Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
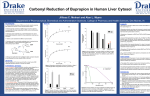
BUPROPION HYDROCHLORIDE Class antidepressant Dosage, Adult (usual) depression initial 100mg BID, maintenance 100mg TID, MAX 450mg/day depression SR formulation: initial dose 150mg QD, maintenance 150mg BID MAX 400mg/day smoking cessation 150mg QD x 3days then 150mg BID x 7-12 weeks Dose Adjustments: renal impairment liver disease Administration smoking cessation patients should set a quit date within first 2 weeks of treatment How Supplied 150 MG SUSTAINED-RELEASE TABLET 100 MG, 75 MG TABLET Indications depression smoking cessation Contraindications seizure disorders prior or current diagnosis of bulimia or anorexia concomitant MAO inhibitor hypersensitivity to bupropion products concomitant use of other bupropion products Adverse Effects N/V seizures/tremors agitation insomnia hypersensitivity reaction (arthralgia, myalgia, fever, rash) hypertension Drug Interactions clorgyline desipramine flecainide fluoxetine guanfacine haloperidol imipramine iproniazid isocarboxazid metoprolol moclobemide nialamide nortriptyline pargyline paroxetine phenelzine procarbazine propafenone risperidone selegiline sertraline thioridazine toloxatone tranylcypromine zolpidem Pregnancy Category B Breast Feeding controversial DRUGDEX DRUG EVALUATIONS BUPROPION 0.0 OVERVIEW A. Bupropion is an antidepressant agent which is structurally different from tricyclic antidepressants (TCA), selective serotonin reuptake inhibitors (SSRI), and monoamine oxidase inhibitors (MAOI). B. DOSING INFORMATION: Dosing should begin at 200 mg/day, (100 mg BID) or 150 mg of the sustained-release (SR) and may be increased to 300 mg/day (100 mg TID or 150 mg BID of the SR), based on clinical response. Doses should not exceed 450 mg/day. C. PHARMACOKINETICS: Rapidly absorbed from the gastrointestinal tract with peak plasma concentrations in approximately 2 hours. The volume of distribution is 19 to 21 L/kg with 80% plasma protein binding. The drug is extensively metabolized in the liver to at least 4 metabolites. Elimination half-life is 14 hours. D. CAUTIONS: Adverse effects of bupropion include nausea, vomiting, constipation, dry mouth, agitation, insomnia, headache/migraine and tremor. Seizures have been reported with bupropion; when taken in recommended doses, the incidence is similar to that with imipramine. E. CLINICAL APPLICATIONS: Bupropion is useful as an alternative to tricyclic, SSRI, and MAO inhibitor antidepressants for the treatment of depression. It also may be helpful as an augmentation agent to existing monotherapy for depression. It is indicated as an aid to smoking cessation treatment. 1.0 DOSING INFORMATION 1.1 DOSAGE FORMS A. Information on specific products and dosage forms can be obtained by referring to the Product Index. 1.2 STORAGE AND STABILITY A. ORAL 1. Protect from light and moisture and store at room temperature 15 to 25 degrees Centigrade (59 to 77 degrees Fahrenheit) (Prod Info Wellbutrin(R), 1999). Store bupropion sustained release at room temperature, 20 to 25 degrees Celsius (68 to 77 degrees Fahrenheit), in a tight, light-resistant container (USP) (Prod Info Wellbutrin(R) SR, 1999). 1.3 ADULT DOSAGE 1.3.1 NORMAL DOSE A. ORAL 1. The recommended initial dose is 200 milligrams/day, administered as 100 milligram doses once in the morning and once in the evening (Prod Info Wellbutrin(R), 1999). Based on clinical response, this dose may be increased to 300 milligrams/day, administered as three 100milligram doses. This increase should not occur sooner than 3 days after beginning therapy. 2. The recommended initial dose of bupropion sustained release is 150 milligrams (mg) given as a single daily dose in the morning. If the initial dose is tolerated, an increase to 150 mg twice daily is recommended as early as day 4. There should be an interval of at least 8 hours between doses. An increase in dosage to the maximum of 400 mg/day given as 200 mg twice daily may be considered for patients in whom no clinical improvement is noted after several weeks of treatment at 300 mg/day (Prod Info Wellbutrin(R) SR, 1999). 3. A maximum bupropion dose of 450 milligrams/day may be considered for patients who are unresponsive to several weeks of 300 milligrams/day (Prod Info Wellbutrin(R), 1999). Single doses of bupropion should not exceed 150 milligrams. The 100-milligram tablets must be administered 4 times daily with at least 4 hours between successive doses, in order not to exceed the limit of 150 milligrams in a single dose. 4. Bupropion should be discontinued in patients who have failed to demonstrate an adequate therapeutic response after an appropriate period of therapy of 450 milligrams/day. Escalating the dose higher than 450 milligrams/day is not recommended by the manufacturer due to the increased risk of seizures (Prod Info Wellbutrin(R), 1999). 5. In clinical trials, doses of bupropion have ranged from 300 to 750 milligrams/day in divided doses (Fann et al, 1981; Stern & HartoTruax, 1980; Zung, 1983; Stern et al, 1983). These dosages were more effective than placebo in treating depression as measured by the Hamilton Scale for Depression and Clinical Global Impression Scores. 6. For smoking cessation, the recommended dose is 150 milligrams (mg) twice daily; an initial dose of 150 mg/day for the first 3 days is recommended. Dosing intervals should be at least 8 hours apart. Approximately 1 week is needed to achieve steady-state blood levels, therefore, treatment should be initiated while the patient is still smoking and a quit date should be set for the second week. Treatment may be continued for 7 to 12 weeks. If by the seventh week no progress has been made towards quitting, then it is unlikely that the patient will quit (Prod Info Zyban(R), 1999). 7. No clinical data is available regarding maintenance therapy with bupropion for smoking cessation. However, the manufacturer states that since the drug has been used for longer periods of time in the treatment of depression, continuing treatment for greater than 12 weeks is feasible and should be determined on an individual basis (Prod Info Zyban(R), 1999). B. ADMINISTRATION TECHNIQUE 1. Splitting bupropion extended-release tablets may be a useful option for some patients (Chochren, 1999). A higher rate of release than that observed with whole tablets occurs during the first 15 minutes; thereafter the release characteristics in divided and whole tablets are similar. Tablets should be used soon after splitting due to their hygroscopic properties with degradation occurring rapidly if exposed to moisture. Crushing or chewing will nullify the extended release formulation. 1.3.2 DOSAGE IN RENAL FAILURE A. The manufacturer indicates that bupropion HCl and its metabolites are almost completely excreted through the kidney, and patients with renal failure should receive a reduced frequency and/or dose initially and be closely monitored for toxic effects (Prod Info Wellbutrin(R) SR, 2000; Prod Info Wellbutrin(R), 2000; Prod Info Zyban(R), 2000). 1.3.3 DOSAGE IN HEPATIC INSUFFICIENCY A. Bupropion is extensively metabolized and its metabolites are conjugated in the liver, therefore, patients with hepatic insufficiency should receive a reduced frequency and/or dose and be closely monitored for toxic effect (Prod Info Wellbutrin(R) SR, 2000; Prod Info Wellbutrin(R), 2000; Prod Info Zyban(R), 2000). B. Preliminary results of a comparative pharmacokinetic study in normal versus cirrhotic patients indicated that the half-lives of the metabolites were prolonged in cirrhotic patients (Prod Info Wellbutrin(R), 1999). C. Bupropion's disposition was monitored following a single oral 200 milligrams dose in 8 healthy volunteers and 8 age-matched and weightmatched volunteers with alcoholic liver disease. The mean elimination half-life of the morpholinol metabolite was significantly prolonged in subjects with liver disease while half-lives for bupropion, erythroamino alcohol and threoamino alcohol were minimally changed. Although these results were encouraging, alcoholic liver disease-patients should be initially dosed cautiously with bupropion (DeVane et al, 1990). 1.3.4 DOSAGE IN GERIATRIC PATIENTS A. SUMMARY: No overall difference in safety or effectiveness has been seen in older patients versus younger patients, and disposition of bupropion and its metabolites appears to be similar (Prod Info Wellbutrin (R), 1999). One study, however, did demonstrate that the elderly are at increased risk for accumulation of bupropion and its metabolites. B. Bupropion was effective in the treatment of depression in geriatric outpatients (55 years or older) at daily doses of up to 450 milligrams/day (Kirksey & Stern, 1984; Kane et al, 1983). C. The clinical safety and efficacy of bupropion 150 milligrams/day and 300 milligrams/day was studied in depressed patients 55 years of age or older. Both doses of bupropion were equal to imipramine in antidepressant activity. Patients on imipramine experienced more anticholinergic side effects while patients on bupropion experienced more insomnia and headaches (Branconnier et al, 1983). 1.3.5 DOSAGE ADJUSTMENT DURING DIALYSIS A. It is anticipated that dialysis clearance would be highly inefficient due to bupropion's large assumed Vd beta of 1.4 to 3.2 L/kg and slow diffusion from tissue binding sites and plasma. In a single patient on hemodialysis, bupropion AUC's did not significantly differ on days when the patient was dialyzed. AUCs for 3 of the active metabolites were 10 to 20% lower on dialysis days. These data indicate that dosage adjustment during hemodialysis is not necessary (Pers Comm, 1985). 1.3.6 DOSAGE IN OTHER DISEASE STATES A. DIABETES 1. Studies in mice have shown that bupropion stimulates insulin secretion in the presence of low, threshold, and high glucose concentration levels and therefore should be administered with caution to type II diabetic patients treated with hypoglycemic medications (El-Dakhakhny et al, 1996). B. DOSING TO REDUCE SEIZURE RISK 1. Retrospective analysis of clinical experiences suggests that the risk of seizure with bupropion may be minimized by not exceeding 450 milligrams (mg) daily of bupropion immediate-release and 400 mg of the sustained-release. Administration should be 3 times daily with the immediate release and twice daily with the sustained-release. No single dose of the sustained-release should exceed 200 mg. All doses should be increased gradually (Prod Info Wellbutrin(R) SR, 1999; Prod Info Wellbutrin(R), 1999). C. SMOKERS 1. Dosage adjustments are not necessary in cigarette smokers, no significant pharmacokinetic differences (Hsyu et al, 1997). 1.4 PEDIATRIC DOSAGE 1.4.1 NORMAL DOSE A. ORAL: 1. Safety and effectiveness in pediatric patients has not been established (Prod Info Wellbutrin (R), 1999). 2.0 PHARMACOKINETICS 2.1 ONSET AND DURATION 2.1.1 ONSET A. INITIAL RESPONSE: 1. Depression: 4 weeks (Prod Info Wellbutrin (R), 1999; Stern & HartoTruax, 1980). a. With high doses (above 300 mg): 8 days (Stern & HartoTruax, 1980). 2.1.2 DURATION A. MULTIPLE DOSE: 1. Depression: Improvement continued after 52 weeks (Gardner, 1983). 2.2 DRUG CONCENTRATION LEVELS 2.2.1 THERAPEUTIC A. THERAPEUTIC DRUG CONCENTRATION: 1. Depression, 10 to 20 ng/mL (not well-established) (Goodnick, 1992). B. TIME TO PEAK CONCENTRATION: 1. Oral, regular release: 2 hours (Prod Info Wellbutrin, 1999; Findlay et al, 1981). 2. Oral, sustained release: 3 hours (Prod Info Wellbutrin(R) SR, 1999). C. AREA UNDER THE CURVE: 1161/ng x hr/mL (Hsyu et al, 1997). 1. Area under the curve values were equivalent for the immediate release and sustained release formulations (Davidson & Connor, 1998). 2. No significant difference between smokers and nonsmokers (Hsyu et al, 1997). 2.3 ADME 2.3.1 ABSORPTION A. BIOAVAILABILITY (F): 1. Route, dosage form: rapidly absorbed (Lai & Schroeder, 1983). a. Absolute bioavailability has not been determined (Prod Info Wellbutrin(R), 1999). However, it appears that only a small proportion of the oral drug reaches the systemic circulation intact. b. Bupropion immediate-release and sustained-release products are bioequivalent (Prod Info Wellbutrin(R) SR, 1999). B. EFFECTS OF FOOD: None (Prod Info Wellbutrin(R) SR, 1999). 2.3.2 DISTRIBUTION 2.3.2.1 DISTRIBUTION SITES A. TOTAL PROTEIN BINDING: 80% (Prod Info Wellbutrin(R), 1999; Findlay et al, 1981). B. CEREBROSPINAL FLUID: 1. Concentrations of the parent drug in the brain are 10- to 25-fold higher than in plasma (Preskorn & Othmer, 1984; Ferris et al, 1983). 2.3.2.2 DISTRIBUTION KINETICS A. DISTRIBUTION HALF LIFE: 1.2 to 1.4 hours (Findlay et al, 1981). B. VOLUME OF DISTRIBUTION (Vd): 19 to 21 L/kg (Findlay et al, 1981). 2.3.3 METABOLISM 2.3.3.1 METABOLISM SITES AND KINETICS A. Liver, major site (Schroeder, 1983). 1. Primarily by the CYP2B6 isoenzyme (Prod Info Wellbutrin(R) SR, 1999; Prod Info Zyban (R), 1999). 2. Considerable first pass metabolism occurs (Schroeder, 1983). 2.3.3.2 METABOLITES A. Morpholinol, active (Prod Info Wellbutrin(R), 1999). 1. The morpholinol appears in the systemic curculation almost as rapidly as the parent drug. The morpholinol and the threo-amino have been found to be half as potent as bupropion in animal screening tests for antidepressant drugs (Smith et al, 1981; Prod Info Wellbutrin(R), 1999). The metabolites are 10 to 25 times less potent as inhibitors of dopamine uptake (Butz et al, 1982). B. Erythro- and threo-amino alcohols, active (Prod Info Wellbutrin(R), 1999). C. Erythro-amino diol bupropion, active (Prod Info Wellbutrin(R), 1999). 2.3.4 EXCRETION 2.3.4.1 BREAST MILK A. BREASTFEEDING: Controversial 1. Bupropion accumulates in human breast milk in concentrations much higher than in maternal plasma. Two metabolites were also found. Neither bupropion nor its metabolites were detected in the infants' plasma, indicating that accumulation did not occur in the infants (Briggs et al, 1993). 2.3.4.2 KIDNEY A. RENAL EXCRETION: 87% (Prod Info Wellbutrin(R), 1999). 2.3.4.3 OTHER A. Feces, 10% (Prod Info Wellbutrin(R), 1999; Preskorn & Othmer, 1984). 2.3.5 HALF-LIFE 2.3.5.1 PARENT COMPOUND A. ELIMINATION HALF-LIFE: 14 hours (Prod Info Wellbutrin(R), 1999; Hsyu et al, 1997; Preskorn & Othmer, 1984). 1. With chronic dosing, elimination half-life is 21 hours (Prod Info Wellbutrin(R) SR, 1999). 2. No significant difference between smokers and nonsmokers (Hsyu et al, 1997). 2.3.5.2 METABOLITES A. Hydroxybupropion (morpholinol), 24 hours (Prod Info Wellbutrin(R) SR, 1999; Prod Info Wellbutrin(R), 1999; Smith et al, 1981). 1. Half-lives were prolonged by cirrhosis (Prod Info Wellbutrin(R), 1999). B. Erythrohydrobupropion, 33 hours (Prod Info Wellbutrin(R) SR, 1999). C. Threohydrobupropion, 37 hours (Prod Info Wellbutrin(R) SR, 1999). 2.3.6 EXTRACORPOREAL ELIMINATION 2.3.6.1 HEMODIALYSIS A. DIALYZABLE: No (Prod Info Wellbutrin(R), 1999). 1. The manufacturer reports that there is no experience with the use of dialysis in the management of bupropion overdoses (Prod Info Wellbutrin(R), 1999). 2.3.6.3 HEMOPERFUSION A. DIALYZABLE: No (Prod Info Wellbutrin(R), 1999). 1. The manufacturer reports that there is no experience with the use of hemoperfusion in the management of bupropion overdoses (Prod Info Wellbutrin(R), 1999). 3.0 CAUTIONS 3.1 CONTRAINDICATIONS A. History of seizure disorder B. Hypersensitivity to bupropion C. History of bulimia or anorexia nervosa D. Concomitant monoamine oxidase (MAO) inhibitors E. Concomitant use of other bupropion products (i.e. Zyban(R)) 3.2 PRECAUTIONS A. Renal impairment B. Hepatic impairment C. History of psychosis and/or mania D. History of cranial trauma E. Patients treated with other medications or treatments that lower seizure threshold 3.3 ADVERSE REACTIONS 3.3.1 BLOOD A. HEMATOLOGIC 1. Post-marketing reports of ecchymosis, leukocytosis, and leukopenia have been described; a causal relationship has not been established (Prod Info Wellbutrin(R), 1999). B. LEUKOPENIA 1. In a long term study (6 months or greater), bupropion 150 to 750 mg/day (mean, 250 to 400 mg/day) was associated with a statistically significant decrease in white blood cell count of 10 to 15%. A decrease in lymphocytes by 6% and an increase in neutrophils by the same amount were also observed during the 3 to 6 month treatment period (Othmer et al, 1983). 3.3.2 CARDIOVASCULAR A. CARDIOVASCULAR EFFECTS 1. In a study utilizing combined sustained-release bupropion and a nicotine transdermal system, treatment emergent HYPERTENSION developed in 6.1% of patients. Most had evidence of preexisting hypertension. No causal relationship has been established; however, the following adverse events have been reported in post-marketing surveillance: orthostatic hypotension and third degree heart block (Prod Info Wellbutrin(R) SR, 2000; Prod Info Wellbutrin(R), 2000; Prod Info Zyban(R), 2000). 2. The cardiovascular effects of bupropion were studied in 36 depressed patients with pre-existing heart disease. All subjects had major depression and pre-existing left ventricular impairment (15), ventricular arrhythmias (15), and/or conduction disease (21). The patients continued their cardiac drug regimens and received bupropion for 3 weeks at a mean dose of 442 mg/d. Although bupropion caused a rise in supine blood pressure, it did not cause significant conduction complications, did not exacerbate ventricular arrhythmias, had a low rate of orthostatic hypotension, and had no effect on pulse rate. However, bupropion treatment was discontinued for 14% of the patients because of adverse effects, including exacerbation of baseline hypertension in 2 patients. It was concluded that bupropion is a useful agent in the treatment of depressed patients with cardiovascular disease (Prod Info Wellbutrin(R) SR, 2000; Prod Info Wellbutrin(R), 2000; Prod Info Zyban(R), 2000; Roose et al, 1991). 3. Data indicate that bupropion treated patients do not manifest clinically significant ORTHOSTATIC HYPOTENSION (Chouinard et al, 1981; Branconnier et al, 1983). Bupropion was administered in doses ranging from 300 mg/day to 600 mg/day to 5 patients who had demonstrated a documented fall of at least 20 mmHg in systolic blood pressure accompanied by symptoms such as dizziness, nausea and lightheadedness while receiving tricyclic antidepressant therapy. During bupropion treatment none of the patients presented with clinically significant orthostatic hypotension, and the mean difference between supine and standing systolic blood pressure after 14 days of bupropion treatment was 8.3 +/- 2.5 mmHg which did not differ significantly from that seen after 7 days of placebo treatment (8.3 +/3.2 mmHg) (Chouinard et al, 1981). 4. Although bupropion does not produce orthostatic hypotension, subjective symptoms of syncope, dizziness and fainting were reported in 6.4% of patients (14/220) receiving bupropion 300 to 750 mg/day (Zung, 1983). These effects are not associated with any objective changes in cardiovascular function (Preskorn & Othmer, 1984). Syncope may be related to phenomena other than that occurring with the tricyclic antidepressants, which results from orthostatic effects (Preskorn & Othmer, 1984). 5. Patients with clinically significant orthostatic hypotension on tricyclic antidepressants may be safely switched to bupropion which has been shown to produce no clinically significant alterations in systolic blood pressure, pulse rate, or orthostasis (Farid et al, 1983). 6. No clinical effects on heart rate, irrespective of therapeutic dose, were found in 700 patients in short-term or long-term studies (Wenger & Stern, 1983). These findings are consistent with other studies (Branconnier et al, 1983). 7. Imipramine (IMI) and bupropion (BUP) were compared for cardiac side effects in 10 depressed patients with impaired left ventricular function (LVF) in a random, double-blind, crossover study. Neither IMI nor BUP adversely affected ejection fraction or other indices of LVF. Orthostatic hypotension requiring discontinuation of the drug occurred in 50% of patients taking IMI. This did not occur with BUP. BUP may be a safe alternative to IMI in depressed patients with congestive heart failure (Roose et al, 1987). 8. Unlike tricyclic antidepressants, bupropion does not cause significant prolongation of cardiac conduction (Wenger et al, 1982 & 1983; Wenger & Stern, 1983; Branconnier et al, 1983). In a randomized double-blind, parallel study (Wenger et al, 1982), the cardiac effects of amitriptyline 75 to 225 mg/day were compared with bupropion 300 to 750 mg/day. Baseline measurements in both treatment groups (23 patients/group) were similar; however, prolongation and QRS duration and depression in QRS height were significantly greater with amitriptyline. 3.3.3 CENTRAL NERVOUS SYSTEM A. CENTRAL NERVOUS SYSTEM EFFECTS 1. Adverse events commonly seen with bupropion include irritability, depression, agitation, insomnia, HEADACHE/MIGRAINE, AND TREMOR. Common events causing discontinuation have included agitation, abnormalities in mental status, seizures, headaches and sleep disturbances. In clinical trials, 9.7% more bupropion treated patients experienced AGITATION than patients receiving a placebo (Prod Info Wellbutrin(R), 1999; Prod Info Zyban(R), 1999). In 2% of patients, symptoms were severe enough to require discontinuation. In studies using bupropion sustained release 400 mg, 9% of patients experienced agitation and 6% experienced ANXIETY (Prod Info Wellbutrin(R) SR, 1999). Other central nervous system effects seen include ataxia/incoordination, myoclonus, dyskinesia, dystonia, mania/hypomania, hallucinations, and depression (Prod Info Wellbutrin(R), 1999). Post-marketing surveillance has received reports of the following adverse events (no causal relationship established): coma, delirium, dream abnormalities, paresthesia, and unmasking of tardive dyskinesia. 2. Anxiety, headache, and agitation are some of the most common events leading to drug discontinuation (Settle et al, 1999). 3. AGITATION has been reported as an adverse effect of bupropion therapy and resulted in discontinuation of therapy in 2 of 71 patients in one study (Stern & Harto-Truax, 1980). Two studies also reported agitation as an adverse effect associated with bupropion therapy (Halaris et al, 1981; Van Wyck Fleet et al, 1983). These subjective complaints may be minimized by increasing the dose slowly (Preskorn & Othmer, 1984). 4. In a non-blinded study comparing bupropion (12 patients), other antidepressants (amitriptyline, 7 patients; maprotiline, 2 patients; amoxapine, 2 patients; and imipramine, 1 patient), and drug-free normal controls (12 patients), perceptual changes were noted by all patients 3 to 12 days after starting bupropion (mean daily dose of 561 mg) and were characterized as vivid dreaming, alteration in time sense, increased emotionality, increased intensity of sensory experience, and experience of competing stimuli (Becker & Dufresne, 1982). Other investigators have not confirmed these findings (Preskorn & Othmer, 1984). 5. A case of bupropion (BUP) DELIRIUM characterized by disorganized thinking, memory impairment, fear, and agitation, but not disorientation, delusion, hallucinations, or other perceptual distortions, was reported (Dager & Heritch, 1990). Symptom onset was dose-related and sustained therapeutic response was subsequently obtained at a lower dose of BUP without recurrence of delirium. Abnormal bupropion metabolism and elevated plasma metabolite levels did not account for the adverse reaction and it may have been from agonist effects. A case of acute delirium and parkinsonism in a bupropion-treated patient who had received a liver transplant has been reported (Strouse et al, 1993). 6. Three cases of organic mental disorders in patients receiving bupropion for treatment of the depressed phase of bipolar disorder have been reported (Ames et al, 1992). These reactions were characterized primarily by visual disturbances, visual hallucinations, and illusions, although one patient also experienced auditory hallucintations. They were unrelated to changes in mood. These patients were also taking other medications that may have contributed to the development of these reactions: lithium, benzodiazepines, beta-blockers, H-2 blockers. Patients with a history of bipolar disorder or psychosis may be at greater risk to develop these reactions while taking bupropion, especially in the presence of the aforementioned medications. 7. A case of bupropion-associated CATATONIA in a 19-year-old male patient with major depression was reported (Jackson et al, 1992). After a dose increase from 75 mg/day up to 225 mg/day, the patient exhibited bizarre behavior the fifth day of treatment. He was admitted to the hospital and developed increased muscle tone, posturing, and waxy flexibility. Bupropion was discontinued and a course of 14 bilateral ECT was given with resolution of psychotic symptoms, improvement in mood, and complete resolution of motor disturbances. B. COMPULSIVE BEHAVIOR 1. Bupropion-induced repetitive compulsive behavior was reported in a 7-year-old boy treated for atttention deficit hyperactivity disorder (Jackson et al, 1994). Dosage was started at 75 mg/d and increased to 75 mg TID. Three weeks later patient exhibited repetitive, compulsive "ordering" behavior which interefered with functioning. On DC of bupropion, compulsive behavior completely remitted. C. DIZZINESS 1. Dizziness was reported in 11% of patients taking bupropion sustained release 400 mg/day (Prod Info Wellbutrin(R) SR, 1999). D. EXTRAPYRAMIDAL SYMPTOMS 1. A 70-year-old woman experienced a reversible orofacial dyskinesia affecting her eyes and tongue while receiving bupropion 75 to 225 milligrams/day (Gardos, 1997). Other symptoms included hand tremor, nausea and dizziness. After discontinuation, the dyskinesia receded and other side effects disappeared. 2. Two geriatric patients (85 and 72 years old) treated with bupropion for major depression experienced a "falling backward" reaction (Szuba & Leuchter, 1992). Maximum dosage in each patient was 400 mg/day and 350 mg/day, respectively. Neither patient had a history of orthostatic hypotension or vertigo. Both patients did manifest other symptoms consistent with a parkinsonian syndrome (akinesia, shuffling gait). After discontinuation of bupropion these adverse effects resolved within 1 to 2 weeks. The mechanism may involve dopaminergic dysfunction in the basal ganglia, leading to PARKINSONIAN EFFECTS. At therapeutic dosage, bupropion primarily exhibits dopamine agonist activity. However, high dosage coupled with slowed metabolism in the elderly may have caused a dopamine antagonist effect and resulted in the adverse reactions. Document Continues... Copyright © MICROMEDEX Inc. 1974 - 2001 All rights reserved. MICROMEDEX(R) Healthcare Series Vol. 109 expires 9/2001 - Content for use only by healthcare professionals in conjunction with clinical data. See complete Warranties and disclaimers. /mdxdocs/contents.htm /mdxdocs/contents.htm/mdxcgi/mdxhtml.exe?&tmpl=mdxhome.tm1&SCRNAME=mdxhome&CTL=c:\mdx\ mdxcgi\megat.sys /mdxcgi/mdxhtml.exe?&tmpl=mdxhome.tm1&SCRNAME=mdxhome&CTL=c:\mdx\mdxcgi\megat.sys/mdxc gi/mdxhtml.exe?&tmpl=hcssrch1.tm1&SCRNAME=hcssrch1&CTL=c:\mdx\mdxcgi\megat.sys /mdxcgi/mdxhtml.exe?&tmpl=hcssrch1.tm1&SCRNAME=hcssrch1&CTL=c:\mdx\mdxcgi\megat.sys/mdxcgi/ cgidict.exe?CTL=c:\mdx\mdxcgi\megat.sys&SET=1C113924301C3E90 /mdxcgi/cgidict.exe?CTL=c:\mdx\mdxcgi\megat.sys&SET=1C113924301C3E90/mdxcgi/display.exe?CTL=c:\ mdx\mdxcgi\megat.sys&SET=1C113924301C3E90&SYS=1&T=276 /mdxcgi/display.exe?CTL=c:\mdx\mdxcgi\megat.sys&SET=1C113924301C3E90&SYS=1&T=276/mdxcgi/dis play.exe?CTL=c:\mdx\mdxcgi\megat.sys&SET=1C113924301C3E90&SYS=1&T=276&PRINTREADY=4 /mdxcgi/display.exe?CTL=c:\mdx\mdxcgi\megat.sys&SET=1C113924301C3E90&SYS=1&T=276&PRINTRE ADY=4/mdxcgi/prodindx.exe?CTL=c:\mdx\mdxcgi\megat.sys&SET=1C113924301C3E90&SYS=1&T=276 /mdxcgi/prodindx.exe?CTL=c:\mdx\mdxcgi\megat.sys&SET=1C113924301C3E90&SYS=1&T=276