Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
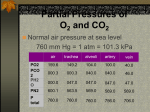
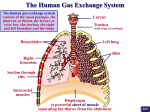
Respiratory System Physiology Dr. Amjed Hassan Al-Juboory lecture 3 Ventilation and Perfusion Ratios for Optimum Gas Exchange Ventilation/perfusion ratio is the ratio of alveolar ventilation V to perfusion (pulmonary blood flow)Q. – In healthy lungs, the V/Q ratio is close to 1:1, resulting in optimum gas pressures and oxygenation in systemic arterial blood. Distribution of V/Q Ratios There are regional differences in alveolar ventilation and blood flow in the upright individual. – Blood flow is very low at the apex of the lung and very high at the base due to the effects of gravity. The differences in regional blood flow are greater than the differences in regional ventilation. This creates different V/Q ratios at various levels of the lung. Typical values are as follows: – Apex V/Q is ~3:1. – Middle of lungs (heart level) V/Q is ~1:1. – Base of lungs V/Q is ~1:2. Gas Exchange and Transport Partial Pressures In a gas mixture, each gas species exerts a pressure, the partial pressure of that gas. The sum of the partial pressures of the gases in a mixture equals the total gas pressure. Partial pressure for an individual gas = the fraction of that gas in the gas mixture × total gas pressure Consider air, which has an approximate composition of 79 % nitrogen and 21 % oxygen. The total pressure of this mixture at sea level averages 760 mm Hg, each gas contributes to the total pressure in direct proportion to its concentration. Therefore, 79 % of the 760 mm Hg is caused by nitrogen (600 mm Hg) and 21 % by oxygen (160 mm Hg). The partial pressures of individual gases in a mixture are designated by the symbols Po2, Pco2, Pn2, and so forth. 1 Respiratory System Physiology Dr. Amjed Hassan Al-Juboory lecture 3 Gas Exchange Diffusion of Gases O2 and carbon dioxide (CO2 ) diffuse between alveolar gas and pulmonary capillary blood according to standard physical principles – The total amount moved per unit of time is proportional to the area available for diffusion and to the difference in partial pressure between alveolar gas and pulmonary capillary blood, and inversely proportional to the thickness of the diffusion barrier. – Gas will diffuse from the alveoli (higher partial pressures) to the pulmonary capillaries (lower partial pressures) until they equilibrate and no partial pressure gradient exists. As a result, blood entering the pulmonary veins from the pulmonary capillaries has virtually the same partial pressures as gases in the alveoli. The diffusion barrier (respiratory membrane) is very thin, which ensures that the diffusion distance between alveolar gas and pulmonary capillary blood is very short. This allows blood in the pulmonary capillaries to equilibrate with alveolar gas during the short time (< 1 sec) that the blood is in the capillaries. Structure of respiratory membrane Respiratory membrane is 0.2 micrometer thickness and composed of: 1) fluid (surfactant), 2) epithelium, 3) epithelial basement membrane, 4) interstitial fluid, 5) capillary basement membrane, 6) endothelial cells. The total surface area is 70 m2 and contain 60-140ml blood. The diameter of the capillary is 5micrometers (RBC is 7 micrometers), so RBC squeeze inside. 2 Respiratory System Physiology Dr. Amjed Hassan Al-Juboory lecture 3 Figure . Ultra structure of the respiratory membrane where diffusion occurs. Partial Pressure Changes of Oxygen and Carbon Dioxide Following Gas Exchange Partial Pressure Changes of Oxygen – The PO2 of humidified inspired air is 150 mm Hg. – The PO2 of alveolar air is 100 mm Hg. This is due to the diffusion of O2 from alveolar air into pulmonary capillary blood. – The PO2 of systemic arterial blood is 95 mm Hg. It is almost the same as the PO2 of alveolar air because the partial pressure of pulmonary capillary blood equilibrates with alveolar air. However, ~2% of the cardiac output bypasses the pulmonary circulation, which accounts for the slight discrepancy in partial pressures. – The PO2 of venous blood is 40 mm Hg because O2 has diffused from arterial blood into the tissues. Partial Pressure Changes of Carbon Dioxide – The PCO2 of humidified inspired air is almost zero. – The PCO2 of alveolar air is 40 mm Hg because CO2 from venous blood entering the pulmonary capillaries diffuses into alveolar air. 3 Respiratory System Physiology Dr. Amjed Hassan Al-Juboory lecture 3 – The PCO2 of systemic arterial blood is 40 mm Hg because pulmonary capillary blood equilibrates with alveolar air. – The PCO2 of venous blood is 46 mm Hg. It is higher than systemic arterial blood due to the diffusion of CO2 from the tissues into venous blood following cellular respiration. Diffusion across the alveolocapillary membrane (respiratory membrane) Gases diffuse from the alveoli to the blood in the pulmonary capillaries or vice versa across the thin alveolocapillary membrane.The diffusing capacity of the lung for a given gas is directly proportional to the surface area of the alveolocapillary membrane and inversely proportional to its thickness. The Po2 of alveolar air is normally 100 mm Hg, and the Po2 of the blood entering the pulmonary capillaries is 40 mm Hg, so O2 diffuses from alveoli into the blood, and the Po2 of blood is raised to 97 mm Hg, a value just under the alveolar Po2. The Pco2 of venous blood is 46 mm Hg, whereas that of alveolar air is 40 mm Hg, and CO2 diffuses from the blood into the alveoli along this gradient. Factors Affecting Diffusion through the Respiratory Membrane 1. Thickness of the membrane. 2. Surface area of the membrane. 3. Diffusion coefficient. 4. Difference in partial pressure. Transport of Oxygen and Carbon Dioxide in Blood and Tissue Fluids Once oxygen has diffused from the alveoli into the pulmonary blood, it is transported to the peripheral tissue capillaries almost entirely in combination with hemoglobin. The presence of hemoglobin in the red blood cells allows the blood to transport 30 to 100 times as much oxygen as could be transported in the form of dissolved oxygen in the water of the blood. In the body’s tissue cells, oxygen reacts with various foodstuffs to form large quantities of carbon dioxide. This carbon dioxide enters the tissue capillaries and is transported back to the lungs. Carbon dioxide, like 4 Respiratory System Physiology Dr. Amjed Hassan Al-Juboory lecture 3 oxygen, also combines with chemical substances in the blood that increase carbon dioxide transport 15- to 20-fold. Oxygen and Carbon Dioxide Transport in Blood Two forms of the gases: physical dissolution and chemical combination. Most of O2 and CO2 in the blood is transported in chemical combination 1.Transport of Oxygen Method Dissolved in Plasma Combined with Hemoglobin Structure Percentage 1.5 % 98.5 % Bound to Hgb Dissolved Oxygen is carried in the blood in two forms, dissolved and combined with haemoglobin (Hb) which increases oxygen carrying capacity 50x (97% of O2 in blood is transported by combining with hemoglobin and only 3% is dissolved). Partial pressure of O2 in blood leaving the lung is 95mmHg = 97% saturation and venous blood contains 40mmHg (75% saturation). Each gram of Hb binds to 1.34ml O2, so 1.34 X 15gm = 20.1ml O2 in 100% saturation. So 95 mmHg (97%) blood carries 19.4 ml O2 , while in tissues, the saturation 40% and in veins (75%) carrying 14.4ml O2 in each 100ml of blood. Hemoglobin structure Protein made up of 4 subunits, every subunit contains a heme moiety attached to a polypeptide chain. 5 Respiratory System Physiology Dr. Amjed Hassan Al-Juboory lecture 3 Basic concepts: Oxygen Capacity : The maximum quantity of oxygen that will combine chemically with the hemoglobin in a unit volume of blood Normal Value: 1.34 ml of O2 per gm of Hb or 20 ml of O2 per 100 ml of blood. Oxygen Content: how much oxygen is in the blood Oxygen Saturation: The percentage of all the available heme binding sites saturated with oxygen The oxygen-hemoglobin dissociation curve: The curve explains the relationship between oxygen levels and hemoglobin saturation in the lungs and tissues. The 'plateau' portion of the oxyhemoglobin dissociation curve is the range that exists at the pulmonary capillaries (minimal reduction of oxygen transported until the PO2 falls 50 mmHg). The 'steep' portion of the oxyhemoglobin dissociation curve is the range that exists at the systemic capillaries (a small drop in systemic capillary PO2 can result in the release of large amounts of oxygen for the metabolically active cells). In the lungs: PO2 is 95mmHg. Hb is nearly 97% saturated. Due to positive cooperativity, affinity of Hb for O2 is the highest, which corresponds to flat portion of curve. Therefore, O2 diffuses into the pulmonary capillary 6 Respiratory System Physiology Dr. Amjed Hassan Al-Juboory lecture 3 blood. The flat position of curve extends from 100mmHg to 60mmHg. This means, human can tolerate substantial decreases in alveolar PO2 to 60mmHg (e.g. caused by decreases in atmosphere pressure) without compromising the O2-carrying capacity of Hb. In the tissues: PO2 is 40mmHg. Hb is 75% saturated and the affinity for O2 is decreased. O2 is not tightly bound which facilitates unloading of O2 in the tissues. Figure: Oxygen-hemoglobin dissociation curve 7