Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
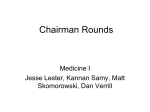
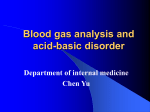
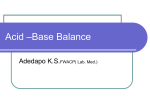
Dr. Montemayor OS 214: Excretory System Module Juan Lecture 3: Interpretation of Arterial Blood Gas Review of the Physiology of Acid-Base Balance Acid-Base Disorders Concept of the Anion Gap Interpreting the ABG and Clinical Applications Exercises F. Three-phased series mechanism that responds to the initial change from normal acid-base status 1. Buffering – most rapid chemical process (in onset); this refers to the ability of a solution containing a weak or poorly dissociated acid and its anion to resist a change in pH upon addition of a strong acid; this means that when an acid is introduced, it is immediately buffered, resisting a change in pH * acid still remains (compared with acids undergoing #2 mechanism: compensation) ex. protein – albumin REVIEW OF THE PHYSIOLOGY OF ACID-BASE BALANCE A. Definitions Acid = H+ donor Base = H+ acceptor Acid (H+ donor) H2CO2 H3PO4 H2PO4- Base (H+ acceptor) HCO3H2PO4HPO4= Major Buffers: HHb H2PO4 H2CO3 The definition of base/acid does not depend on the charge. Note that H2PO4- can be both an acid and a base. Definition is based on ability to donate/accept H+ B. Acid Strength The strength of an acid depends on its solubility. Strong acid – one which, when in solution, is completely or almost completely dissociated; very little exist as undissociated HA H+ + A Weak acid – one which when in a solution is only slightly dissociated; important in biological systems - type used in our body; dissociation is reversible; can exert a positive or negative effect of H+ ion to/from solution HA H+ + A- H+ + HbH+ + HPO= H+ + HCO3- [From 2011] The Respiratory Buffer Response A normal by-product of cellular metabolism is carbon dioxide (CO2). CO2 is carried in the blood to the lungs, where excess CO2 combines with water (H2O) to form carbonic acid (H2CO3). The blood pH will change according to the level of carbonic acid present. This triggers the lungs to either increase or decrease the rate and depth of ventilation until the appropriate amount of CO2 has been re-established. Activation of the lungs to compensate for an imbalance starts to occur within 1 to 3 minutes. Other examples of buffers include : a. pCO2/HCO3- (independently regulated by the lungs and kidneys) b. Hemoglobin buffer system: When in the deoxy form, hemoglobin can buffer more acid. Co2 is transported to the lungs as HCO3c. Cellular and plasma proteins, intracellular organic phosphates, bone (carbonates and phosphates) D. Sources of Hydrogen Ion Loss *pH maintained at a very, very narrow range 1. Loss of H+ in the vomitus: gastric secretions 2. Loss of H+ in the urine The only two pathways by which a person can lose H+ 2. Compensation - a process of slower onset than buffering but much more effective in returning pH toward normal. * because you remove a certain acid/base (compared with those in #1 mechanism: buffering) E. Threats to pH 1. Volatile acids: CO2 CO2: major end product in the oxidation of carbohydrates. Fats and amino acids can be regarded as an acid by virtue of its ability to react with water to form carbonic acid (H2CO3) which can dissociate to form H+ and HCO3-. 2. The Renal Buffer Response In an effort to maintain the pH of the blood within its normal range, the kidneys excrete or retain bicarbonate (HCO3 -). As the blood pH decreases, the kidneys will compensate by retaining HCO3- and as the pH rises, the kidneys excrete HCO3- through the urine. Although the kidneys provide an excellent means of regulating acid-base balance, the system may take from hours to days to correct the imbalance. When the respiratory and renal systems are working together, they are able to keep the blood pH balanced by maintaining 1 part acid to 20 parts base. C. Sources of Hydrogen Ion Gain = Bicarbonate loss 1. Generation of H+ from CO2 2. Production of acids from metabolism of protein and other organinc molecules 3. Gain of H+ because of loss of HCO3- in diarrhea or other nongastric fluids 4. Gain of H+ because of loss HCO3 in the urine Gaining an acid is equivalent to losing a base. Or losing an acid is equivalent to gaining a base. Yep. CO2 + H2O H2CO3 carbonic acid 1 a. Hypotension: decreased BP : increased lactic acid in hypoxic cells (glycolysis shifts to lactic acid production in hypoxic states versus shift to Kreb’s cycle in normal oxygen states) b. DKA: decreased insulin: increased production of ketoacids. OUTLINE I. II. III. IV. V. EXAM - H+ + HCO3- Fixed acids: Sulfuric and Phosphoric Acids; usual exogenous sources are meaty foods / proteins. Thus, a meat eater would produce acids more, while a vegetarian would produce alkali more. Organic Acids: Lactic acid (muscle fatigue/anaerobic metabolism); acetoacetic acid and beta-OH butyric acid (starvation, DM – absence of insulin) formed during the metabolism of carbohydrates and fats Usually seen in pathologic states In the physiological state, organic acids are present in small amounts because they are readily metabolized by the liver into bicarbonates. Accumulation of organic acids is evident in pathological states. (e.g. lactic acid is generated in tissue ischemia) - The respiratory system, by altering PCO2 constitutes compensation in metabolic disorders. The lungs handle the respiratory component by either blowing off or retaining CO2. The kidneys by altering plasma [HCO2-] provide compensation in respiratory disorders. The kidneys handle the metabolic component in terms of removing or retaining HCO3. Respiratory compensation is faster (3 – 4 hrs) than renal compensation (42 – 48 hrs delayed), but renal compensation is more complete. *acute if not compensated yet 2012: The kidneys and lungs are the yin-yang stuff of the body. The kidneys handle the metabolic component in terms of removing or retaining HCO3. The lungs, on the other hand, handle the respiratory component by either blowing off or retaining CO2. Both work to maintain body pH in the face of fluctuating CO2/HCO3 values. Page 1 of 8 MONDAY | March 1, 2010 JF, Justin, Alex, Suzie Dr. Montemayor OS 214: Excretory System Module Juan Lecture 3: Interpretation of Arterial Blood Gas Again, when an acid is introduced, the buffer system will try to bring pH back to normal (it will never normalize, though). If the pH remains neutral after adding acid, then acidic/alkali problems exist. 3. Correction - the definitive process that returns all the acidbase variables to normal. ex. kidney failure – recovery; kung problems – recovery G. The Law of Mass Action and the Henderson-Hasselbach Equation HA H+ + Av1 = k1 [HA] v2 = k2 [H+] [A-] 1 All gases partially dissolve/dissociate in water. The degree to which this occurs is proportional to the partial pressure of gases in solution. In humans, the partial pressure of CO2 is 40mmHg. [CO2] dis = α P CO2 = 0.03mmol/L/mmHg x 40 mmHg = 1.2 mmol/L where 0.03 mmol/L/mmHg is the solubility constant for CO2 in the plasma at normal temperature (therefore, febrile/hypothermic states may affect the solubility constant). BASIC RULE: in body fluid, at equilibrium: v1 = v2 since they’re equal, substituting for v1 and v2: k1 [HA] = k2 [H+] [A-] EXAM Equilibrium In plasma at 37o C, K’a = 800 nanomol/L and [ CO2 ] dis = 0.03 x P CO2 Thus: [ H+ ] = (800x0.03) P CO2 [HCO3- ] [ H+ ] = 24 P CO2 [HCO3- ] If k1/k2 = ka, then: ka [HA] = [H+] [A-]\ Solving for [H+]: * In most ABG machines, pCO2 is directly measured; [HCO3-] is only measured via an equation [H+] = ka [ HA ] [ A- ] This is the Henderson equation. ***To keep the concentration of H+ constant: if there is an increase in acid concentration [HA], the base concentration [A-] should increase, too. If you want to measure the pH: Taking the -logarithm of both sides: -log [H+] = - log ka - log [HA]/[A-] Since the normal H+ concentration is 40 nanomol/L and the P CO2 is 40 mmHg, the normal [HCO3- ] can be calculated: At pH of 7.4, 40 = 24 x 40 . [HCO3- ] [ HCO3-] = 24 mmol/L The normal free [H+] is very minimal, 40 nmoles/L only. This ion is very reactive and can easily displace other cations in enzymatic reactions. By comparison, Sodium (Na) is around 135-145 mmol/L! if: pH = - log [H+], pka = - log ka and + log [A-] / [HA] for - log [HA] / [A-] then: pH = pka + log [ A- ] [ HA ] Must Know! This is the Hasselbach equation. ***However, it is difficult to get acid-base relationship using this equation. H. HCO3/CO2 Buffer system CO2(g) CO2 (aq) + H20 H2CO3 H+ + HCO3 removed Since H2CO3 readily dissociates to H+ and HCO3, we can say that CO2 + H2O goes straight to it (minimal amounts of H2CO3). The equation can be simplified to: [CO2 ] dis + H2O H+ + HCO3- Normal values: [HCO3] = 24 mmol/L pCO2 = 40 mmHg [H+] = 40 nanomole/L Plasma pH = 7.4 [ H+ ] = 24 pCO2 [HCO3- ] I. Isohydric Principles From the law of mass action, the acid/base ratio of any weak acid is determined by its Ka and the H+ concentration of the solution. Since the H+ concentration affects each buffer, the following relationship is present: [ H+ ] = Ka1 0.03 PCO2 = Ka2 [ H2PO4- ] [HCO3- ] [ HPO4= ] = Ka3 [ HA] [A-] If the H+ concentration is altered, the acid/base ratios of all the buffers in the solution are affected. *can use any body buffer system The law of mass action for this reaction is: Ka = [ H+ ] [HCO3- ] [CO2 ] dis [ H2O ] Since the concentration of water is constant, ( Ka x [ H2O ]) can be replaced by: Hasselbach equation: pH = pka + log [A-] or pH = pka + log base [HA] acid K’a = [ H+ ] [HCO3- ] [CO2 ] dis Note: K’a is equal to (Ka x [H2O]), so if you substitute it with the previous equation, (the one with Ka), and you solve for K’a, you get this equation. Solving for [H+], [ H+ ] = K’a [ CO2 ] [ HCO3- ] Note: It will make life easier if you can memorize this equation :-? Since CO2 metab is in the lungs and HCO3 is in the kidneys: pH = pKa + log kidneys - base lungs - acid Note that the numerator in the above equation is the acid handled by the lungs, and the denominator is the base handled by the kidneys Page 2 of 8 MONDAY | March 1, 2010 JF, Justin, Alex, Suzie Dr. Montemayor OS 214: Excretory System Module Juan Lecture 3: Interpretation of Arterial Blood Gas J. Relationship of pH to H+ concentration Acidification: pH < 7.4 Alkalinization: pH > 7.4 (Acidemia) (Alkalemia) EXAM ACID-BASE DISORDERS K+ in Metabolic Acidosis (nM) H+ H+ doubles for each; 0.3 unit fall in pH H+ halves for each 0.3 unit rise in pH Organic anions H+ K+ K+ K+ SO4PO4= A pH increase of just 0.3 decreases H+ to half the normal value, while a pH decrease of just 0.3 doubles it! Normal pH is 7.4 Organic acidosis ex. H+ pH 7.1 free H+ is 80nM Inorganic Acidosis - eg. intentional ingestion of acids i.e. sulfuric acid, renal failure accumulation of sulfates & phosphates - when H+ increases, it moves into the cell while inorganic anions (ie PO4, SO4) stay out, so K+ goes out to maintain balance, thus there would be an increase in serum concentration of K+. * inorganic acidosis extreme K+ depletion compared to organic acidosis MUST KNOW! MUST UNDERSTAND! What is the H+ if the plasma pH is 7.16? pH H+ 7.4 40 7.16 x .24 y .3 .3 _____ -40 = _____ .24 y -40 TABLE 1. CHARACTERISTICS OF PRIMARY ACID – BASE DISTURBANCES 1º Disorder pH [H+] Compensation Disturbance Metabolic ↓ ↑ ↓ PaCO2 ↓ [HCO3-] -oracidosis ↑ PaCO2 Metabolic ↑ ↓ ↑ [HCO3-] -or↑ PaCO2 alkalosis ↓ PaCO2 Respiratory ↓ ↑ ↑ PaCO2 -or↑ [HCO3-] Acidosis ↓ [HCO3-] Respiratory ↑ ↓ ↓ PaCO2 -or↓ [HCO3-] alkalosis ↑ [HCO3-] * Metabolic HCO3Respiratory pCO2 Problems in handling of HCO3- is a metabolic problem Problems in handling CO2 means that there is a respiratory problem Compensatory response goes in the same direction as the 1o disturbance parameter in bold How to look at it: a decrease in pH means there is retention of acid or a loss of a base. Acidosis = decrease in pH due to accumulation of H+ 80 40 – x = y 40 + 32 = x X = 72 y = -32 Step 1: Step 2: Step 3: Step 4: Step 5: Step 6: Inorganic acidosis Organic Acidosis - eg. lactic acidosis, ketoacidosis - as H+ increases, it moves into the cell together with organic anions, thus there is no change in serum concentration of K+. Exercise: What is the H+ if the plasma is 7.16? pH H+ 7.4 40 7.16 x 7.10 80 7.10 1 normal pH minus lowest 7.4 – 7.10 = 0.3 normal H+ minus lowest 40 – 80 = -40 normal pH minus x 7.4 – 7.16 = 0.24 normal H+ minus x = y 40 – x = y divide the answer in step 3 by 0.3 units 0.3/0.24 = -40/y y = -32 substitute y in equation in step 4 40-x = y 40+32 = x x =72 ↓ HCO3- or ↑ PaCO2 Note: This only works for computing values near physiologic pH, 1º Disturbance: Compensatory: since at that range, the curve of values is relatively linear. Application: pH = 7.6 H+ = 26nmol/L pCO2 = 26mmHg HCO3- = ? metabolic ↓ PaCO2 respiratory ↑ HCO3- To recognize the primary problem, look at the: 1. pH 2. PaCO2 then [HCO3-] TABLE 2. COMPENSATORY RESPONSES IN SIMPLE ACID-BASE DISORDERS H+ = 24 x pCO2/HCO3(recall encircled equation in the previous page) * Ex. salicylic acid poisoning H+ Tx: alkalinize urine pH=7.5 Disorder How much HCO3- should be given? 26 = 24 x 26/HCO3HCO3- = 24 24 should be considered normal, BUT pH is abnormal (7.6), so another parameter must be abnormal, too. (remember the Must Know! box in page 2?) Metabolic acidosis Metabolic alkalosis Respiratory Acidosis Respiratory alkalosis 1 Abnormality HCO- 2 Response Loss of 3 or gain of H+ Gain of HCO-3 or loss of H+ Hypo-ventilation ↑ ventilation HCO3- generation Hyper-ventilation HCO3- consumption ↓ ventilation Page 3 of 8 MONDAY | March 1, 2010 JF, Justin, Alex, Suzie Dr. Montemayor OS 214: Excretory System Module Juan Lecture 3: Interpretation of Arterial Blood Gas TABLE 3. RENAL AND RESPIRATORY COMPENSATION TO 1 ACID – BASE DISTURBANCES Compensatory Disorder 1 Abnormality Response Metabolic ↓[HCO3-] -or1.2mmHg DECrease in PaCO2 for every acidosis ↑PaCO2 1mEq/L fall in HCO-3 Metabolic ↑[HCO3-] -or0.7mmHg INCrease in PaCO2 for every alkalosis ↓PaCO2 1mEq/L rise in HCO3Respiratory Acidosis (acute) ↑PaCO2 -or1mEq/L INCrease in [HCO-3] for every Ex. pneumonia, ↓[HCO3-] 10mmHg rise in PaCO2 PaCO2 = 15 Answer: Given the ff. ABG results, describe the acid-base status and adequacy of compensation: Ex 1. [HCO3-] = 24 PaCO2 = 40 pH = 7.40 PaCO2 = 22 Normal pH; Low [HCO3-]; Low PaCO2. To determine the dominant factor (whether it is metabolic acidosis or respiratory alkalosis) in the maintenance of such pH, compute how deviated each value is from the normal. Since there is no greater parameter (the deviations are equal), the acid base status is a… COMBINED METABOLIC ACIDOSIS & RESPIRATORY ALKALOSIS. Arterial Measurements in Hypothetical Acid-Base Disorder [HCO3-] PCO2 meq/L mmHg pH = 7.24 Answer: a. Low pH; Low [HCO3-]; Low PaCO2 PURELY METABOLIC ACIDOSIS b. Ideal compensatory response: remember that in metabolic acidosis, there is a 1.2mmHg decrease in PaCO2 for every 1mEq/L fall in HCO3-. Thus: Fall in HCO3- = normal value (NV) – given value = 24 – 9 = 15 (N) [HCO3-] = 24 (normal) PaCO2 = 40 (normal) = 9 (patient) Deviation = 15 (patient) = (24-9)/24 Deviation = (40-15)/40 = 0.625 = 0.625 determine which parameter has a greater change in value of deviaion Answer: NORMAL Therefore, REMEMBER THESE VALUES! Ex 2. [HCO3-] = 9 pH = 7.40 1 Clinical situation that can present with this scenario: renal failure with hyperventilation (as an early compensatory response), proceeding to hypoventilation, after fatigue sets in. Ex 4. [HCO3-] = 9 acute asthma Respiratory Alkalosis ↓PaCO2 -or2mEq/L DECrease in [HCO-3] for every (acute) ↑[HCO3-] 10mmHg fall in PaCO2 In metabolic processes, the key value to remember is 1 mEq/L change. In respiratory processes, the key value is 10mmHg change. * Chronic respiratory conditions – ex. COPD, restrictive lung dses EXAM pH Acid base status 24 40 7.40 Normal 9 22 7.23 Pure metabolic acidosis 9 40 6.98 Primary metabolic and secondary respiratory acidosis 9 15 7.40 Combined metabolic acidosis and respiratory alkalosis Compensatory response (CR) = 15 x 1.2 (refer to table 3) = 18mmHg CONCEPT OF THE ANION GAP Ideal compensation = NV – CR = 40 – 18 = 22mmHg 2 20–24 Since actual PaCO2 (22 mmHg) is within the ideal PaCO2 (20–24 mmHg). Note: 2 in ideal compensation either for HCO3 or pCO2 ADEQUATE Compensation *PURE METABOLIC ACIDOSIS – pure siya if maximum pCO2 value is within 20-24 mmHg. If > 24mmHg, there is now a 2o respiratory acidosis. Total cations and anions in the ECF should be equal. Anion gap refers to the anions not routinely measured on serum electrolytes. The dominant anions are Sodium (140 mmol/L) and Chloride (105 mmol/L) Usually negatively charged proteins, SO4-, PO4 Generally, Na+ is the only cation considered in computing the anionic gap (since others have relatively small concentrations in serum). Any minor increase in K, Ca and Mg can be fatal! K+ Ca++ Mg++ *ex. PaCO2 = 25mmHg 1o Metabolic Acidosis with 2o Respiratory Acidosis Pr- ex. albumin; SO4=; PO4= Gets? Kamusta? If malabo, review muna previous pages… Ex 3. [HCO3-] = 9 PaCO2 = 40 Answer: AG HCO3- (N) pH = 6.98 Na+ Low pH; Low [HCO3-]; Normal PaCO2. 1 METABOLIC ACIDOSIS, 2 RESPIRATORY ACIDOSIS Since there is a decrease in [HCO3-], there should have been a corresponding PaCO2 decrease. But since PaCO2 is normal, it means no compensation occurred! If it rises above 40, then it’s time to intubate the patient. Cl(major anion) *K (4), Ca (2.5), Mg (0.8 -1)– very narrow range *Pr, SO4, PO4 – not routinely measured in lab Page 4 of 8 MONDAY | March 1, 2010 JF, Justin, Alex, Suzie Dr. Montemayor OS 214: Excretory System Module Juan Lecture 3: Interpretation of Arterial Blood Gas Anion gap is therefore defined as the DIFFERENCE between the EXAM 1 INTERPRETING THE ABG AND CLINICAL APPLICATIONS concentrations of measured cations and measured anions (since laboratory tests can’t measure it directly) 1. AG = [Na+] – ( [Cl-] + [HCO3-] ) Normal Value = 12 2 2. 3. 4. 5. ANION GAP Illustrations 6. Get a good History and PE. (it could tell you (1) the need for blood gas assessment and if there’s an acid-base disturbance and (2) what to expect in the interpretation ex. Renal failure high anion gap) Get your ABG. Determine the serum electrolytes at the same time. Know the primary disorder. Compute for the range of compensation. Don’t forget to 2! For METABOLIC ACIDOSIS: GET THE ANION GAP 1. FOR HIGH ANION GAP METABOLIC ACIDOSIS: Get ∆AG and compare it to ∆HCO3- to determine if there are other HIDDEN METABOLIC PROBLEMS. AG = AG – 12 (normal value) ∆HCO3- = 24 (normal value) - [HCO3] Table 4. Determining Hidden Problems in High Anion Gap Metabolic Acidosis ∆AG = ∆HCO3Pure High 10 lactate (lactic acid) AG H+ + lactate): H+ (buffered) + HCO3 metabolic CO2 + lactate goes to AG increasing acidosis A. Normal ion distribution B. High anion gap metabolic acidosis (accumulation of anions) Lactic acidosis: lactate Ketoacidosis: B-hydroxybutyric acid Renal failure: sulfate, phosphate, urate Ingestions - salicylates: ketones, lactatem salicylate - methanol/ formaldehyde - ethylene glycol: glycolate/ oxalate AG so high AG ∆AG > ∆HCO3- *ex. Adding lactic acid (H+ + lactate): H+ (buffered) + HCO3 CO2 + lactate goes to AG increasing AG - - diarrhea Renal HCO3- loss - types 1 Renal Tubular Acidosis (RTA) - Type 2 RTA - hyperkalemia Ingestion: ammonium chloride (NH4Cl) High AG metabolic acidosis w/ normal metabolic acidosis Renal failure + diarrhea (Kaw naman try mo explain?) Table 5. Determining Hidden Problems in Normal Anion Gap Metabolic Acidosis ∆Cl- = ∆HCO3- Metabolic Acidosis and the Anion Gap Na+ X- Pure Normal metabolic acidosis AG Na+ HCO3- H2CO2 H2O + CO2 Normal Normal AG Acidosis 140 105 24 11 High AG Acidosis 140 105 14 21 1 ∆Cl- < ∆HCO3- +10 11 0 Ingestion of poisons + NGT HCO3= 20: dapat 14 lang (from 24-10) so may na-add na 6 HCO3 so may met alka -10 0 1 Normal AG metabolic acidosis with metabolic alkalosis 10 HCl H+ (met acid) and Cl by 10, do not add in AG so ((N) AG) 140 115 14 11 -10 Diarrhea + ingestion of poisons 10 HCl H+ and HCO3 by 10 (met acid), Cl, do not add in AG so ((N) AG) ∆Cl- > ∆HCO3- Na+ ClHCO3AG Δ HCO3Δ AG LactΔ Lact Renal failure (accumulation of anions) adding to acidity and anions go to AG so increasing AG more high AG met acid 2. FOR NORMAL ANION GAP METABOLIC ACIDOSIS: Get ∆Cl- and compare it to ∆HCO3- to determine if there are other hidden metabolic problems (compare them since they are the only parameters that change, when AG is normal). *ex. add’n of HCl (H+ + Cl-): H+ (buffered) + HCO3 H2CO3 CO2 + H2O + Cl- (Cl does not go to AG so Normal pa din AG) H+ X- Renal failure +vomiting Vomiting H- met alka ∆AG < ∆HCO3- C. Normal anion gap metabolic acidosis Gastrointestinal loss of HCO3 High AG metabolic acidosis w/ metabolic alkalosis +10 Normal AG metabolic acidosis with high AG metabolic acidosis 2013 B: Another process which consumes bicarbonate>> metabolism Ingestion of poisons + renal failure 10 HCl H+ (met acid) and Cl by 10, do not add in AG so ((N) AG) HCO3 = 4: dapat 14 (from 24-10) so may naconsume na 10 HCO3 or may naaadd na acid Page 5 of 8 MONDAY | March 1, 2010 JF, Justin, Alex, Suzie Dr. Montemayor OS 214: Excretory System Module Juan Lecture 3: Interpretation of Arterial Blood Gas i.e lactic acid, ketoacid so may high AG met acid EXAM 1 1. What are the diagnostic clues for the presence of a possible blood gas abnormality? - The patient is from a place of high altitude (The Andes) compensatory in HCO3 - we need to get pH, PCO2 values POP Quiz! HPE Vomiting NGT Comatose not intubated Comatose intubated Renal failure + diarrhea Possible Interpretation Metabolic alkalosis Metabolic alkalosis Respiratory acidosis Respiratory alkalosis High AG metabolic acidosis with Normal metabolic acidosis High AG metabolic acidosis with hidden metabolic alkalosis Renal failure + vomiting *If px gains H+, it may also mean that px gains HCO3. Not discussed but included in the ppt: BUFFERS 1. pCO2/HCO3- (independently regulated by the lungs and kidneys) 2. Hemoglobin buffer system: When in the deoxy form, hemoglobin can buffer more acid. CO2 is transported to the lungs as HCO33. Cellular and plasma proteins, intracellular organic phosphates, bone (carbonates and phosphates) The Hemoglobin Buffer System: 9 6 ClHCO3KCl Cl6 K+ HCO3- HHb Hb- HHb 7 O2 HHbO2 KHCO3 K+ 5 HCO3- 4 H+ 8 Justin: Hi 2013 block A, renal na!!! we can do this! Hi to paul, motch, rommel! Suzie: For sale: GLOBE prepaid cards: G100 for P100, G300 for P290 & G500 for P 490. Moniegold Sweet and Spicy Tamarind candies for only P20. CO2 CO2 CELL KHCO3 10 H2CO3 CO2 CA 1 11 H2 O Lab works: pH = 7.11 pCO2 = 25.4 HCO3- = 7.8 Na+ = 141 mmol/L K+ = 2.4 mmol/L Cl- = 111 mmol/L Crea = 250mmol/L 2. What is your primary disorder? - low pH and decreased HCO3 Metabolic acidosis 12 2 CO2 PLASMA Problem 2: A 36-year old woman has been having watery diarrhea for the past 3 days after eating pork barbeque. When she was brought to emergency room, she was noted to be weak-looking with sunken eyeballs and poor skin turgor. Vital signs: BP = 90/60mmHg HR = 120/min RR = 26/min CA H2 O 3 HCO3- KHCO3 KHbO2 H2CO3 JF: Hi everyone! Congrats sa mga nanalo sa Culture Week!!! Ang galling ng 2013!!! HCO3Cl- K+ - HCO3 value can be a 1o or a 2o problem 1. What are your diagnostic clues? - watery diarrhea (she is losing bicarbonates) (N) AG metabolic acidosis) - weak-looking, sunken eyeballs, poor skin turgor dehydration perfusion renal failure high AG met acid - tachycardic worsening acidosis - weak-looking, hypotensive maybe lactic acidosis renal failure high AG metabolic acidosis Cl- KCl 2. What is your interpretation of the serum HCO3-? - Strictly speaking, the serum HCO3- is below normal (N=24nmol/L), but since we have to take into account the place of origin of the patient (The Andes), the serum HCO3- is actually just right for her to function well. CO2 3. What is your compensatory response? ALVEOLAR CAPILLARY Venous blood gas Fall in bicarbonate: Expected fall in PCO2: Expected PCO2 level: 24 - 7.8 = 16.2 16.2 x 1.2 = 19.44 40 - 19.44 = 20.56 2 = 18.56-22.56 Given pCO2: 25.4 ( > the upper limit of range or > 22.56) Not compensated 2o (mild) Respiratory acidosis Arterial blood gas So why worry about acids and bases? pH = 7.8 incompatible with life pH = 7.7 seizures, tetany pH = 7.6 muscle cramps, fatigued, irregular heart beat pH = 7.5 breathing is slow Worsening Alkalosis 4. What is the anion gap? AG = [Na+] – ( [Cl-] + [HCO3-] =141 – (111+ 7.8) = 22.2 22.2 > 12 2 (10-14) High anion gap metabolic acidosis pH = 7.4 normal arterial pH pH = 7.3 breathing is rapid pH = 7.2 fatigued, nausea and abdominal pain, pulse and breathing rapid pH = 7.1 blood pressure falling due to decreased force of heart beat and vasodilation, irregular pulse pH = 7.0 decreased consciousness pH = 6.8 incompatible with life Worsening Acidosis 5. Is there a hidden problem? Since it is a HIGH AG metabolic Acidosis, Compare Δ AG __?____ Δ HCO322 - 12 _______ 24 - 7.8 10 ___<____ 16.2 (8-12) (16.2 > 8-12) – may naconsume na at least 4.2 addtl HCO3 or may naadd na acid Yes, a Normal anion gap metabolic acidosis EXERCISES Before starting with the exercises, Let us review *sabi ni ma’am, easier daw na tingnan na lang yung difference between AG & HCO3 ex. in this case, 16.2-10 = 6.2. If ≥ 2, it is significant. There is a hidden problem. If Δ AG < Δ HCO3, there is metabolic acidosis. If Δ AG > Δ HCO3,there is metabolic alkalosis. PaCO2 = 40 mmHg [H+] = 40 nmol/L at pH = 7.4 2 for our purposes [HCO-3] = 24 nmol/L 6. What is your final interpretation? *If you’re not interested in getting pO2, you can use venous blood gas Also, just follow these steps in solving value. for the problems ahead. Problem 1 Step1: pH (Is it a problem of acidosis or alkalosis?) A 21 year old Andean woman had no medical problems. She was Step 2: PaCO2 (Is it respiratory?) accepted as a first year medical student in the USA. Before leaving, she Step 3: [HCO3-] (Is it metabolic?) underwent a complete history and physical examination, including Step 4: Check for compensatory response (Tables 2&3, p. 4 ) blood tests. Everything was normal except for a serum HCO3- of 15 Step 5: Compute for anion gap (In metabolic acidosis cases) mmol/L. AG = [Na+] – ( [Cl-] + [HCO3-] ) Normal Value = 12 2 HIGH ANION GAP METABOLIC ACIDOSIS WITH 2o RESPIRATORY ACIDOSIS AND A HIDDEN NORMAL ANION GAP METABOLIC ACIDOSIS Problem 3: A 27 year-old male with insulin-dependent diabetes mellitus has not been taking his insulin and is admitted to the hospital in a semicomatose condition. The following laboratory data are obtained: Page 6 of 8 MONDAY March 2010 Step| 6: Check if1,there is a hidden problem (Tables 4&5, p.5-6) *Usually (but not always: Hidden Problems are seen in High AG metabolic acidosis Step 7: State the final interpretation/diagnosis completely. JF, Justin, Alex, Suzie Dr. Montemayor OS 214: Excretory System Module Juan Lecture 3: Interpretation of Arterial Blood Gas [ Na+] = 140 meq/L pH = 7.10 [ K+ ] = 7.0 meq/L pCO2 = 20 mmHg [ Cl-] = 105 meq/L [ HCO3-] = 6 meq/L Glucose = 800 mg/L 1. What are your diagnostic clues? - not been taking insulin for his DM diabetic ketoacidosis high AG metabolic acidosis due to acetoacetic acid and/or beta-butyric acid - semicomatose condition fluid intake is most probably decreased respiratory acidosis 1 Since it is a HIGH AG metabolic Acidosis, Compare Δ AG __?____ Δ HCO318.1 - 12 ___?____ 24 – 20.9 6.1 ____>____ 3.1 (4.1 – 8.1) 3.1< (4.1–8.1)** **konti lang nagamit na HCO3. supposedly around 17.9 ang HCO3 but 20.9. Parang may nag-aadd ng HCO3…so look for other causes of hypokalemia Metabolic alkalosis 2. What is your primary disorder? Low pH, low HCO3 Metabolic Acidosis 6. What is your final diagnosis? HIGH ANION GAP METABOLIC ACIDOSIS WITH METABOLIC ALKALOSIS 3. What is the compensatory response? Fall in bicarbonate: 24 – 6 = 18; Expected decrease in PCO2: 18 X 1.2 = 21.6; Expected PCO2 level: 40 – 21.6 = 18.4 2 = 16.4-20.4 Given pCO2: 20 (within the expected level) Compensated Problem 5: A 45 y/o female with peptic ulcer disease complaining of persistent vomiting. PE: 100/60 mmHg, poor skin turgor, flat neck veins. [Na+] = 140 mEq/L pH = 7.53 [Cl-] = 86 mEq/L PaCO2 = 53 mmHg [K+] = 2.2 mEq/L [HCO3-] = 42 mEq/L 1. 4. What is the anion gap? AG = [Na+] – ( [Cl-] + [HCO3-] ) = 140 – (105 + 6) = 29 > 12 2 (10-14) High Anion gap metabolic acidosis Alex: Shameless plug You are all invited to WHITE LIE: Too good to be true on March 5, 2010 (Friday), 8:00pm, Hexagon Lounge, 4th floor, RCBC Plaza, Makati City. It’s going to be a night of white hot fashion, freeflowing booze, pounding hip hop beats all night, plus surprising games and prizes. For tickets and details, approach me. Dindin Grey! Happy birthday! Yay to chocolate fondue surprises. Sana di kayo masyado nagaway ni Karl. Haha! Sorry bangag ako sa “speech” ko. Si Pao kasi! Basta, you know that I love you always. I think that transcends all the speeches I can give. EXAM 2. What is your primary disorder? - high pH, high HCO3 Metabolic alkalosis 5. Is there a hidden problem? Since it is a HIGH AG metabolic Acidosis, Compare Δ AG __?____ Δ HCO329 - 12 _______ 24 - 6 17 ___<___ 18 (15-19) (18 is within 15-19) No hidden problem 3. What is your compensatory response? Increase in bicarbonate: 42 – 24 = 18 Expected rise in pCO2: 18 x .7 = 12.6 Expected pCO2 level: 40 + 12.6 = 52.6 2 = 50.6 – 54.6 Given pCO2: 53 mmHg (within the expected range) Compensated 6. What is your final diagnosis? HIGH ANION GAP METABOLIC ACIDOSIS, COMPENSATED Problem 4: A 17 year old male has a history of on and off weakness since 2 years ago. A few hrs before admission, he can’t move his lower extremities. [ Na+] = 154 meq/L pH [ K+ ] = 2.3 meq/L pCO2 [ Cl-] = 115 meq/L = 7.36 = 37.5 mmHg [ HCO3-] = 20.9 meq/L Base excess = - 3.7 What are your diagnostic clues? persistent vomiting metabolic alkalosis poor skin turgor poorly perfused tissues poorly perfused kidneys High AG metabolic acidosis *Base excess = excess of a base (hehehe) *If base excess is negative, there is an absence of an excess of the base. Like in this case. 1. What are your diagnostic clues? - on and off weakness HPP or Hypokalemic Periodic Paralysis - Severe hypokalemia ms injury toxic substance acute renal faillure -DDx: (1) Rebal tubular acidosis waste HCO3 (N) AG metabolic acidosis - (2) rhabdomyolysis acute renal filure High AG metabolic acidosis 4. What is your final diagnosis? COMPENSATED METABOLIC ALKALOSIS Not discussed: Causes of Impaired HCO3- excretion that allow metabolic alkalosis to persist Decreased GFR - Effective circulating volume depletion - Renal failure ( usually associated with metabolic acidosis) Increased Tubular Reabsorption - Effective circulating volume depletion - Chloride depletion - Hypokalemia - Hyperaldosteronism Pathophysiology of Metabolic Alkalosis 1. Why do patients become alkalotic? 2. Why do they remain alkalotic, since renal excretion of the excess HCO3- should rapidly restore normal acid-base balance Check serum and urine pH 2. What is your primary disorder? Low pH, low HCO3 Normal Anion Gap Metabolic Acidosis 3. What is your compensatory response? Decrease in bicarbonate: 24 – 20.9 = 3.1 Expected fall in PCO2 : 3.1 X 1.2 = 3.72 Expected pCO2 level: 40 – 3.72 = 36.27 2 = 34.27 – 38.27 Given pCO2: 37.5 mmHg (within expected range) Compensated 1. Serum and urine pH both increased: loss of acid through the GIT, gain of alkali, exogenous 2. Urine pH low: loss of acid through the kidneys (mineralocorticoid excess) 4. What is the anion gap? AG = [Na+] – ( [Cl-] + [HCO3-] ) = 154 - (115 + 20.9) = 18.1 > 12 2 (10-14) High anion gap metabolic acidosis 5. Is there a hidden problem? Page 7 of 8 MONDAY | March 1, 2010 JF, Justin, Alex, Suzie OS 214: Excretory System Module Juan Lecture 3: Interpretation of Arterial Blood Gas PROXIMAL PROXIMAL TUBULE TUBULE REABSORPTION REABSORPTION Lumen Proximal Tubule Cell ISF Na+ HCO3Na+ Na+ Na+ 5 H+ H+ 2 H+ H+ H2CO3 Na+ 1 ATP K+ H2CO3 CO2 4 H2O CA CO2 1. Active transport of Na+ creates an intracellular (-) allowing diffusion of Na+ 2. H+ is secreted into the lumen by the Na+ - H+ exchanger 3HCO3- HCO3- ATP 3 H2 O Dr. Montemayor 3. H+ combines wth filtered HCO3- to form H2CO3 and then CO2 and H2O 4. CO2 diffuses into the cell to combine with H2O to form H2CO3 then H+ + HCO35. HCO3- returns to the circulation by a Na+ - 3 HCO3- cotransporter Problem 6: A 54 year old lawyer complained of leg pains and eventually underwent femoral popliteal bypass surgery. Preop renal function and acid-base status were normal. 24 hours later, he was noted to be oliguric, cold and clammy and drowsy. PE revealed a BP of 90/60 mm Hg. HR = 126/min and absent pulses in his R foot. EXAM [ Na+] = 144 meq/L pH = 7.36 [ K+ ] = 4.2 meq/L pCO2 = 54.0 mmHg [ Cl-] = 105 meq/L [ HCO3-] = 30.6 meq/L 1. What are your clinical clues? 2. What is the primary disorder? 3. Compensatory response? 4. Anion Gap? 5. Hidden problem? 6. Interpretation? Problem 9: A 25 year old patient with epilepsy suffered a grand mal seizure. Immediately after the seizure, the ff labs were obtained: [ Na+] = 140 meq/L pH = 7.14 [ K+ ] = 4.2 meq/L pCO2 = 45.0 mmHg [ Cl-] = 98 meq/L [ HCO3-] = 14 meq/L 1. What are your clinical clues? 2. What is the primary disorder? 3. Compensatory response? 4. Anion Gap? 5. Hidden problem? 6. Interpretation? [ Na+] = 140 meq/L pH = 7.0 [ K+ ] = 6.4 meq/L pCO2 = 32 mmHg [ Cl-] = 103 meq/L [ HCO3-] = 8.0 meq/L 1. What are your diagnostic clues? - oliguric, cold and clammy and drowsy circulatory collapse, poorly perfused kidneys renal failure high AG metabolic acidosis - cold, clammy poor tissue perfusion lactic acidosis High AG metabolic acidosis - (-) pulses in his ® foot ischemia lactic acidosis high AG metabolic acidosis 2. What is your primary disorder? - low pH, low HCO3 Metabolic Acidosis 3. What is your compensatory response? Decrease in bicarbonate: 24 – 8.0 = 16 Expected fall in PCO2 : 16 X 1.2 = 19.2 Expected pCO2 level: 40 – 19.2 = 20.8 2 = 18.8 – 22.8 Given pCO2: 32 mmHg > expected range Not Compensated 2O Respiratory Acidosis 4. What is the anion gap? AG = [Na+] – ( [Cl-] + [HCO3-] ) = 140 - (103 – 8.0) = 29 > 12 2 (10-14) High anion gap metabolic acidosis 5. Is there a hidden problem? Since it is a HIGH AG metabolic Acidosis, Compare Δ AG __?____ Δ HCO329 - 12 ___?___ 24 – 8.0 17 ___>___ 16 (15-19) 16 is within (15-19) No Hidden Problem 6. What is your final diagnosis? HIGH ANION GAP METABOLIC ACIDOSIS WITH RESPIRATORY ACIDOSIS Practice Problems: Problem 7: This is a 50 year old male who underwent nephrolithotomy for R staghorm calculus. There was no ff-up after discharge. A few days prior to admission, he complained of weakness, nausea and vomiting. [ Na+] = 143 meq/L pH = 7.25 K+ ] = 6.2 meq/L pCO2 = 24.5 mmHg [ Cl-] = 102 meq/L [ HCO3-] = 10.8 meq/L 1. What are your clinical clues? 2. What is the primary disorder? 3. Compensatory response? 4. Anion Gap? 5. Hidden problem? 6. Interpretation? Problem 8: A 74 year old male was admitted for pneumonia. He presented with the ff. labs. Page 8 of 8 MONDAY | March 1, 2010 JF, Justin, Alex, Suzie 1