Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
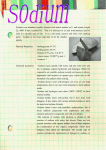
Sodium and Your Health Rebecca Burson, M.D., M.P.H. Assistant Clinical Faculty at Texas A&M FM Residency Sodium and health Discuss briefly how sodium is utilized in the body Discuss how sodium affects hypertension Discuss how sodium affects congestive heart failure Discuss how sodium affects chronic kidney disease Dietary Sodium, hypertension, and the scope of problem Salt is common in the American diet average daily intake > 3.0 grams Ingesting too much salt can contribute to worsening of many common health problems hypertension, congestive heart failure, and chronic kidney disease. Associated morbidity and mortality Modifiable factors, including adjustments in sodium intake. Article 1 Sodium’s Role in the Human Body Sodium draws water to itself and is therefor a way to maintain blood volumes and blood pressure at appropriate levels Sodium is an element essential for nerve and muscle function Muscle contractions and nerve signals utilize sodium to communicate with electrical currents Hyponatremia Too little sodium Muscle cramps, headaches, irritability, fatigue, nausea, confusion, hallucinations, coma, death Hypernatremia Too much sodium Lethargy, spasticity, seizures www.uptodate.com Sodium’s Adverse Affects Excess consumption of sodium is a major contributor to the disease processes related to elevated blood pressures Sodium chloride (table salt) Increased sodium intake leads to elevated blood pressures Increased sodium can cause renal injury and increase the rate of injury already caused by diabetes or glomerulonephritis It can cause an increase in filtration rate, increased albumin excretion, increased oxidative stress, and increased fibrosis All further damaging and scarring to the kidneys Increased amounts of sodium can decrease the effects of some blood pressure medications Which help lower blood pressures and stop protein excretion from the kidneys Article 1 Hypertension Definitions of elevated blood pressure Normal blood pressure: 120/80 mmHg (systolic/diastolic) Pre hypertension: 121-139/81-89 mmHg Hypertension: > 140/90 mmHg Hypertension and Related Diseases Blood pressure has a direct effect on many diseases Blood pressure can be modifiable Examples of diseases related to blood pressure coronary artery disease stroke congestive heart failure chronic kidney disease Coronary artery disease and stroke are among the top causes of morbidity Chronic hypertension fibrosis of heart, kidneys, and arteries Left ventricular hypertrophy Article 1 Hypertension Essential Hypertension No clear identifiable cause, such as kidney or adrenal disease Seen mostly in societies where dietary intake is greater than 100 meq/day (2.3 g sodium) 1 teaspoon of salt is 2.3 g of sodium Certain societies can be as low as 50 meq/day (1.2 g Sodium) Observations show there may be a threshold level of sodium intake as it relates to elevated blood pressure Chloride ion important Elevated blood pressure not seen in other ion combinations such as sodium citrate or ammonium chloride Age related hypertension is associated with increased stiffness of major blood vessels in the body Article 1 Essential Hypertension and Sodium Excretion In essential hypertension, hypertension which is not related to kidney disease or adrenal disease sodium excretion is impaired It is theorized that essential hypertension has a genetic component and that certain genes may be responsible for the bodies inability to process sodium properly Article 4 Sodium as it Relates to Hypertension Mechanism of sodium sensitivity aren’t well understood May be related to the way the body processes sodium and chloride A increased intake of sodium typically leads to increased blood volume which causes an increased pressure to be noted at the kidneys This pressure leads to the excretion of salt and water in the kidneys known as “pressure natriuresis” which is the body’s regulatory mechanism for decreasing blood pressure Sodium and water are urinated and normal blood pressure restored This blood pressure regulatory system is accomplished through hormone signals involving the liver, kidneys, adrenal glands, and posterior pituitary gland Renin-Angiotensin-Aldosterone System Article 2 http://en.wikipedia.org/wiki/Renin%E2%80%93angiotensin_system Salt Sensitivity Salt sensitivity Blood pressure that changes in relation to amount of sodium in the body Increases with age African Americans Obese patient Metabolic syndrome Chronic kidney disease May play a role in development of hypertension in these patient groups These groups don’t appear to utilize the renin-angiotensin-aldosterone system as much to regulate sodium levels and blood pressure Article 2 Salt Sensitivity Those without salt sensitivity can process a sodium load without an increase in blood pressure by suppressing the renin release and increasing atrial natriuretic peptide ANP is a natural dilator of arteries and stimulates sodium excretion which decreases blood pressure Those who are not salt sensitive also tend to have a baseline lower blood pressure Article 2 Effects of Increased Sodium Intake Hyperfiltration Leads to kidney damage – overworking of the kidneys Reduced effectiveness of calcium channel blockers and ACE Inhibitors in patients with proteinuria Increased calcium excretion Left ventricular hypertrophy Elevated heart rate Insulin resistance Stomach cancer incidence increased Asthma Article 1 Sodium Restriction and Hypertension Restricting dietary sodium Lower extracellular volume which decreases blood volume and blood pressure This decrease in blood pressure has been seen in both hypertensive and normotensive patients Appears to improve response to blood pressure medications except calcium channel blockers Sodium restriction may also decrease the degree of potassium depletion that occurs when taking diuretics Potassium is a key element in cellular function Increase in renin production Lead to blood pressure more dependent on Angiotensin II Leads to blood pressure more responsive to ACE Inhibitors (ex. Lisinopril) and Angiotensin II receptor blockers (ex. Losartan) Article 2 Benefits of Decreased Sodium Intake Sodium reduction is related to less stiffness in blood vessels Sodium reduction is related to arterial vasodilation Decrease cardiac output due to less blood volume Decrease work load on the heart Weight loss decreases the sympathetic nervous system Less activation of the RAAS Decreased blood pressure Weight loss is thought to lessen sodium retention Decreased blood pressure Article 4 Effects of Decreased Sodium Intake Lower urinary calcium excretion (decreased kidney stones) Potential reduced risk of osteoporosis Less calcium excreted from body Increased anti-protein effects on patients with chronic kidney disease who are taking ACE Inhibitors Help slow progression of CKD Improvement of left ventricular hypertrophy Chronic high blood pressure causes the muscle wall to thicken and stiffen and therefor has a decreased ability to pump as well as a normal heart LVH and chronic hypertension are cofactors in the development of certain types of congestive heart failure Article 2 Sodium and Comorbid Diseases Sodium intake also related to other conditions that can aggravate hypertension Insulin resistance Affects propensity for DMII and hypertriglyceridemia Cofactors in chronic kidney disease and atherosclerosis Hyperlipidemia Renal injury Can lead to increased renal vasoconstriction and decreases sodium excretion Can lead to worsening of hypertension Article 2 Article 4 Article 4 145 Control diet 140 135 Higher to lower sodium Control: −8 DASH: −7 −2.1 (−0.1 to −4.0) −8.0 (−4.9 to −11.1) −6.0 (−4.0 to −7.9) −7.5 (−4.2 to −10.8) DASH diet −1.6 (0.6 to −3.8) 130 125 0 −6.7 (−3.5 to −9.8) −5.1 (−3.0 to −7.3) Lower-sodium DASH vs. higher-sodium control: −15 High (3.5 g) Intermediate (2.3 g) Low (1.2 g) Dietary Sodium Figure 2. Sodium Reduction, the DASH Diet, and Changes in Systolic Blood Pressure. Article 4 The figure shows the additive beneficial effects of the DASH diet and reduced intake of sodium on systolic blood pressure in patients with mild hypertension who were older than 45 years of age. The participants were a subgroup of those in the study of the effects of the DASH diet and reductions in dietary sodium,53 who were randomly assigned to follow a DASH diet (33 participants) or a typical U.S. diet (37 participants) for 90 days. During that period, each group consumed three versions of the diet adjusted for daily sodium content. The participants in each group consumed each of the sodiumadjusted diets for 30 days in a crossover design; body weight was held constant. The two downward-sloping arrows on the left depict the effect of intermediate sodium intake as compared with higher sodium intake, and the two downward-sloping arrows on the right depict the effect of lower sodium intake as compared with intermediate sodium intake. The dotted lines show the effect of the DASH diet as compared with the typical U.S. diet at each level of dietary sodium. Numbers shown represent the mean changes with 95% confidence intervals. Adapted from Bray et al.54 DASH Diet vs. Control Diet 3.5, 2.3, and 1.5 grams sodium per day (high/intermediate/low) NEJM, 2011 “Systolic blood pressure was 12 mm Hg higher among participants between 55 and 76 years of age than among those between 21 and 41 years of age when they were given a typical U.S. diet that was high in sodium. This difference in systolic blood pressure is similar to that in the U.S. population when the same age groups are compared.55 In marked contrast, systolic blood pressure was the same among older and younger participants when they were given the DASH diet with low sodium content. This finding suggests that the typical rise in blood pressure that occurs with age during adult life may be prevented or reversed if the low- sodium DASH diet is followed.” “Women, blacks, and those with the metabolic syndrome have a mildly enhanced reduction in blood pressure in response to a low-sodium diet". 53,54,56,5 Article 4 Congestive Heart Failure Congestive Heart Failure Heart failure is one of the most common causes of hospitalization, readmission, and death Its prevalence and morbidity/mortality makes the importance of early intervention and patient care at home critical Approximately 5.8 million Americans have heart failure Leading cause of hospitalization in patients over 64 Over ¼ of those patients will be readmitted within 30 days Article 5 Congestive Heart Failure Heart failure is when the pumping mechanism of the heart does not work properly Increased blood pressures and failed pumping mechanism of the heart fluid leaks back into the tissues (lungs, legs) Shortness of breath and fatigue The physiology of heart failure is related to decreased cardiac output, increased blood pressures, and decreased blood flow to the kidneys This perpetuates a cycle of the kidneys attempting to hold onto sodium and water to keep blood pressures elevated despite the fact that the body’s blood pressure is elevated Article 6 Article 6 Figure. Effects of sodium intake in heart failure: low-sodium intake may have varied effect on heart failure. Intravascular volume contraction improves hemodynamics and reduces diuretic requirement, congestion, and myocardial wall stress, leading to compensated heart failure. Intravascular volume contraction, however, may also lead to a vicious cycle of increased sodium and water retention through neurohormonal activation predisposing to decompensated heart failure. AVP indicates arginine vasopressin; Na, sodium; K, potassium; MR, mitral regurgitation; PWCP, pulmonary wedge capillary pressure; red plus, diuretic action enhances contraction of intravascular volume; red minus, low diuretic doses reduce hormonal activation and contraction of intravascular volume. Article 6 Congestive Heart Failure At least 1/5 of the patients with acute episodes of heart failure are due to ingestion of too much sodium Decreased sodium and decreased blood pressure enhances the effects of blood pressure medications and helps prevent excess loss of potassium by antihypertensive medications The American Heart Association and the American College of Cardiology recommend less than 3 grams per day of sodium ingestion for those with heart failure recommends less than 2 grams per day in those with severe heart failure Article 5 Monitoring Sodium intake Monitor salt intake Daily weights Identify concerning symptoms Shortness of breath Increased swelling in legs Adjust medications Good patient self care has been shown to reduce readmission to the hospital for acute exacerbation of congestive heart failure by 40% Article 5 Chronic Kidney Disease Chronic Kidney Disease Diabetes and high blood pressure are the top 2 causes of chronic kidney disease The number of people who are on Medicare disability due to end stage kidney disease increased from approximately 10,000 in 1973 to approximately 615,000 as of December 2011 Article 7 Chronic Kidney Disease High sodium intake decreases the anti-protein effects of antihypertension medications such as ACE inhibitors or Angiotensin Receptor Blockers Decreased blood pressure = less damage to the kidneys Proteinuria associated with worsening kidney function High sodium intake also related to a higher incidence of end stage renal disease Maintaining lower blood pressures is the mainstay of CKD treatment Prevent further damage to the kidneys from elevated blood pressures Goal blood pressure of less than 130 mmHg systolic Article 7 Recommendations for Sodium Intake Because 90% of people will eventually develop high blood pressure the 2013 guidelines at U.S. Department of Health and Human Services suggests that all people consume less than 2300 mg/day A decreased intake of sodium by 75 meq/day for 4 or more weeks has shown a decrease in blood pressure by 5/3 mmHg in hypertensives and 2/1 mm Hg for those without hypertension More of a reduction in blood pressure seen with salt restriction in older adults versus younger adults It seems that sodium restriction can reduce the blood pressure rise seen with age Article 2 Recommendations Around the World World Health Organization Centers for Disease Control The United Nations The U.S. Department of Health and Human Services (HHS) and the U.S. Department of Agriculture (USDA) http://health.gov/dietaryguidelines/default.asp Dietary guideline for Americans (every 5 years) Advises sodium intake of 2300mg/day or less National Institute of Health DASH diet (Dietary approach to stop hypertension) Fruits, vegetables, whole grains, low fat dairy, low in saturated and trans fats, low sugar, low sodium Advises 2300mg/day of sodium, and 1500mg/day or less to further lower sodium in certain populations Recommendations for Sodium Intake American Heart Association 1.5 grams sodium/day or less JNC 7 in 2003 2.3 grams sodium/day 2007 European Society of Hypertension 2 grams/day Department of Agriculture and of Health and Human Services and National Institute of Health 2.3 grams/day or less of sodium If over 50 years old, African American, HTN, DMII, CKD then less 1.5 grams/day Table 1. Re com m e nde d We e k ly and Occas ional Food Purchas e s for One Pe rs on Follow ing a He althful Die t Containing 2100 k cal and 1500 m g of Sodium pe r Day.* Type of Food We e k ly purchas e s Se rvings pe r Wk Se rving Size Total Am ount Re com m e ndations Purchas e d pe r Wk Market periphery Vegetables† Leafy greens Salad greens Other greens Cruciferous Colorful‡ Do most weekly shopping in this section 4 4 3 15 1 cup 1/2 cup 1/2 cup 1/2 cup Other Fruits Fresh 3 1/2 cup 20 Dried Juice Herbs, alliums, and other seasonings Meat, poultry, and fish Fish and shellfish 8 4 Use freely 1 medium or 1/2 cup chopped 1/4 cup 1 glass (8 oz) 2 6–8 oz 1 lb Poultry Red meats Dairy products Milk Yogurt Cheese Processed-food aisles§ Nuts (whole or butter) Legumes Olives Spices Baked goods 2 1 6–8 oz 2–4 oz 1 lb 1/4 lb 10 3 4 1 glass (8 oz) 1 cup 1 slice 10 3 2 Use freely 20 Tomato products Chips and other snacks Chocolate or sweets Other food aisles (sweetened beverages, candy, cookies) Le s s frequent purchases‖ Breakfast cereals Pasta, rice, and grains Cooking oils Table fats 12 16 Salad dressings and mayonnaise Sugars Desserts Eggs 21 24 Salt 1 oz 1 cup 1/2 cup 1 slice 1–2 bags or heads 1–2 bunches 1–2 heads 8–12 individual items 1/2 lb 15–20 individual items 1 bag 1 qt 1/2 gallon 1 container 1/4 lb 1 bag or jar 1 can or bag 1 jar 1 bag 4 3 1 2/3 cup 1/2 cup 1 oz 2 jars or cans 3 bags 1 bar or similar amount 2 3 1/2 cup 1 cup (cooked) 1 tbs 1 tsp 1 1/2 cups 1/2 cup Lettuce, mixed spring greens, spinach bunch (about 1 lb) Kale, collard greens, mustard greens (about 1 lb) Broccoli, cabbage, cauliflower (about 1 lb) Tomatoes, carrots, squash, peppers, sweet potatoes, corn, eggplant, avocados (about 3 lb) Celery, green beans, peas, lima beans, sprouts Apples, pears, grapes, bananas, peaches, plums, oranges, tangerines, berries, cantaloupe, pineapple Raisins, apricots, prunes, cherries (about 1/2 lb) Orange, grapefruit, unsweetened carrot Thyme, ginger, garlic, onion, bay leaf, lemon juice Cod, sea bass, halibut; fresh or canned salmon, tuna, or sardines; mollusks, shrimp, crabmeat Turkey, chicken, low-sodium cold cuts Beef, pork, lamb, low-sodium cold cuts Choose low-fat or nonfat products Choose low-fat or nonfat products (about 32 oz) Soft or hard Choose only low-sodium products¶ Walnuts, almonds, peanuts (about 1/2 lb) Chickpeas, lentils, black beans (about 1 lb) Black, green, stuffed (about 1/4 lb) Black pepper, cayenne, cinnamon, paprika Bread, rolls, pancakes, waffles (about 1 1/2 lb); choose wholegrain products Sauce, juice, whole or diced (about 12 oz per jar or can) Tortilla chips, popcorn, pretzels (about 1 1/2 oz per bag) Granola bars, chocolate bars (about 1 oz) Skip these aisles Oats, bran, whole wheat flakes, other whole grains Pasta, brown rice, bulgur, quinoa, wheat berries 3/4 cup 1/3 cup Canola, corn, sunflower, olive, soybean Soft, oil-based spreads free of trans fat 1 3 1 tsp 1 tsp 1/2 cup 1 1/2 cup 1/2 cup 1/2 cup 3 Choose low-sodium items Table sugar, jelly, honey, maple syrup Ice cream, sorbet, frozen yogurt, other (4 oz) Large eggs 7 1/3 tsp 2 1/3 tsp Salt for cooking or added at the table References 1. Circulation. 2011;123:1138-1143, Appel et al. 2. https://uptodate.com/contents/salt-intake-salt-restriction-and-primaryessential-hypertension 3. https://uptodate.com/contents-antihypertension-therapy-andprogression-of-non-diabetic-chronic-kidney-disease-in-adults 4. N Engl J Med 2010:362:2102-12. Sacks M.D., Frank M. and Campos PhD., Hannia 5. https://uptodate.com/contents-overview-of-the-therapy-of-heart-failuredue-to-diastolic-dysfunction 6. http://circ.ahajournals.org/content/126/4/479.full#T1 7. https://uptodate.com/contents-epidemiology-of-chronic-kidney-disease