Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cryptosporidiosis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Listeria monocytogenes wikipedia , lookup
Schistosomiasis wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Gastroenteritis wikipedia , lookup
Hepatitis C wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Hepatitis B wikipedia , lookup
Anaerobic infection wikipedia , lookup
Oesophagostomum wikipedia , lookup
Neonatal infection wikipedia , lookup
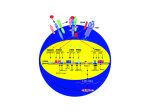
Infectious Risks in Patients Receiving TNF-alpha inhibitors Michael J. Tan, MD, FACP, FIDSA Associate Professor of Internal Medicine, Northeast Ohio Medical University Summa Health, Akron, OH Objectives Review mechanism of action of TNF-alpha inhibitors Understand the role of TNF in the inflammatory response Be familiar with infections associated with TNF inhibitors Review methods to prevent infection in these patients. 2 What is a biologic? Biologics Monoclonal antibodies against specific target cells or cytokines. May also be receptor constructions 3 Two contrasting outcomes of signaling through tumor necrosis factor receptor 1 (TNFR1). Engagement of TNFR1 by trimeric tumor necrosis factor- (TNF-) can trigger apoptosis and/or nuclear factor B (NF-B) activation. Both processes involve the adapter protein TNFR-associated death domain (TRADD), which associates with TNFR1 via interactions between "death domains" (D.D.) on both proteins. For NF-B activation, TNFR-associated factor 2 (TRAF2) and receptorinteracting protein (RIP) are required. Induction of apoptosis occurs when the death domain-containing protein Fasassociated death domain protein (FADD) associates with TRADD. FADD also contains a "death effector domain" (D.E.D.) that interacts with caspase 8 to initiate the apoptotic process. Cys = cysteine. (Adapted from Yuan J: Transducing signals of life and death. Curr Opin Cell Biol 9:247, 1997; and Nagata S: Apoptosis by death factor. Cell 88:355, 1997.) 4 TNF-alpha TNF, TNF-alpha, cachectin Systemic inflammatory cytokine able to induce apoptotic cell death Produced by macrophages, lymphoid cells, mast cells, endothelial cells, cardiac myocytes, adipose, fibroblasts, neuronal tissue. Able to induce inflammation Able to inhibit tumorigenesis and viral replication Acts with other cytokines, including IFN-gamma, to generate cell-mediate immune response to pathogens such as M tuberculosis, Listeria sp, Histoplasma sp. Lack of TNF prevents formation of granuloma 5 TNF Acute phase response, associated with fever No known human state of TNF deficiency 1997 “knock-out” mouse model lacking TNF were markedly more susceptible to mycobacterial infection and infection with intra-cellular pathogens including Listeria, Salmonella, some viruses, and pneumococcus 6 TNF-alpha antagonists Infliximab – Remicade Chimeric anti-TNF-alpha monoclonal antibody Often given with other immunesuppressants to prevent immune response to murine protein and may increase risk of infection. Etanercept – Enbrel Two TNF-alpha receptor domains fused to a portion of human IgG1 Binds soluble TNF alpha with receptor domains, binds circulating TNF-alpha but less membrane bound TNF-alpha. Adalimumab – Humira Fully human anti-TNF alpha monoclonal antibody Golimumab – Simponi Certolizumab pegol – Cimzia Pegylated FAb region, human monoclonal antibody. 7 8 Who uses them? Patients with Rheumatoid arthritis Ankylosing spondylitis Crohn Disease Psoriasis, psoriatic arthritis Some use in EtOH associated hepatitis, Behcet, uveitis, pyoderma gangrenosum, Still’s disease, sarcoidosis, Sjogren, severe hidradenitis, GVH 9 Diseases associated with TNF-alpha antagonists Mycobacterial infections, mostly MTb Miliary, disseminated, urinary tract, osteoarticular, tonsillitis, and peritonitis have been reported. Fungi, including endemic mycoses Viruses PCP Listeria TNF Blocker infections: Intracellular organisms: Mycobacteria, Histo, Candida, Listeria, Aspergillus, Cyrptococcus, Nocardia, Salmonella Isaacs D. Infectious Risks Associated with Biologics, in Curtis N, et al eds. Hot Topics in Infection and Immunity in Children IX, Advances in Experimental Medicine and Biology, 2013 Rychly DJ, DiPiro JT. Infections Associated with Tumor Necrosis Factor-alpha Antagonists. Pharmacotherapy 2005; 25(9):1181-1192 Crum NF, Lederman ER, Wallace MR. Infections Associated with Tumor Necrosis Factor-alpha Antagonists. Medicine 2005;84:291-302. 10 Case Review Crum et al, 2005 MTb Cryptococcosis Coccidioidomycosis Pneumococcal bacteremia • Bacterial infections due to Strep, Staph, Moraxella, including pneumonia, abscess, cellulitis, sinusitis Histoplasmosis, Aspergillosis, NTM, Candidiasis, PCP, Listeriosis, Legionellosis Intracellular pathogens such as Salmonella, Toxoplasma, Bartonella, Leishmania have been reported Nocardia, Sporothrix, Zygomycetes CMV, HSV, Molluscum contagiosum Post-operative infections—little risk Are some of these infections due to the TNF or are the patients naturally at greater risk because of the disease states? Crum NF, Lederman ER, Wallace MR. Infections Associated with Tumor Necrosis Factor-alpha Antagonists. Medicine 2005;84:291-302. 11 What is the risk of Tb? Infliximab RCT, case series, case reports reviewed 3 cases of MTb in 3882 receiving infliximab vs. 0/2430 placebo/control Post-licensure Tb rates: • US with RA 6.2/100k • RA + inflixumab 24.4/100k – 4x higher. MTb generally developed 12 weeks into therapy. Rychly DJ, DiPiro JT. Infections Associated with Tumor Necrosis Factor-alpha Antagonists. Pharmacotherapy 2005; 25(9):1181-1192 12 What is the risk of Tb? Etanercept review 0 cases in RCT 2 cases in reviewed that had tonsillitis/enteritis January 1998-Sept 2002, 39 cases in surveillance system Adalimumab review 1/1750 vs. 0/832 control. 8/477 (1.7%) in Development trials. 5/1900 in surveillance Cases of MTb were reported to have occurred longer after initiation of therapy than with infliximab (30-46 wks mean) 13 Other infectious risks Debatable. May be based on epidemiology Recommendation-Prevention is key 14 Screens Tb TST at baseline and every 12 mos, baseline CXR Histoplasmosis Consider CXR, urine histo ag at baseline and f/u q3-4 mos for those in endemic areas Coccidioidomycosis CXR and serolgic testing with IgM/IgG at baseline and f/u q3-4 mos for those in endemic areas Cryptococcus No data Listeria Patient education regarding food prep and safety Crum NF, Lederman ER, Wallace MR. Infections Associated with Tumor Necrosis Factor-alpha Antagonists. Medicine 2005;84:291-302. 15 Prevention All patients on TNF Screen for MTb with TST or IGRA, baseline and q12mos Consider prophlyaxis for Pneumocystis Immunization • Consider pneumococcal conjugate vaccine • Consider HBV series. 16 Prophylaxis? Tb No/Treat LTBI Histoplasmosis Itraconazole daily?? Lifestyle modification, avoid high risk activity. Coccidioidomycosis fluconazole daily? More likely secondary prophy. Cryptococcus fluconazole? More likely secondary prophy. Listeria TMP-SMX? Little data, but would help with PCP, nocardia 17 Case A 60 year old woman with RA presents to your office. Her rheumatologist would like to start a TNF inhibitor. A TST was performed and reported to be 12x12mm. She is sent to you for evaluation. 18 An approach to +PPD/IGRA Common: Patient with RA to start TNF, but PPD or IGRA positive Ascertain exposure history If +PPD, consider getting IGRA due to poor PPD/TST placement or reading of test. (10mm, but immune compromised consider 5mm). Check Chest radiography (PA/LAT) as baseline • If negative, proceed with LTBI therapy. Safest: Initiate INH daily x9 months. • Check LFT at baseline, 2 weeks, q every other month. Generally defer TNF, but if must start, allow 4-6 weeks of INH before starting TNF Check repeat CXR 1-2 months after starting TNF Finish INH, and follow CXR. Probably little benefit of repeat TST or IGRA since positivity will persist. 19 Vaccination Live, such as HSV or VZV? Or… “Help! My RA patient on TNF-inhibitor just got VZV Vaccination!” 20 Vaccinations DOI: 10.1093/cid/cit684, Rubin, et al 2013 IDSA Clinical Practice Guideline for Vaccination of the Immunocompromised Host 21 Pneumococcus Vaccination recommendation: Previously vaccinated with PPSV23: • Dose PCV 13, redose PPSV23 >8 weeks later and >5 years after previous PPSV23. Vaccine naïve: • Dose PCV13, redose PPSV23 >8 weeks later. 22 American College of Rheumatology 23 http://www.rheumatology.org/Publications/Hotline/Update_on_Herpes_Zoster_%28Shingles%29_Vaccine_for_Autoimmune_Disease_Patients/ In general, for vaccinations Give prior to planned immunesuppression Live: >=4 weeks of immunesuppression, and avoid within 2 weeks of initiation of immunesuppression On immunesuppression: No live, but perhaps hold for a few weeks, vaccinate, and restart. Inactivated: >=2 weeks prior to initiation of immunesuppression If one immunesuppression, inactived can be given 24 VZV Vaccination appropriate >4 weeks prior to immunesuppression Little said about vaccination of someone that is currently on therapy. Some will hold therapy for 4-8 weeks prior to vaccination, then restart 4 weeks afterward. Risk of vaccine acquired VZV and HSV higher with TNFinhibitor patients. >100 cases, but VZV severity “acceptable” Try not to panic No need to use antiviral Watch patients closely. 25 Do you need to hold therapy prior to surgery, colonscopy, cataracts? What’s the risk? Infection Impaired wound healing Recommendation: Hold for 1-2 weeks prior to surgery, resume 1-2 weeks after surgery or when PO • How is this impacted by the long effect of the agents? • Data overall are limited and may not necessarily support holding agents. – Recommend to hold for at least one dosage cycle. • HSS J. Sep 2006; 2(2): 141–147. • BSR/BHPR: doi:10.1093/rheumatology/keq249b 26 Medscape’s take 27 Does presence of TNF inhibitors need to change manner of thinking of pathogens for common infections? Common things are still common History should be your trigger Has there been travel to endemic area? Does the patient have epidemiologic risk factors? How long have the symptoms been present, and how did they progress? Has the patient had previous treatment for LTBI? Endemic mycosis? Vaccinations? 28 Questions? 29 Suggested Reading Isaacs D. Infectious Risks Associated with Biologics, in Curtis N, et al eds. Hot Topics in Infection and Immunity in Children IX, Advances in Experimental Medicine and Biology, 2013 Rychly DJ, DiPiro JT. Infections Associated with Tumor Necrosis Factor-alpha Antagonists. Pharmacotherapy 2005; 25(9):1181-1192 Crum NF, Lederman ER, Wallace MR. Infections Associated with Tumor Necrosis Factor-alpha Antagonists. Medicine 2005;84:291-302. 2013 IDSA Clinical Practice Guideline for Vaccination of the Immunocompromised Host. DOI:10.1092/cid/cit684 30