Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hospital-acquired infection wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Sociality and disease transmission wikipedia , lookup
Periodontal disease wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Chagas disease wikipedia , lookup
Marburg virus disease wikipedia , lookup
Schistosomiasis wikipedia , lookup
Kawasaki disease wikipedia , lookup
Ankylosing spondylitis wikipedia , lookup
Behçet's disease wikipedia , lookup
Neuromyelitis optica wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Infection control wikipedia , lookup
Transmission (medicine) wikipedia , lookup
African trypanosomiasis wikipedia , lookup
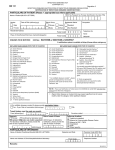
Appendix 5: NOTIFICATION OF INFECTIOUS DISEASE or FOOD POISONING No. To the CONSULTANT FOR COMMUNICABLE DISEASE CONTROL (Proper Officer) I HEREBY CERTIFY AND DECLARE THAT IN MY OPINION THE PERSON NAMED BELOW IS SUFFERING FROM THE DISEASE STATED NAME (in full) DATE OF ONSET AGE DISEASE See Note NOTE SEX FULL ADDRESS WHERE PATIENT NOW IS:- IF PATIENT IS AT PRESENT IN A HOSPITAL 1. THE ADDRESS IN FULL FROM WHICH THE PATIENT WAS ADMITTED IS:- WHEN THE FORM IS USED FOR A CASE OF FOOD POISONING ENTER “F.P.” (OR “F.P. SUSPECTED”) UNLESS THE CASE IS DIAGNOSED AS ONE OF SPECIFIC DISEASE (e.g. DYSENTERY) WHICH IS REQUIRED TO BE NOTIFIED AS SUCH. 2. IN MY OPINION THE DISEASE WAS/WAS NOT CONTRACTED IN THE HOSPITAL (Delete whichever does not apply) Additional particulars required in cases of certain diseases. 3. DATE OF ADMISSION OPHTHALMIA NEONATORUM DATE OF BIRTH................................... NAME AND ADDRESS OF PARENT OR OTHER PERSON IN CHARGE OF THE CHILD. MARK “X” WHERE APPLICABLE MALARIA CONTRACTED: Abroad............................................................ Therapeutically........................................................... In this country................................................. Accidentally........................................................ IF INDUCED: ACUTE MENINGITIS ACUTE POLIOMYELITIS CAUSAL ORGANISM, if known ........................................................................................................................................................................ PARALYTIC OR NON-PARALYTIC? weakness or P N-P (PARALYTIC means that there are or have been signs of paralysis of muscles either permanent or transient (Ring symbol which applies) (NON- PARALYTIC means that there have been no ACUTE ENCEPHALITIS such signs.) INFECTIVE OR POST – INFECTIOUS? I P-I BELOW: IF POST INFECTIOUS, STATE PRECEDING INFECTION (Ring symbol which applies) TUBERCULOSIS DATE ORGAN OR PART AFFECTED..................................................................................................................... SIGNATURE OF DOCTOR ADDRESS:



















![Human Disease & Prevention[1].](http://s1.studyres.com/store/data/008490697_1-a09883a764253f65e6e0383c54276c4a-150x150.png)
