Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
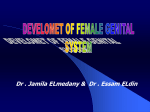
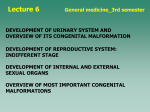
Lecture 7: Urogenital System Slide 1: Title slide: Urogenital System Main points: Covers Chapter 15 Slide 2: Cross section showing parts of the mesoderm Main points: 1. There are three parts to the mesoderm: paraxial, intermediate, and lateral plate. 2. Most of the urinary and genital systems develop from the intermediate mesoderm. Slide 3: Scanning electron micrograph of a cross section showing the parts of the mesoderm Slide 4: Illustration showing three kidney systems Main points: 1. Three kidney systems form: the pronephros, mesonephros, and metanephros. These three systems represent evolutionary development from lower to higher vertebrate species—an example of ontogeny recapitulating phylogeny. 2. These systems form in the intermediate mesoderm that extends from cervical to pelvic regions along the posterior wall. 3. Pronephros: segmented, forms in the cervical regions, rudimentary, barely develops with little or no significance. 4. Mesonephros: unsegmented, forms in thoracic and upper lumbar regions, may function briefly, consists of filtration units and a duct, degenerates almost completely in females, but contributes to the duct work of the male reproductive system. 5. Metanephros: definitive kidney system, forms in the pelvic region, begins functioning in the 10th to 12th weeks. 6. All three systems are never present at the same time. Thus, as the pronephros starts to degenerates (fourth week), the mesonephros is forming (fourth to sixth weeks), and as it starts to disappear, the metanephros is forming (fifth week). Slide 5: Illustrations showing the urogenital ridge Main points: 1. In the lumbar region, the gonads develop from a proliferation of mesoderm and overlying epithelium. Together the gonads and mesonephros form the urogenital ridge. Note that this ridge is retroperitoneal (covered by peritoneum only on its anterior surface). 2. Excretory tubules form in the mesonephros and differentiate into Bowman’s capsule around a tuft of capillaries called the glomerulus. This is the filtration region for the kidney. Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013 3. The filtration units (Bowman’s capsule plus glomerulus) together with the excretory tubules constitute a nephron, the functional unit of the kidney. 4. Two ducts form by pinching off of the epithelium: mesonephric (wolfian) and paramesonephric (müllerian) ducts. Both ducts enter into the anterior portion of the cloaca that will form the urogenital sinus. 5. The mesonephric duct is the collecting duct for the mesonephric kidney and will contribute to the male reproductive ducts. 6. The paramesonephric duct parallels the mesonephric duct and contributes to the female reproductive system. Slide 6: Illustration showing formation of the metanephric kidney Main points: 1. The ureteric bud grows off the caudal end of the mesonephric duct and into intermediate mesoderm (the metanephric blastema) in the pelvic region. 2. The bud is responsible for inducing the mesoderm to form the kidney. Slide 7: Differentiation of the ureteric bud Main points: 1. The ureteric bud forms the collecting system for the definitive kidney. 2. The ureteric bud lengthens and then starts to divide, eventually forming the renal pelvis, major and minor calyces, and collecting tubules for the definitive kidney. Slide 8: Slide showing formation of nephrons Main points: 1. As the ureteric bud branches in the metanephric blastema, it induces this mesoderm to form filtration units (nephrons). 2. Thus, tubules form that eventually develop into Bowman’s capsules around the glomeruli and proximal and distal convoluted tubules and Henle’s loops. 3. In turn, these filtration units hook up with the collecting ducts developing from the ureteric bud via the distal convoluted tubules. Slide 9: Illustration showing molecular regulation of kidney development Main points: 1. Kidney induction represents another epithelial-mesenchymal interaction: Epithelium of the ureteric bud interacting with intermediate mesoderm of the metanephric blastema. 2. WT1 is expressed in the mesoderm, making it competent to respond to induction by the ureteric bud. 3. WT1 regulates production of glial-derived neurotrophic factor (GDNF) and hepatocyte growth factor (HGF), which cause the bud to branch. In turn, the bud secretes fibroblast growth factor 2 (FGF2) and bone morphogenetic protein 7 (BMP7), which stimulate growth of the mesoderm. 4. Tubule formation in the mesoderm is regulated by WNT9B and WNT6 secreted by the buds that cause expression of PAX2 and WNT4 in the Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013 mesoderm. PAX2 causes the mesoderm to condense, and WNT4 causes the condensations to differentiate into epithelial cells and form tubules. 5. The bottom line is that WT1 is the master gene for kidney development, and mutations in this gene are responsible for Wilms’ tumor, a cancerous tumor common in childhood. 6. If induction fails, the result is renal agenesis, and the fetus presents with Potter sequence. There is oligohydramnios (too little amniotic fluid) because the fetus drinks but cannot excrete, which results in compression of the uterine cavity and, consequently, the fetus. This causes the baby to have a flattened face, beak-like nose, and club feet. These fetuses are stillborn or die shortly after birth due to the absence of the kidneys. Slide 10: Illustration showing the early location of the kidneys in the pelvis Main points: 1. Kidneys are initially formed in the pelvic region and are said to “ascend” into their definitive location in the lumbar area. Slide 11: Illustrations showing ascent of the kidneys from the pelvic region Main points: 1. Kidneys ascend from the pelvis to the lumbar region. 2. This is mostly a passive process created by growth of the caudal region of the embryo while the kidneys are held in their original positions. Slide 12: Examples of pelvic and horseshoe kidneys Main points: 1. Sometimes a kidney sticks in the pelvis during caudal growth of the embryo and fails to ascend, resulting in a pelvic kidney. 2. During their early development in the pelvis, the kidneys are in close proximity, and sometimes their tissues fuse. The result is a horseshoe kidney that is blocked in its ascent by the inferior mesenteric artery. Slide 13: Examples of congenital polycystic kidneys Main points: 1. Autosomal recessive form: Cysts arise from collecting tubules, and renal failure usually occurs in childhood. 2. Autosomal dominant form: More common than recessive form, with cysts arising from all regions of the nephrons, but the disease is less severe than the recessive form. Renal failure usually occurs in adulthood. Slide 14: Examples of duplication defects in the ureters Main points: 1. Complete and partial duplications may occur. 2. They are not usually symptomatic but may make it more difficult to pass kidney stones. Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013 Slide 15: Illustrations showing formation of the hindgut and bladder Main points: 1. Initially, both the urinary system and the gut enter into a common chamber called the cloaca. 2. Proliferation of mesoderm from the floor of the pelvis causes formation of the urorectal septum. This septum grows caudally until it completely separates the rectal canal from the anterior portion of the cloaca called the urogenital sinus. The tip of the urorectal septum forms the perineal body. 3. The upper portion of the urogenital sinus forms the bladder. 4. The allantois connects the bladder-forming region of the urogenital sinus to the umbilicus. This is a vestigial structure that, in birds, serves as a respiratory organ. It later forms a fibrous cord, the urachus, which ultimately becomes the medial umbilical ligament. 5. The caudal part of the urogenital sinus forms the urethra. Slide 16: Illustrations showing repositioning of the ureters and bladder formation Main points: 1. As the region of the urogenital sinus that forms the bladder expands, it incorporates portions of the mesonephric ducts into its posterior wall. 2. The incorporated portion of the ducts results in mesoderm contributing to the posterior bladder wall, a region called the trigone. Later endoderm will grow over this area. 3. Because the ureters are outgrowths from the mesonephric ducts, their position is altered when the mesonephric ducts are incorporated into the bladder. Thus, incorporation of the ducts causes the ureters to enter the bladder directly. 4. If the embryo is a male, the mesonephric ducts remain to form the vas deferens and ejaculatory ducts, which enter into the prostatic portion of the urethra. Notice that the vas deferens crosses over the ureters. 5. If the embryo is female, the mesonephric ducts degenerate. Slide 17: Illustration showing different locations for ectopic ureters Main points: 1. Because of the nature of bladder formation, including repositioning of the ureters, and because it develops from the urogenital sinus that contributes to formation of the vagina, it is possible to develop an ectopically positioned ureter. 2. The ureter may enter the urethra directly (a circumstance that can also occur in males) or the vagina. Slide 18: Illustration showing the final position of the ureters and vas deferens in a male Main points: 1. In the male, the mesonephric ducts differentiate into the vas deferens, and at their caudal end, the seminal vesicle forms as an outpocketing. From the Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013 point of formation of the seminal vesicle to where the duct enters the urethra, the mesonephric duct forms the ejaculatory duct. 2. The prostate forms from endodermal buds (proliferations) from the urethra. Slide 19: Illustrations showing urorectal septal defects and imperforate anus Main points: 1. If the urorectal septum fails to descend completely, the gut tube will not be separated from the urogenital portion of the cloaca, resulting in fistulas between rectum and urethra (males) or vagina. 2. If the septum is misplaced slightly anteriorly, then separation of the gut tube may occur, but it will be abnormally positioned. In this case, a fistula may develop in the perineal region. 3. Normally, the lower portion of the rectum is derived from a proliferation of ectoderm in the anal pit. If this fails, then imperforate anus results. This defect may also occur if the anal membrane fails to degenerate. (See Lecture 6: Respiratory and Digestive System Development.) Slide 20: Illustrations showing defects of the urachus Main points: 1. Normally the allantois, which connects the bladder to the umbilicus, constricts to form a fibrous cord called the urachus that then becomes the medial umbilical ligament. 2. If the allantois fails to degenerate into a cord, then a fistula between the bladder and umbilicus forms, and urine may leak from this region. 3. Cysts and sinuses represent variations on the theme. Slide 21: Illustrations showing the relationship of the gonad to the mesonephros Main points: 1. Gonadal tissue forms next to the mesonephric system and forms its own ridge, the gonadal or genital ridge. 2. In combination, the region where the gonad and mesonephros are together forms the urogenital ridge along the posterior body wall. 3. Note that the proximity of the mesonephros and gonad sets the stage for tubules and ducts from the mesonephros to play a role in conduction of sperm in the male. Slide 22: The origin and migration of germ cells Main points: 1. Germ cells are formed in yolk sac endoderm and have to migrate to the genital ridge. They do so by going along the hindgut through the dorsal mesentery and into the ridge. They start their migration in the fourth week and reach the ridge by the sixth week. 2. Some teratoma-type tumors (see sacrococcygeal tumor, Lecture 2) are thought to arise from germ cells that fail to make it to the genital ridge. Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013 Slide 23: Illustration showing the relationship of germ cells to epithelium of the genital ridge Main points: 1. Once they arrive in the genital ridge, germ cells are surrounded by epithelial cells derived from the surface of the gland. 2. Surface epithelial cells proliferate and extend into the gonad to form the primitive sex cords. Slide 24: Illustrations showing the origin of the seminiferous tubules Main points: 1. In males, primitive sex cords lose their connection to the surface of the gonad. 2. Epithelium remaining on the surface of the gland thickens to form a tough outer covering, the tunica albuginea. 3. The cords become horseshoe shaped and, at puberty, will canalize to form the seminiferous tubules. 4. Sertoli cells differentiate from some of the cells of the cords and secrete antimüllerian hormone (also called müllerian-inhibiting substance), which causes regression of the paramesonephric (müllerian) duct. Sertoli cells also serve as nurse cells for sperm development. 5. Interstitial cells (of Leydig) differentiate from mesoderm between the sex cords. These cells secrete testosterone, which causes maturation of the ducts and tubules in the male. Testosterone is converted in some tissues to dihydrotestosterone, which causes maturation of the external genitalia. 6. As the male duct system differentiates, tubules called the rete testis make connections between the seminiferous tubules and some of the old mesonephric tubules. Mesonephric tubules connected in this way form the efferent ductules that conduct sperm into the old mesonephric duct, which now forms the ductus deferens. Slide 25: Illustration showing continued development of the male ducts Main points: 1. Not all of the mesonephric tubules differentiate into efferent ductules, so the remainder degenerate, although remnants exist called the paragenital tubules. 2. Similarly, not all of the mesonephric duct is utilized to form the ductus deferens, and its remnant forms the appendix epididymis. 3. By late fetal stages, the ductus deferens has become the vas deferens. 4. The seminal vesicle forms as a proliferating outpocketing of duct epithelium near the prostate. From the point of the seminal vesicle to its opening into the prostatic urethra, this portion of the ductus deferens forms the ejaculatory duct. 5. At its proximal end, the ductus proliferates and becomes highly coiled, thereby forming the epididymis. Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013 Slide 26: Formation of oocytes and follicular cells Main points: 1. In females, the original sex cords degenerate (the medullary cords), and a second set of cords is formed near the surface of the ovary (cortical cords). 2. Follicular cells differentiate from these cortical cords and surround the germ cells that have now differentiated into oogonia. Each oogonium, with its surrounding follicular cells, forms a primary follicle. 3. By the time of birth, many of these oogonia will degenerate, and no more will form, unlike males who, once they reach puberty, produce sperm for most of the remainder of their life. Slide 27: Illustrations showing differentiation of the ducts in females Main points: 1. In females, there is no testosterone, so the mesonephric duct and tubules degenerate. Remnants of the tubules form the epoophoron and paroophoron, and a small remnant of the duct near the vagina forms Gartner’s cyst. 2. In the absence of Sertoli cells and their antimüllerian hormone, the paramesonephric ducts remain and are stimulated by estrogens. 3. The proximal end of the paramesonephric duct forms the uterine (fallopian) tube and grows finger-like projections (fimbriae) on its end near the ovary. 4. The caudal end of these ducts fuse to form the uterus and upper portion of the vagina. Interesting note: The uterine tube is open to the peritoneal cavity and ovulated eggs must be caught by the fimbriae, which become sticky and start to beat at the time the egg is ovulated. Also, eggs rupture through the ovarian epithelium directly into the peritoneal cavity during the ovulatory process. Sometimes eggs make it into the tube, become fertilized, and then fall back into the peritoneal cavity to become an ectopic pregnancy. The most common site in the peritoneal cavity for this type of ectopic pregnancy to occur is in the rectouterine (Douglas’) pouch, the lowest point in the cavity. The most common site for all ectopic pregnancies is the uterine tube (a tubal pregnancy). Slide 28: Illustrations showing formation of the broad ligament Main points: 1. The urogenital ridge grows away from the posterior wall and rotates slightly, moving the ovaries into a more transverse plane and closer toward the midline. 2. This growth causes the paramesonephric ducts to come together caudally so that they fuse and form the uterus. 3. Since the ridge is covered by peritoneum (retroperitoneal), it carries the peritoneal layer with it. Eventually this layer drapes over the ovaries and uterine tubes as the broad ligament. 4. At its cranial and caudal poles, mesoderm of the ridge thins to form the ligaments of the ovary (see next slide). Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013 Slide 29: Illustration showing the final relationship of the ovary, uterine tube, and uterus Main points: 1. Mesoderm of the urogenital ridge thins to form the suspensory ligament (attached to the posterior wall) and proper ligament (attached to the uterus) of the ovary. Slide 30: Sagittal views showing induction of the vagina by the paramesonephric ducts. Main points: 1. Paramesonephric ducts enter into the posterior wall of the urogenital sinus. Contact with the wall induces formation of the sinovaginal bulbs. 2. These bulbs grow out from the sinus as a solid group of cells that then canalize to form the lower portion of the vagina. 3. The fused paramesonephric ducts form the upper portion of the vagina and the cervix. Slide 31: Frontal views of vaginal development Main points: 1. Note that, at the site of fusion, the wall between the paramesonephric ducts has to degenerate. 2. A small amount of tissue from the posterior wall of the urogenital sinus remains as the hymen. Slide 32: Examples of abnormalities of the uterus and vagina Main points: 1. A variety of defects occur that are primarily due to problems with induction, fusion of the paramesonephric ducts, or programmed cell death patterns responsible for removal of cells. 2. In some cases, fusion may fail completely, resulting in a double vagina and uteri. 3. Occasionally, one duct fails to contact the sinus, resulting in a rudimentary horn. In this case, there is no outlet for blood once menstruation begins at puberty. Slide 33: Summary of differences between testes and ovarian development Slide 34: Summary of genetic signals for testes and ovarian development Main points: 1. In males, the sex-determining gene is called SRY (sex-determining region on the Y chromosome). With the presence of this gene, testes develop, and the fetus is male. It is the master gene for male development. 2. In females, WNT4 plays a primary role. Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013 3. Note that the two signaling pathways interact to inhibit genes in one or the other to assist with their specific patterns of development. Thus, SOX9 in males inhibits WNT4 in their system so that this “female” gene is not active. Likewise, DAX1 in females inhibits SOX9, which would normally activate the male pathway. Interesting note: Previously, females were thought to develop by default due to the absence of the SRY gene. Not surprisingly, this is not true, and modern molecular techniques have shown that there is an important signaling pathway in females just as there is in males. Slide 35: Views showing the early stages of external genitalia development Main points: 1. These early stages of development are identical in both sexes. 2. In males, testosterone is converted to dihydrotestosterone to regulate development of the external genitalia. 3. In females, absence of testosterone and the presence of estrogens regulate development of this region. 4. At 4 weeks, proliferation of mesoderm creates swellings around the cloacal membrane called the cloacal folds. Anteriorly, these folds unite to form the genital tubercle. 5. Lateral to the cloacal folds, a second pair of swellings appears called the genital swellings. 6. By the end of 6 weeks, the urorectal septum has separated the hindgut and urogenital sinus portions of the cloaca, such that the cloacal folds are divided into the urethral folds anteriorly and the anal folds posteriorly. Slide 36: Illustrations showing differentiation of male genitalia Main points: 1. In males, the genital tubercle lengthens to form the penis, and the urethral folds come together and fuse, thus forming the penile urethra. 2. The genital swellings become the scrotal swellings as they enlarge and eventually fuse to form the scrotum. The line of fusion creates the scrotal raphe. 3. The very tip of the glans is canalized by a proliferation of ectoderm that pushes inward to meet the urethra and then hollows to form an opening. Slides 37 & 38: Examples of male fetuses and genitalia development Slide 39: Examples of hypospadias Main points: 1. Hypospadias is a defect resulting from a lack of closure in fusing regions of the urethra or scrotum, creating openings that may leak urine. Interesting note: These defects are increasing in frequency, and sperm counts are declining (by 50% over the last 100 years), leading some investigators to hypothesize that estrogen-like compounds accumulating in our environment are the cause. These factors Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013 are called endocrine disruptors and are derived from waste in the environment, primarily plastics and chemicals. In some cases, plants convert these chemicals to phytoestrogens, which are then ingested. On another note, it is interesting that closure of the neural tube and the penile urethra and their closure defects are similar morphologically and may involve some of the same cellular mechanisms. Slide 40: Illustrations showing development of female external genitalia Main points: 1. Females begin at 6 weeks with the same indifferent stage as males. 2. Development in females is characterized by less growth of the genital tubercle, which becomes the clitoris, and absence of fusion between the urethral folds, which form the labia minora, and the genital swellings, which form the labia majora. 3. Once the paramesonephric ducts contact the urogenital sinus and induce formation of the vagina, openings for the vagina and urethra become separated. Slide 41: View of female fetal genitalia Main points: 1. At 11 weeks, the genital tubercle (clitoris) in female fetuses is as large as or larger than in males. Consequently, it is difficult to determine sex with ultrasounds until about the 13th week. Slide 42: Example of female pseudohermaphrodism (adrenogenital syndrome) Main points: 1. True hermaphrodites are rare and have both ovarian and testicular tissues (ovotestes). Most are 46XX and have mostly female characteristics. 2. Pseudohermaphrodites are more common and are classified as male or female based on their genotypic sex: XX female; XY male. 3. The most common form of female pseudohermaphrodism is the adrenogenital syndrome. Biochemical defects in steroid biosynthesis (usually 21 hydroxylation) result in accumulations of ACTH and ultimately androgen compounds. These androgens then stimulate the external genitalia to take on a more male-like appearance—in this case, fusion of the labia majora and enlargement of the clitoris. Slide 43: Example of male pseudohermaphrodism Main points: 1. A common cause for this type of abnormality is the androgen insensitivity syndrome. Patients are XY and have testes. However, their external genitalia lack receptors for testosterone, causing them to assume a female morphology. 2. Because testes are present, so is antimüllerian hormone; thus the paramesonephric (müllerian) ducts are inhibited, and no uterus forms. The vagina, if present at all, is short and blind ending. Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013 Slide 44: Summary of the signals for sexual differentiation Slide 45: Illustrations showing testicular descent Main points: 1. Testes develop in a retroperitoneal position in the lumbar region. Consequently, they must migrate to the scrotum and, in so doing, pass through the layers of the abdominal wall. As they pass through, each layer contributes a layer surrounding the testes. 2. During the eighth week, the urogenital ridge thins caudally to form the caudal genital ligament, which is supported by additional matrix material that condenses into the gubernaculum. 3. The gubernaculum extends from the caudal pole of each testis and eventually reaches the scrotum by passing through the inguinal canal. It assists in pulling the testes into the scrotal sac. 4. Testicular descent is preceded by an outpocketing of peritoneum called the processes vaginalis that migrates through the inguinal canal and into the scrotal sac. Once the testis arrives in the scrotum, the processes wraps around the gland, forming the visceral and parietal layers of the tunica vaginalis. 5. The testes should reach the inguinal canal by 7 months and be in the scrotum at birth. In 3% of infants, the testes do not make it but will find their way by 3 months of age. In 1%, they will remain undescended, a condition called cryptorchidism. 6. Factors regulating descent include testosterone and antimüllerian hormone (müllerian-inhibiting substance), which act on the gubernaculum. Interesting note: Testes require a lower temperature for sperm production. That is why they migrate into the scrotum, where temperature can be maintained 2-3° lower than body temperature. Slide 46: Illustration showing coverings of the testes Main points: 1. The inguinal canal is an oblique passageway through the layers of the abdominal wall; as the processes vaginalis and testes migrate through the wall, they are covered by these layers. 2. Note that the transversus abdominis muscle does not provide a covering. This results because its insertion arches over the internal ring of the inguinal canal, and so the testes do not migrate through this muscle layer. Slide 47: Examples of defects related to the processes vaginalis Main points: 1. Once the processes vaginalis reaches the scrotum, its connection to the peritoneum pinches off and closes. If closure fails, then a tract remains through which intestines may pass into the inguinal canal and sometimes all the way into the scrotum. Herniation of intestines along this pathway is called an indirect inguinal hernia. Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013 2. If the pinching off occurs abnormally, cysts may form that can fill with fluid to form hydroceles. Slide 48: Illustration showing final positioning of the ovary Main points: 1. Ovaries also descend, but not as far as testes. This descent is caused partly by growth of the urogenital ridge toward the midline, but also because the ovaries, like the testes, form a caudal genital ligament surrounded by the gubernaculum that extends to the labia majora. 2. Due to growth of the uterus, this connection between the caudal pole and labia majora is lost, and the caudal ligament attaches to the side of the uterus to form the proper ovarian ligament. 3. The part of the caudal genital ligament extending from the side of the uterus to the labia majora forms the round ligament of the uterus. 4. Sometimes the attachment of this ligament to the uterus fails to occur, and an ovary may be located in the labia majora. Interesting note: Since the ovaries do not descend, the inguinal canal in females is rudimentary, and indirect hernias are rare. Sadler, T.W.: Langman’s Medical Embryology, 12e © Lippincott Williams & Wilkins, 2013