The municipal water distribution system, is often faecally contaminated during non-supply hours, due to leaky pipelines and sewerage system. In such homes Page 5/7 the water may be stored in a tank which is specifically reserved for the purpose of water storage, or e.g. in the family bath. Collection, storage and handling of drinking water in the home, is one of the major risk areas in respect of domestic hygiene in most developing countries. Water storage vessels and water handling in the home Repeated hand contact with drinking water, during collection and storage is a major health concern: Water is often taken from these containers by dipping hands into the water which may be contaminated with faecal pathogens. If the container is not kept covered, the water may become contaminated from flies, cockroaches or domestic animals. Domestic vessels for storing drinking water: should be made of stainless steel/porcelain/glass/burnt clay and should be designed with a narrow neck and provided with a tap at the bottom so that hand contact is not required. should always be emptied and rinsed with clean water before refilling. Cleaning and disinfection of drinking water storage tanks in the home Water storage tanks in the home must be kept clean because pathogens can sometimes become established and form a permanent reservoir. Large scale water storage tanks must be emptied and cleaned, preferably once a month, or at least every 2-3 months. This should be done by cleaning and descaling to remove any biological growth from the water contact surface followed by disinfection by superchlorination. For disinfection of drinking water contact surfaces, the container should be filled with a solution containing 20-50 mg/l available chlorine for a contact period of 10-24 hrs. IFH Guidelines and Training Resources on Home Hygiene 1. Guidelines for prevention of infection and cross infection the domestic environment. International Scientific Forum on Home Hygiene. Available from: http://www.ifhhomehygiene.org/IntegratedCRD.nsf/70f1953cec47d5458025750700035d86/92111 ae38986bfbb802574dd003fc2c1?OpenDocument 2. Recommendations for selection of suitable hygiene procedures for use in the domestic environment. International Scientific Forum on Home Hygiene. Available from: http://www.ifhhomehygiene.org/IntegratedCRD.nsf/70f1953cec47d5458025750700035d86/24401 f935e57e79e802574e200391c43?OpenDocument 3. Guidelines for prevention of infection and cross infection the domestic environment: focus on issues in developing countries. International Scientific Forum on Home Hygiene. Available from: http://www.ifhhomehygiene.org/IntegratedCRD.nsf/70f1953cec47d5458025750700035d86/24eb0 6345354d067802574e1005a075d?OpenDocument 4. Home Hygiene - prevention of infection at home: a training resource for carers and their trainers. International Scientific Forum on Home Hygiene. Available from: http://www.ifhPage 6/7 homehygiene.org/IntegratedCRD.nsf/571fd4bd2ff8f2118025750700031676/9aaaeb 306bb3c50c80257522004b4fdc?OpenDocument 5. Home Hygiene in Developing Countries: Prevention of Infection in the Home and Peridomestic Setting. A training resource for teachers and community health professionals in developing countries. International Scientific Forum on Home Hygiene. Available from: http://www.ifhhomehygiene.org/IntegratedCRD.nsf/571fd4bd2ff8f2118025750700031676/19155a b46073e67f8025752200546d83?OpenDocument Further Information 1. Combatting waterborbe disease at the household level . World health Organisation 2007http://www.who.int/water_sanitation_health/publications/combating_diseas epart1lowres.pdf 2. Household water storage, handling and point-of-use treatment. 2005, A review commissioned by the International Scientific Forum on Home Hygiene. http://www.ifhhomehygiene.org/IntegratedCRD.nsf/a639aacb2d462a2180257506004d35db/aa885658ec 1f19ee8025752200559653?OpenDocument . 3. The changing hygiene climate: a review of infectious disease in the home and community. International Scientific Forum on Home Hygiene. www.ifhhomehygiene.org/IntegratedCRD.nsf/111e68ea0824afe1802575070003f039/29858aa00 6faaa22802572970064b6e8?OpenDocument 4. The World Health Report 2004; Geneva: World Health Organisation. 5. Meeting the MDG Drinking Water and Sanitation Target, A Mid-Term Assessment of Progress 2004; World Health Organisation: Geneva. http://www.who.int/water_sanitation_health/monitoring/jmp04.pdf. 6. Sobsey, MD. Managing water in the home: accelerated gains from improved water supply. 2002 World Health Organization, Geneva: WHO/SDE/WSH/ 02.07. 7. Bartram J, Thyssen N, Gowers A, Pond K, Lack T, eds. Water and health in Europe: a joint report from the European Environment Agency and the WHO Regional Office for Europe (2002). WHO Regional Publications, European Series No. 93. 8. Anon 2002. Surveillance for water-borne-disease outbreaks with drinking water – United States, 1999–2000. Morbidity and Mortality Weekly Report 2002;51:128. 9. Anon 2004. Surveillance for water-borne-disease outbreaks associated with drinking water – United States, 2001–2002. Morbidity and Mortality Weekly Report 2004;53:23-45. 10. Safe Water from every tap: Improving water service to small communities.1996. National Research Council. National Academy Press, Washington DC. 11. US Environmental Protection Agency 1997 National Public Water Systems Annual Compliance Report and update on implementation of the 1996 Safe Drinking Water Act amendments. August 18th 1997. Page 7/7