Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
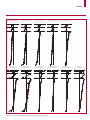
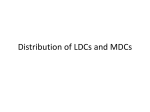
Articles Global cancer transitions according to the Human Development Index (2008–2030): a population-based study Freddie Bray, Ahmedin Jemal, Nathan Grey, Jacques Ferlay, David Forman Summary Background Cancer is set to become a major cause of morbidity and mortality in the coming decades in every region of the world. We aimed to assess the changing patterns of cancer according to varying levels of human development. Methods We used four levels (low, medium, high, and very high) of the Human Development Index (HDI), a composite indicator of life expectancy, education, and gross domestic product per head, to highlight cancer-specific patterns in 2008 (on the basis of GLOBOCAN estimates) and trends 1988–2002 (on the basis of the series in Cancer Incidence in Five Continents), and to produce future burden scenario for 2030 according to projected demographic changes alone and trends-based changes for selected cancer sites. Findings In the highest HDI regions in 2008, cancers of the female breast, lung, colorectum, and prostate accounted for half the overall cancer burden, whereas in medium HDI regions, cancers of the oesophagus, stomach, and liver were also common, and together these seven cancers comprised 62% of the total cancer burden in medium to very high HDI areas. In low HDI regions, cervical cancer was more common than both breast cancer and liver cancer. Nine different cancers were the most commonly diagnosed in men across 184 countries, with cancers of the prostate, lung, and liver being the most common. Breast and cervical cancers were the most common in women. In medium HDI and high HDI settings, decreases in cervical and stomach cancer incidence seem to be offset by increases in the incidence of cancers of the female breast, prostate, and colorectum. If the cancer-specific and sex-specific trends estimated in this study continue, we predict an increase in the incidence of all-cancer cases from 12·7 million new cases in 2008 to 22·2 million by 2030. Published Online June 1, 2012 DOI:10.1016/S14702045(12)70211-5 Section of Cancer Information, International Agency for Research on Cancer, Lyon, France (F Bray PhD, J Ferlay ME, D Forman PhD); and Department of Surveillance and Health Policy Research, American Cancer Society, Atlanta, GA, USA (A Jemal PhD, N Grey PhD) Correspondence to: Dr Freddie Bray, Section of Cancer Information, International Agency for Research on Cancer, 150 cours Albert Thomas, 69372, Lyon Cedex 08, France [email protected] Interpretation Our findings suggest that rapid societal and economic transition in many countries means that any reductions in infection-related cancers are offset by an increasing number of new cases that are more associated with reproductive, dietary, and hormonal factors. Targeted interventions can lead to a decrease in the projected increases in cancer burden through effective primary prevention strategies, alongside the implementation of vaccination, early detection, and effective treatment programmes. Funding None. Introduction Global action is needed to stem the increasing burden of non-communicable diseases, especially in low-income and middle-income countries1–9 which now bear 80% of the worldwide burden of such diseases.10 Cancer, already the leading cause of death in many high-income countries, is set to become a major cause of morbidity and mortality in the next few decades in every region of the world, irrespective of level of resource.10–12 The UN has forecast that the global population will reach 7 billion by 2012 and 8·3 billion by 2030.13 The effect of population ageing and growth will be greatest in low-income and middle-income countries. These changes translate to a predicted global burden of 20·3 million new cancer cases by 2030 compared with an estimated 12·7 million cases in 2008, and a predicted 13·2 million cancer-related deaths worldwide by 2030, up from 7·6 million in 2008.11 Such a demographic transition and the resulting upsurge in cancer incidence and mortality are contingent on population projections that assume decreases in human fertility and population growth as a result of continuous social and economic development,14 and on incidence and mortality rates of all cancer types combined remaining unaltered over the next few decades. The static trends in the risk of cancer in future decades seems the less robust of these two assumptions, especially in view of the cancer-specific incidence and mortality trends seen over the past half century. Rather than describing constant rates over time, many reports have documented lagged changes in lung and other tobacco-related cancers according to the country-specific and sex-specific phases of the tobacco epidemic, uniform decreases in stomach cancer as a result of primary prevention efforts, and a rising incidence of breast, colorectal, and prostate cancers, initially in affluent populations and, within the last couple of decades, in historically less-affluent populations at lower cancer risk. The changes are likely to be attributable to a combination of unfavourable changes in several ill defined reproductive, dietary, metabolic, hormonal, and other behavioural determinants that increase the risk of these cancers. The so-called cancer transition—an analogy to Omran’s epidemiological www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5 1 Articles See Online for appendix transition15—thus fits well with the occurrence of socioeconomic transition in several historically lowresource to medium-resource populations. The result has been a reduction in the prevalence of predominantly infection-based diseases, and a concomitant rise in those with apparently little or no established associations with infection.16 By linking geographical and temporal patterns of cancer to corresponding levels of social and economic progress, we provide an overview of the key characteristics of the global cancer transition. We used the Human Development Index (HDI)17 as an indicator of socioeconomic development, and rates of cancer incidence and mortality as markers of the extent of the cancer transition globally. We aimed to draw attention to geographical variations and trends in cancer-specific rates in each of the HDI areas and in different world regions, and to offer a global, trends-based profile of the possible cancer burden in 2030. Methods Data sources For the GLOBOCAN database see http://globocan.iarc.fr For Cancer Incidence in Five Continents see http://ci5.iarc.fr The International Agency for Research on Cancer has compiled estimates of the worldwide incidence and mortality for 27 cancers in 184 countries in 2008 by age group and sex in the GLOBOCAN 2008 database.11 Details are provided elsewhere.11 The methods used to estimate cancer-specific incidence and mortality rates at the national level are dependent on the availability and accuracy of local data sources. Generally, there is a paucity of high quality cancer incidence and mortality data in low-resource and medium-resource areas—eg, no population-based cancer registries exist in 34 of the 184 countries examined in this paper, 32 of 34 countries are low-resource or mediumresource countries, and no vital statistics systems exist in 88 countries, of which 85 are either lowresource or middle-resource countries. To examine patterns in the incidence of different types of cancer in 2008 by levels of socioeconomic development, we linked the country-specific GLOBOCAN estimates to the corresponding HDI, as estimated for 2007 by the UN Development Programme (UNDP).17 The HDI is a summary measure of human development, which (for the 2007 UNDP estimates) is a composite index of three basic dimensions of human development, namely a long and healthy life (based on life expectancy at birth), access to knowledge (based on a combination of adult literacy rate and primary education to tertiary education enrolment rates), and a decent standard of living (based on GDP per head adjusted for purchasing-power parity [US$]). We used the predefined categories of the distribution of HDI by country: low (HDI<0·5), medium (0·5≤HDI<0·8), high (0·8≤HDI<0·9), and very high (HDI≥0·9). The global breakdown by country within each development level is shown in figure 1 and the specific countries are listed in the appendix. We use these HDI levels to characterise aspects of the cancer burden according to level of resource and extent of societal development. We also combined the high HDI and very high HDI levels, and low HDI and medium HDI levels, to create lower HDI and higher HDI areas, as alternatives to the traditional grouping of more developed (North America, Europe, Australia, New Zealand, and Japan) and less developed regions (all other areas of the world). To examine incidence trends in common cancers, we extracted incident cases of the seven most commonly diagnosed cancers worldwide: cancers of the lung, female breast, colorectum, stomach, prostate, liver, and cervix. Together, these cancers constitute more than 58% of the estimated global cancer burden. Corresponding population datasets were obtained from CI5 Plus, which contains annual incidence for population-based cancer registries published in Cancer Incidence in Five Continents (CI5) for the longest year Low HDI (0·3–0·499) Medium HDI (0·5–0·799) High HDI (0·8–0·899) Very high HDI (0·9–0·999) Figure 1: Global Human Development Index (HDI) levels This map shows only the countries included in the analysis. 2 www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5 Articles A World cancer incidence New cases in 2008 (thousands) 1000 500 0 500 1000 Lung 830 Female breast 832 Colorectum 825 778 551 409 366 Stomach Prostate 766 622 132 572 B World cancer incidence Cumulative risk up to age 75 years 5 4 3 2 1 0 1 2 3 4 5 Lung 3·5 Female breast 3·4 Colorectum 3·1 Prostate 3·4 375 Cervix uteri 215 141 Leukaemia 175 175 Corpus uteri 157 132 245 493 Stomach 0·9 1·4 Liver 163 532 Liver 0·6 1·4 Liver 106 Non-Hodgkin lymphoma Stomach 1·5 Oesophagus 127 1·2 1·1 Breast 389 Bladder Non-Hodgkin lymphoma 0·7 0·4 0·5 World cancer mortality Cumulative risk up to age 75 years 5 4 3 2 1 0 1 2 3 4 5 695 Colorectum 141 681 D Lung 0·4 178 256 2·3 1·4 1·8 Liver Bladder World cancer mortality Deaths in 2008 (thousands) 1000 500 0 500 1000 Stomach Cervix uteri Oesophagus C 368 230 Oesophagus 89 1·1 Cervix uteri 62 Lung 240 Colorectum 228 Breast 317 213 2·7 2·0 1·2 0·6 0·8 0·6 0·4 Oesophagus Pancreas 0·7 0·9 0·2 0·9 Pancreas 190 77 Cervix uteri 0·2 0·6 0·9 0·4 Prostate 179 79 Prostate 0·4 0·2 0·8 0·3 Leukaemia 113 0·2 91 101 0·3 0·2 80 95 Leukaemia Brain, nervous system Non-Hodgkin lymphoma 0·3 Non-Hodgkin lymphoma Brain, nervous system Bladder 0·3 0·2 87 63 Ovary 0·3 0·2 65 Bladder 0·2 0·2 Lip and oral cavity 0·2 0·3 Kidney 0·3 0·1 Corpus uteri 0·7 0·4 Kidney 0·8 0·2 Pancreas 194 84 Pancreas 0·7 0·2 Kidney 201 72 Lip and oral cavity 0·5 0·4 144 Ovary 75 Lip and oral cavity 114 149 Leukaemia 0·6 0·3 Lip and oral cavity 39 89 Brain, nervous system Ovary 109 129 Ovary 0·5 0·2 Kidney 79 37 119 106 Melanoma of skin 0·6 0·1 Gallbladder 61 48 Gallbladder 0·2 0·1 Thyroid 140 73 Brain, nervous system 0· 4 0·3 Other pharynx 30 65 Other pharynx 0·1 0·2 Melanoma of skin 178 22 Thyroid 0·5 0·1 Larynx 35 46 Larynx 0·2 0·1 Larynx 75 76 Larynx 0·3 0·2 Corpus uteri 8 36 Corpus uteri 0·1 0·1 Gallbladder 81 64 Other pharynx 0·3 0·2 Multiple myeloma 50 22 Multiple myeloma 0·2 0·1 Nasopharynx 7 45 Other pharynx 57 79 Gallbladder 0·3 0·2 Multiple myeloma 76 27 Multiple myeloma 0·3 0·1 Melanoma of skin Nasopharynx 13 71 Nasopharynx 0·1 0·2 Thyroid Hodgkin lymphoma 35 33 Testis 38 Kaposi sarcoma Hodgkin lymphoma 0·1 <0·1 Hodgkin lymphoma 14 Testis 0·1 <0·1 Kaposi sarcoma 34 Kaposi sarcoma <0·1 Testis Melanoma of skin 0·1 0·0 12 Nasopharynx <0·1 0·1 14 22 Thyroid <0·1 0·1 35 9 21 Hodgkin lymphoma 29 Kaposi sarcoma <0·1 Testis <0·1 <0·1 4 6 <0·1 <0·1 Higher HDI Lower HDI Figure 2: Distribution of cancer types by Human Development Index (HDI) level (A) Number of new cases. (B) Lifetime cumulative risk of incidence. (C) Number of deaths. (D) Lifetime cumulative risk of death. Kaposi sarcoma not estimated in higher HDI countries. span available by registry, year of diagnosis (1988–2002), and 5-year age group. Inclusion in CI5 was chosen as a general marker of each registry’s data quality over time, because the CI5 process includes a detailed assessment of the comparability, completeness, and validity of the submitted datasets. We estimated age-standardised incidence and mortality rates per 100 000 population using the world standard population,18,19 and estimated the lifetime cumulative risk for individuals aged 0–74 years, assuming an absence of competing causes of death.20 To obtain the estimated annual percentage change in incidence between 1988 and 2002, registry-specific, sex-specific, and cancer-specific log-linear models were fitted with an identify link, with the age-standardised incidence rates the response, and the year of occurrence included as a covariate, with 95% CIs obtained for the annual percentage change. We present the future burden of cancer in 2030 by sex for all cancers combined for the four levels of HDI on the basis of the rates in 2008, assuming population growth and ageing in 2030 occurs according to the UN World Population Prospects medium-fertility variant.13 On the basis of application of the average trends seen for several common cancers in medium, high, and very high HDI areas to the rates in 2008, we also provide a trend-based scenario of the future cancer burden in 2030. www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5 3 Articles Role of the funding source There was no funding source for this study. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. Results Within higher (high and very high) HDI areas, cancers of the lung, female breast, and colorectum each account for a very similar number of new cases (about 830 000) in 2008, with prostate cancer accounting for about 766 000 cases (figure 2). Together, these four cancers comprised almost half (49%) the total cancer burden in these areas. In lower (low and medium) HDI areas, lung cancer was also the most commonly diagnosed cancer (778 000). However, several types of cancer were more common in lower HDI areas than they were in higher HDI areas, including stomach cancer and liver cancer, which are more common than both female Population in 2008 (millions [% of world population]) Population in 2030 (millions [% of world population]) Incidence in 2008 (millions [% of total global burden]) Incidence in 2030*: demographic (millions [absolute % increase from 2008]) Incidence in 2030†: demographic plus trend (millions [absolute % change from 2008]) Men Low HDI 196 (5·7%) 332 (7·9%) 0·11 (1·6%) 0·21 (94%) 0·23 (111%) 2266 (66·4%) 2811 (67·2%) 3·0 (44·7%) 5·4 (82%) 5·4 (82%) High HDI 452 (13·2%) 504 (12·1%) 1·0 (14·4%) 1·6 (68%) 1·8 (90%) Very high HDI 498 (14·6%) 532 (12·7%) 2·6 (39·3%) 3·8 (46%) 4·5 (75%) 11·0 (66%) 12·0 (81%) Medium HDI Worldwide 3412 4179 6·6 Women Low HDI Medium HDI§ 198 (5·9%) 332 (8·0%) 0·14 (2·3%) 0·27 (92%) 0·27 (92%) 2176 (64·8%) 2722 (66·0%) 2·8 (45·6%) 4·8 (73%) 4·9 (79%) High HDI 470 (14·0%) 527 (12·8%) 0·9 (15·6%) 1·4 (53%) 1·6 (70%) Very high HDI 512 (15·3%) 542 (13·2%) 2·2 (36·6%) 2·9 (31%) 3·4 (54%) 6·0 9·4 (55%) 10·2 (69%) Worldwide 3356 4123 Total Low HDI Medium HDI High HDI 394 (5·8%) 664 (8·0%) 0·25 (2·0%) 4442 (65·6%) 5533 (66·6%) 5·7 (45·1%) 0·48 (93%) 0·49 (100%) 10·1 (78%) 10·3 (81%) 3·4 (80%) 922 (13·6%) 1031 (12·4%) 1·9 (14·9%) 3·0 (60%) Very high HDI 1010 (14·9%) 1074 (12·9%) 4·8 (38·0%) 6·7 (39%) 7·9 (65%) Worldwide 6768 8302 20·3 (61%) 22·2 (75%) 12·7 *Based on demographic changes (UN)—the predicted cases worldwide are derived by aggregation of the predicted cases obtained after the first application of age-specific rates to the demographic forecasts within each Human Development Index (HDI) level (these numbers will not correspond exactly with those predicted from the single global figures, because the underlying rates used to derive the predictions from the two sources differ in their age structure and size). †Based on demographic changes (UN) plus crude assumptions on trends in rates of six cancers on the basis of changing annual age-adjusted incidence in 101 cancer registries 1988–2002 (figure 5; table 2): annual decreases in stomach (2·5%, [worldwide in both sexes]), cervical cancer (2% [worldwide]) and lung cancer (1% [high HDI and very high HDI areas in men only]); increases in colorectal (1% [worldwide both sexes]), lung (1% [high HDI and very high HDI areas in women only]), female breast (2% [worldwide]), and prostate cancer (3% [worldwide]). See appendix for a list of countries by HDI region. Table 1: Estimated numbers of new cases of cancers (all sites excluding non-melanomas) in 2008 and predicted new cases by 2030 4 breast cancer and colorectal cancer in such areas; cancers of the cervix and oesophagus are also major contributors to the cancer burden in lower HDI areas (figure 2). In combination, these seven cancers account for nearly two-thirds (62%) of the estimated total cancer burden in lower HDI areas. The lifetime cumulative risk of incidence of cancers of the lung, female breast, colorectum, and prostate are all more than 3% in higher HDI areas—for the remaining cancers, only the risk of stomach cancer exceeds 1% (figure 2). In lower HDI areas, lifetime risk of lung cancer is highest at 2·3%, with the lifetime risk of five common cancers—cancers of the stomach, liver, female breast, colorectum, and oesophagus—varying from 1% to 2%. A greater proportion of the mortality burden is seen in low HDI and medium HDI areas, especially for cancers of the liver, stomach, and oesophagus (figure 2). The most common causes of cancer death in higher HDI areas are those of the lung, colorectum, stomach, and female breast, which comprise about 45% of the total cancer mortality burden. The four most common types of cancer death in lower HDI areas include cancers of the lung and stomach, but also liver cancer and oesophageal cancer, which together constitute 49% of the cancer mortality burden in these areas. The lifetime risk of lung cancer death ranks highest in both higher HDI and lower HDI areas. The second highest lifetime risk of cancer death was for colorectal cancer in higher HDI areas, with stomach and liver cancer equal second in lower HDI areas; lifetime risk of stomach cancer death ranked third in both higher HDI and lower HDI areas (figure 2). Very high HDI areas seem to bear a larger proportion of the cancer burden, with almost 40% of the global incidence estimated to occur in these countries, despite having only 15% of the world’s population (table 1). The same five cancers (cancers of the colorectum, lung, female breast, prostate, and stomach) are the most commonly diagnosed cancers in both very high and high HDI areas (figure 3). With an estimated 635 000 cases, cancer of the colorectum is the most common cancer in very high HDI areas; and cancers of the lung, female breast, and prostate all contribute about 597 000 cases or more. Lung cancer is the most common neoplasm in medium HDI areas with an estimated 773 000 new cases, ahead of stomach, liver, and female breast cancer, each contributing more than half a million new cases annually. The cancer profile is quite different in low HDI areas, where cervical cancer is the most common cancer, with female breast cancer, liver cancer, Kaposi sarcoma, and non-Hodgkin lymphoma the four other most common cancers (figure 3). In terms of age-adjusted incidence rates in men, nine different types of cancer are estimated as most often diagnosed, the most common of which being prostate cancer (most common in 82 countries, mainly in countries with high HDI levels, but also in central and www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5 Articles southern Africa), lung cancer (most common in 47 countries, mainly in eastern Europe and Asia, including China, India and Indonesia), and liver cancer (most common in 22 countries, mainly in eastern Africa and southeast Asia; figure 4). In women, either breast cancer or cervical cancer are the most common cancer diagnoses in almost all countries (breast cancer was the most common cancer diagnosis in 135 countries and cervical cancer was the most common cancer diagnosis in 45 countries; figure 4). In terms of age-adjusted mortality, eight different cancer types worldwide are represented as the most common cause of cancer death by country among men (figure 4). In terms of age-adjusted cancer mortality in men, lung cancer is the most common cause of cancer A death in 94 countries, prostate cancer is the most common cause in 31 countries, liver cancer is the most common cause in 24 countries, and stomach cancer is the most common cause in 18 countries (figure 4). In women, cancers of the breast and cervix are the most common causes of cancer death worldwide, with breast cancer the most common cause in 99 countries and cervical cancer the most common cause in 55 countries (figure 4). Lung cancer is the most common cause of cancer deaths in women in 17 countries. Other distinct geographical patterns are also evident—eg, clusters of high incidences of male oesophageal cancer in five countries in eastern Africa and Kaposi sarcoma in nine sub-Saharan countries, and high mortality rates of stomach cancer in South America (figure 4). Very high Human Development Index Men Colorectum Women 347 Lung 288 385 224 600 Breast Prostate 597 149 Stomach B 80 High Human Development Index Breast 232 Lung 168 Colorectum 96 168 Prostate 82 55 Stomach C 53 94 Medium Human Development Index Lung 238 535 Stomach 403 Liver 208 158 391 Breast 527 Colorectum D 218 182 Low Human Development Index 33 Cervix uteri Breast 24 Liver 15 8 Kaposi sarcoma 13 6 Non-Hodgkin Lymphoma 7 5 600 4 2 0 2 New cases in 2008 (thousands) 4 600 Figure 3: Five most frequently diagnosed cancers in terms of new cases estimated in 2008, by Human Development Index level Maps shows only the countries included in the analysis. www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5 5 Articles A Prostate Lung Liver Stomach Kaposi sarcoma Oesophagus Colorectum Oral cavity Bladder B Lung Prostate Liver Stomach Kaposi sarcoma Oesophagus Colorectum Bladder C Breast Cervix uteri Thyroid Liver D Breast Cervix uteri Lung Stomach Liver Thyroid Non-Hodgkin lymphoma Gallbladder Figure 4: Incidence and mortality from the most common forms of cancer, by sex (A) Incidence in men. (B) Mortality in men. (C) Incidence in women. (D) Mortality in women. Maps show only the countries included in the analysis. 6 Figure 5 plots the estimated annual percentage change (with 95% confidence limits) based on the trends in annual age-adjusted incidence rates of lung, female breast, colorectal, stomach, prostate, liver, and cervical cancer 1988–2002 by sex in 101 cancer registries which reside in countries in medium, high or very high HDI areas. Table 2 presents the simple overall mean of these according to HDI area. Although the absence of registries in low HDI areas, together with the few registries in medium HDI areas (six registries) and high HDI areas (11 registries) weaken the interpretation of trends in estimated annual percentage change, some patterns in the observed trends emerge. Incidence rates of female breast cancer and prostate cancer have been increasing in almost all countries, irrespective of HDI level, with average increases for breast cancer of about 2%; increases for prostate cancer varied between 3·2% and 7% (table 2). We also observed recorded increases in colorectal cancer in many registry populations, although the increases are more evident in registries in medium HDI areas and high HDI areas (figure 5 and table 2). We recorded decreases in the incidence of cervical and stomach cancers (in both sexes) in most of the populations examined, with mean annual decreases in rates between about 1% and 3% in medium HDI, high HDI, and very high HDI countries. The trends for liver cancer are more varied and perhaps less generalisable than are those for cervical and stomach cancers (figure 5). Lung cancer incidence rates in men tend to be decreasing in most registries, but are increasing in women—at least in populations with very high HDI levels (figure 5 and table 2). The projected demographic changes will mean the global incidence of cancer in both men and women will increase from an estimated 12·7 million in 2008 to 20·3 million by 2030 (table 1), a net increase of about 60%. The increases in cancer incidence are proportionally greatest in lower HDI settings, a 93% increase in both sexes (table 1). Worldwide, we project annual increases in the rates of colorectal cancer, female breast cancer, and prostate cancer, and, in high HDI to very high HDI areas, for lung cancer in women (table 2). We project annual decreases worldwide in stomach cancer and cervical cancer, and, in high HDI to very high HDI areas, for lung cancer in men (table 2). Assuming rates in 2030 of all other cancers remain as estimated in 2008 (including liver cancer, in view of the fact that the recorded trends are diffuse between and within HDI areas), we would see an increase in the annual incidence of 75% from 2008 to 22·2 million by 2030 (table 1). Figure 5: The estimated annual percentage change (EAPC) in trends in annual age-adjusted incidence rates of the seven most common cancers, by level of Human Development Index (1988–2002) Each point estimate (with 95% CIs) is one of 101 cancer registries. www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5 Articles Stomach (men) EAPC incidence 1988−2002 −10 −6 −2 2 6 10 Stomach (women) EAPC incidence 1988–2002 −10 −6 −2 2 6 10 Cervix EAPC incidence 1988−2002 −10−8−6−4−2 0 2 4 6 8 10 Lung (men) EAPC incidence 1988−2002 −10 −6 −2 2 6 10 Lung (women) EAPC incidence 1988−2002 −10 −6 −2 2 6 10 Medium Medium Medium Medium Medium High High High High High Very high Very high Very high Very high Very high Liver (men) EAPC incidence 1988−2002 −10 −6 −2 2 6 10 Liver (women) EAPC incidence 1988−2002 −10 −6 −2 2 6 10 Colorectum (men) EAPC incidence 1988−2002 −10 −6 −2 2 6 10 Colorectum (women) EAPC incidence 1988−2002 −10 −6 −2 2 6 10 Female breast EAPC incidence 1988−2002 −10 −6 −2 2 6 10 Prostate EAPC incidence 1988−2002 −10 −6 −2 2 6 10 Medium Medium Medium Medium Medium Medium High High High High High High Very high Very high Very high Very high Very high Very high www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5 7 Articles Men Women Medium HDI High HDI Very high HDI –2·7% –2·6% ·· ·· Lung –1·5% –1·3% Liver 0·1% Colorectum 1·5% Stomach Cervix uteri Breast Prostate Scenario-based prediction for 2030* Medium HDI High HDI Very high HDI –2·8% –1·9% –2·5% –2·5% 2·5% annual decrease in all HDI areas per year ·· –1·8% –1·2% –2·6% 2% annual decrease in all HDI areas per year –1·6% –0·5% 0·5% 1·8% 1% annual decrease in high HDI and very high HDI areas (men) 1% annual increase in high HDI and very high HDI areas (women) 0·2% 2·5% –0·4% 0·4% 2·1% Difficult to generalise, assume no change 2·8% 0·6% 1·5% 1·8% 0·3% 1% annual increase in all HDI areas per year ·· ·· ·· 2·1% 2·6% 1·6% 2% annual increase in all HDI areas per year 3·2% 7·0% 4·4% ·· ·· ·· 3% annual increase in all HDI areas per year Data are estimated annual percentage change. HDI=Human Development Index. *Cancer-specific scenarios for the annual percentage change in incidence rates up to 2030 are derived from unweighted averages of the estimated annual percentage change (EAPC) by sex and HDI level when clear directional trends emerged; for cancers of the lung (low-to-medium HDI) and liver (all HDI levels), we assumed no change in the incidence rates by 2030, in view of the heterogeneity in the direction and magnitude of the trends, and the need for country-specific information on the tobacco epidemic (for lung cancer); for prostate cancer, we assumed a conservative 3% increase in the incidence rates per annum (at least relative to the increases in very high HDI settings) for all HDI levels—future trends in prostate cancer incidence will be strongly associated with the (unknown) future trends in testing for prostate-specific antigen. Table 2: Changing trends in cancer-specific age-adjusted incidence Discussion Cancers of the breast, lung, colorectum, and prostate account for about 50% of the cancer burden in high HDI and very high HDI regions, whereas in medium HDI regions, cancers of the oesophagus, stomach, and liver are also common, and together these seven cancers account for about 62% of the burden in low HDI and high HDI areas. Within low HDI regions, cervical cancer is more common than both breast cancer and liver cancer. We identified the nine most common cancers in men in the 184 countries studied, with cancers of the prostate, lung, and liver most prevalent. In women, either breast cancer or cervical cancer was the most commonly diagnosed neoplasm in almost all countries. In medium HDI and high HDI settings, the observed decreases in cervical and stomach cancer incidence seem to be offset by an increase in the incidence of female breast, prostate, and colorectal cancers. To our knowledge, this study is the first global overview of cancer to investigate patterns of incidence and mortality in relation to predefined levels of the HDI (panel). There has been a scarcity of research examining how macroeconomic determinants correlate with cancer incidence, mortality, and survival, and how the relation varies by cancer type and country. Assessment of these burden indicators against the specific components of HDI (education, health, and living standards) should enable examination of their relative importance. Other inequality measures might also be of relevance, such as inequality-adjusted HDI, which equals the HDI when there is no inequality across a population, but is less than the HDI when inequality is present.21 Cancer is a heterogeneous mix of diseases with different types of cancer more common in some populations than in others, sometimes substantially so.22 Cancers have very different causes, some of which are well understood and 8 some of which are poorly understood, and differences in the regional and temporal distribution of risk factors will determine the geographical and secular patterns of cancer. Therefore, many barriers exist to the understanding of global patterns of cancer—the availability of information about disease incidence and mortality, an understanding of the underlying causes and how these can change, and knowledge of the demographics of populations in terms of size and age structure.23 Incidence estimates will probably become more accurate as the number of high quality populationbased cancer registries expands (especially in low-income and middle-income countries) and the completeness and validity of registration improves in areas already covered. Forecasted population data are themselves predictions based on forecasts of birth and death rates and levels of immigration and emigration. Projections—and subsequently cancer predictions—can thus be materially altered when information from more up-to-date censuses is obtained. Forecasts are dependent not only on demographics and risk factors, but also on the extent and modalities of early detection and screening for cancer, which vary from country to country. Increasing levels of screening at the population level have the potential to independently increase the future cancer incidence burden in many settings, especially for those cancers in which a precursor lesion is not the target of the intervention. This would include prostate and breast cancers, for which incidence is already increasing in many populations. We are aware of some ambiguity in the examination of these trends in countries transiting socially and economically with time, because we have categorised each country according to the HDI index of 2007. The trend analyses for a given population should, therefore, be considered in relation to the levels of human development attained for that country in 2007. www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5 Articles Despite the substantive deficiencies in these domains, much can be learned from analyses of global patterns of cancer, and the contrasting patterns in relation to levels of human development. In both high HDI and very high HDI regions, four cancers (cancers of the female breast, lung, colorectum, and prostate) explain almost half the overall cancer burden. In medium HDI regions, lung and female breast cancers remain among the most common types of cancer along with stomach and liver cancers, which are both associated with infectious causes.24,25 In low HDI regions, female breast and liver cancers are also common but two additional infectionrelated cancers—cervical cancer and Kaposi sarcoma— are also prevalent. Some cancers seem to be positively associated with the level of socioeconomic development and colorectal cancer is a good example of this, with 40% of the global burden occurring in very high HDI regions despite such regions comprising only 15% of the world’s population. The reasons for this association are not clear, although dietary and metabolic factors associated with a so-called western lifestyle might be of particular relevance.26 Prostate cancer is another example of a cancer that is positively associated with HDI and for which the high incidence is partly a function of increased access to testing facilities for prostate-specific antigen in higher-resource regions.27 However, prostate cancer is also the most common cancer and cause of cancer death in men in several sub-Saharan African countries—both inherited susceptibility and environmental and lifestyle exposures could contribute to the increased rates in these regions. Cervical cancer, however, is negatively associated with HDI such that it is the most common cancer in low HDI regions and the most common cancer and cause of cancer death in women in several low HDI and middle HDI countries. Infection with human papillomavirus (HPV) is well established as a cause of cervical cancer28 and changing sexual behaviour leading to increasing persistent infection with high-risk HPV, together with inadequate facilities for screening, early detection, and treatment underpin this association. Other infection-related cancers are also associated with lower HDI (stomach cancer, liver cancer, and Kaposi sarcoma); Sylla and Wild29 proposed that control of relevant infections should become a crucial component of cancer prevention programmes in subSaharan Africa, where the impact of infection is greatest. Female breast cancer is the only type of cancer that is common in all regions, irrespective of level of HDI. It is the most common form of female cancer in the vast majority of countries in the world and thus the global control of breast cancer through both early detection and primary prevention is a high priority. Lung cancer and other tobacco-associated cancers, although not placed among the leading cancers in low HDI regions at present, will become a serious problem unless tobacco smoking is effectively controlled. Lung cancer is the most common form of cancer worldwide, it is the leading Panel: Research in context Systematic review We reviewed available studies for key papers on the descriptive epidemiology of cancer, as well as the evidence for resource-dependent primary prevention, early detection, and screening interventions for cancer. We searched Medline for studies in English, with no date restrictions. Interpretation To our knowledge, this study is the first global overview of present and future patterns of cancer incidence and mortality in relation to predefined levels of the Human Development Index (a marker of socioeconomic development). Public health clinicians and cancer control specialists should be alerted to the increasing magnitude of cancer incidence and mortality worldwide, the differing cancer profiles that emerge according to level of human development, and the changing cancer profiles as countries continue to change both socially and economically. Cancer is already the leading cause of death in many high-income countries and is set to become a major cause of morbidity and mortality in the next decades in every region of the world; this study serves as an important reference point in drawing attention to the need for global action to reduce the increasing burden of cancer. It should also serve as a catalyst for further work on human inequality and cancer from a global perspective, to better determine how and why macroeconomic determinants affect cancer incidence, mortality, and survival. cause of cancer deaths in men in many countries, and is the most common form of cancer death in women in North America, parts of Europe, and China. In terms of cancer incidence trends over time, analysis of the high quality cancer registry data draws attention to some important aspects of the global cancer transition. A tendency towards increases in breast, colorectal, and prostate cancers exist in the very high HDI, high HDI, and medium HDI regions (where data are available). These effects seem to be stronger in countries with very high HDI levels relative to those of medium HDI or high HDI, which might be indicative of an incidence plateau having being reached, at least in some very high HDI populations. Colorectal cancer trends, in particular, seem to be stable or decreasing in several very high HDI populations. Nevertheless, the trends point to the westernisation effect in countries with high HDI or medium HDI levels, and with increasing average levels of social and economic development, the population prevalence of several reproductive, dietary, metabolic, and hormonal risk factors (towards levels more similar to those commonly seen in high-income countries) could correspondingly increase the risk of these cancers. To some extent, these increases in incidence are countered by another hallmark of cancer transition, a reduction in infection-based cancers. Decreases in the incidence of stomach and cervical cancers are uniformly www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5 9 Articles seen in populations with very high, high, and medium HDI levels. The reduction in cervical cancer burden has been attributed to corresponding decreases in risk in older generations of women and, within higher-resource settings, the beneficial effects of mass screening cytology programmes.30 The uniform decreases of stomach cancer during the past 50 years are commonly ascribed to both a reduction in Helicobacter pylori infection in successive birth cohorts related to changing childhood environment, and to improved food preservation practices and better nutrition.30 The onset of refrigeration for food transport and storage could have been vital in reduction of salt consumption by largely eradicating the need for salting, smoking, and pickling of foods.30,31 Liver cancer is the other infection-related cancer examined here, and for which the incidence trends show much more heterogeneity across populations within each of the three HDI categories assessed. The assumptions that trends will stay unchanged is, however, perhaps unduly pessimistic in view of the prospects for prevention of hepatocellular carcinoma through mass immunisation against hepatitis B virus infection. In Taiwan, for instance, the preventability of hepatocellular carcinoma (after vaccination of all newborn babies in 1984) has been shown beyond childhood to early adulthood in a 20-year follow-up study.32 In China, where most liver neoplasms are diagnosed (about 0·35 million incident cases and deaths estimated per year11), neonatal hepatitis B vaccination programmes have been expanded as part of the China-GAVI project.33 With a few exceptions, lung cancer rates in men have been decreasing in the populations with very high, high, and medium HDI levels examined here, but have been increasing in women in the same populations. These contrasting sex-specific trends in very high HDI settings are in line with the respective population-specific rise and fall in adult cigarette consumption in the past decades. Evidently, other tobacco-related cancers—including cancers of the bladder, oesophagus, and oral cavity, which are the 8th, 9th, and 14th most frequent neoplasms worldwide, respectively—will alter patterns of tobacco consumption in different regions and countries change. This study attempted to incorporate cancer-specific time trends on the basis of recorded data to inform on the future cancer burden, but a more detailed appraisal would take into account the specific preventative actions in operation in the respective countries and regions of the world, and is an important next step. The trend-based scenario extrapolates recorded rates by use of crude averages of the estimated annual percentage change that are heterogeneous across registries in every HDI category, and thus should be interpreted with caution. One clear concern is the reliance on extrapolation of trends in just six population-based cancer registries (including two each from China and India) to be representative of all medium-resource settings. Clearly, more data and greater precision are needed, although we 10 believe that the scenarios selected in table 2 for making projections to 2030 are sufficiently reasonable to take at least preliminary account of the rate changes for some of the major cancers globally. Forouzanfar and colleagues34 presented trends in breast and cervical cancer between 1980 and 2010 in 187 countries using a unified modelling framework that, as well as being comprehensive, potentially provides greater comparability between countries. However, comparisons of their modelled cumulative risk estimates (ages 15–79 years) of breast cancer incidence with data from four longstanding Nordic population-based cancer registries showed a systematic overestimation in all four countries,35 and the uniformly decreasing trends in cervical cancer incidence in Uganda reported by Forouzanfar and colleagues were at odds with the rapidly increasing trends reported in Kampala 1991–2006,36 which were based on registry data that were considered to be of high quality.37 Our approach to the trend analyses and future extrapolations centres around use of observed data, and although more restrictive than Forouzanfar and colleagues’, adheres to the principle that results obtained from models should reasonably agree with actual observations that are thought to be of reasonable accuracy. The scarcity of historical time-trend data for any low HDI populations is an important drawback in view of the different contemporary patterns of cancer in these populations, mainly in sub-Saharan Africa, and correction of this deficiency will be crucial to the development of cancer control plans in this region. The projected decreases in cervical cancer worldwide might be rather over-optimistic in low HDI settings where screening and early treatment have not yet had an effect. In terms of the global burden predictions, however, the low HDI populations constitute 5·7% of the world’s population and 1·6% of the cancer burden, and the absence of this information will have a minor effect. However, the potential effect of major changes in the rates of common cancers in the vast populations of China and India is enormous. The tobacco epidemic and its effect on tobacco-related cancers in China, for instance, will heavily affect the predicted number of global cancer cases by 2030. The prevalence of smoking in men, for example, has risen sharply in many medium-HDI countries, including China and Indonesia. The future burden of lung cancer and other smoking-related cancers in men (in low HDI and medium HDI areas) and women (globally) will largely depend on smoking practices at the population level, including the duration of smoking, the extent of cessation, the types of tobacco smoked, and the patterns of consumption.38 The incidence and mortality estimates from GLOBOCAN for 2008 are also subject to precision limitations. In the compilation of country-specific cancer incidence and mortality, a hierarchy of methods is used in GLOBOCAN with accuracy dependent on the quality and availability of the source information at a given time, and www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5 Articles as such requires constant review. For example, national estimates of cancer incidence in India are based on corresponding rates obtained from the urban and rural population-based cancer registries, whereas national mortality is derived from incidence and survival estimates. In view of the possible concerns with the accuracy of cancer deaths in India (and in other low-income and middle-income countries) related to the number of deaths occurring at home and without medical attention, the mortality estimates reported by Dikshit and colleagues,39 which were based on a nationally representative sample of 1·5 million households, could complement the GLOBOCAN estimates, although the methodological differences need further assessment.40 More generally, there is a scarcity of high quality population-based cancer registries in Africa, Asia, and Latin America, with about 1%, 4%, and 6% of the populations of these respective regions covered, and there are few national vital registration systems with adequate mortality data in lowresource and medium-resource countries, especially in Africa and Asia. Although GLOBOCAN is a comprehensive data source for examination of the cancer burden worldwide and in the promotion of global cancer control, population-based cancer registries have been shown to be a crucial component in national cancer control strategies, where the registered incidence information provides the means to plan, monitor, and assess the effect of specific interventions in targeted populations.10,41 This study underscores the diversity of cancer as a worldwide occurrence and the extent to which the disease patterns vary from country to country. Classification of these populations by broad levels of human development does, however, draw attention to some of the key determinants of such variations, especially in countries rapidly transiting from lower to higher levels of human development. The reduction in infection-related cancers seems to be being offset by concomitant increases in cancers related to a westernisation of lifestyle and changes in tobacco consumption and the effect on lung and other cancers. Although forecasted demographic changes will probably increase the number of people with cancer to more than 20 million per year by 2030, targeted interventions can substantially reduce this number through resourcedependent interventions. Such actions include primary prevention strategies to effectively control the prevalence of lifestyle factors including tobacco avoidance and cessation of smoking, a reduction in alcohol consumption and obesity, and the promotion of increased levels of physical activity; as well as the implementation of vaccination programmes (for liver and cervical cancer), and early detection programmes (for colorectal, breast, and cervical cancer). Further reductions in mortality could be brought about by increasing access to curative treatment for specific cancers (including cervical, breast, and colorectal cancer), while increasing access to palliative care for those patients dying of cancer will reduce the inequities. Contributors FB contributed to the data collection, study design, analysis, and writing of the paper. JF contributed to data collection, analysis, and writing of the paper. AJ and NG contributed to the writing of the paper. DF contributed to drafting and finalising the paper. All authors read and approved the final paper. Conflicts of interest We declare that we have no conflicts of interest. References 1 Adams C, Grey N, Magrath I, Miller A, Torode J. The World Cancer Declaration: is the world catching up? Lancet Oncol 2010; 11: 1018–20. 2 Alwan A, Maclean DR, Riley LM, et al. Monitoring and surveillance of chronic non-communicable diseases: progress and capacity in high-burden countries. Lancet 2010; 376: 1861–68. 3 Beaglehole R, Bonita R, Alleyne G, et al. UN High-Level Meeting on Non-Communicable Diseases: addressing four questions. Lancet 2011; 378: 449–55. 4 Beaglehole R, Bonita R, Horton R, et al. Priority actions for the non-communicable disease crisis. Lancet 2011; 377: 1438–47. 5 Farmer P, Frenk J, Knaul FM, et al. Expansion of cancer care and control in countries of low and middle income: a call to action. Lancet 2010; 376: 1186–93. 6 Yach D, Hawkes C, Gould CL, Hofman KJ. The global burden of chronic diseases: overcoming impediments to prevention and control. JAMA 2004; 291: 2616–22. 7 GAVI’s challenges: funding and leadership. Lancet 2010; 376: 1438. 8 Miranda JJ, Kinra S, Casas JP, Davey SG, Ebrahim S. Non-communicable diseases in low-income and middle-income countries: context, determinants and health policy. Trop Med Int Health 2008; 13: 1225–34. 9 Morris K. UN raises priority of non-communicable diseases. Lancet 2010; 375: 1859. 10 WHO. Global Status Report on Non-Communicable Diseases 2010. http://www.who.int/nmh/publications/ncd_report2010/en/ (accessed May 25, 2012). 11 Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010; 127: 2893–917. 12 Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011; 61: 69–90. 13 United Nations Population Division. World Population Prospects: The 2008 Revision. New York: United Nations, 2007. 14 Myrskyla M, Kohler HP, Billari FC. Advances in development reverse fertility declines. Nature 2009; 460: 741–43. 15 Omran AR. The epidemiologic transition: a theory of the epidemiology of population change. Milbank Mem Fund Q 1971; 49: 509–38. 16 Gersten O, Wilmoth JR. The cancer transition in Japan since 1951. Demographic Research 2002; 7: 271–306. 17 United Nations Development Programme. Human development report 2009: overcoming barriers—human mobility and development. New York: United Nations, 2009. 18 Segi MKM. Cancer mortality for selected sites in 24 countries (1950–1957). Tokyo: Tohoku University School of Medicine, 1966. 19 Doll R, Payne P, Waterhouse J. Cancer incidence in five continents: a technical report. New York: Springer, 1966. 20 Day NE. Cumulative rate and cumulative risk. In: Waterhouse J, ed. Cancer incidence in five continents (volume IV). Lyon: International Agency for Research on Cancer, 1982: 668–70. 21 United Nations Development Programme. Human development report 2011. http://hdr.undp.org/en/statistics/ (accessed April 26, 2012). 22 Doll R, Peto R. The causes of cancer: quantitative estimates of avoidable risks of cancer in the United States today. J Natl Cancer Inst 1981; 66: 1191–308. 23 Bray F, Moller B. Predicting the future burden of cancer. Nat Rev Cancer 2006; 6: 63–74. 24 Polk DB, Peek RM Jr. Helicobacter pylori: gastric cancer and beyond. Nat Rev Cancer 2010; 10: 403–14. 25 Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol 2006; 45: 529–38. www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5 11 Articles 26 27 28 29 30 31 32 33 34 12 Chan AT, Giovannucci EL. Primary prevention of colorectal cancer. Gastroenterology 2010; 138: 2029–43. Signorello LB, Adami H-O. Prostate cancer. In: Adami H-O, Hunter D, Trichopolous D, eds. Textbook of cancer epidemiology. Oxford: Oxford University Press, 2002: 400–28. Walboomers JM, Jacobs MV, Manos MM, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol 1999; 189: 12–19. Sylla BS, Wild CP. A million Africans a year dying from cancer by 2030: what can cancer research and control offer to the continent? Int J Cancer 2012; 130: 245–50. Parkin DM, Bray FI, Devesa SS. Cancer burden in the year 2000: the global picture. Eur J Cancer 2001; 37 (suppl 8): 4–66. Howson CP, Hiyama T, Wynder EL. The decline in gastric cancer: epidemiology of an unplanned triumph. Epidemiol Rev 1986; 8: 1–27. Chang MH, You SL, Chen CJ, et al. Decreased incidence of hepatocellular carcinoma in hepatitis B vaccinees: a 20-year follow-up study. J Natl Cancer Inst 2009; 101: 1348–55. Progress in hepatitis B prevention through universal infant vaccination—China, 1997–2006. Morb Mortal Wkly Rep 2007; 56: 441–45. Forouzanfar MH, Foreman KJ, Delossantos AM, et al. Breast and cervical cancer in 187 countries between 1980 and 2010: a systematic analysis. Lancet 2011; 378: 1461–84. 35 36 37 38 39 40 41 Ferlay J, Forman D, Mathers CD, Bray F. Breast and cervical cancer in 187 countries between 1980 and 2010: a systematic analysis. Lancet 2012; 379: 1390–91. Parkin DM, Nambooze S, Wabwire-Mangen F, Wabinga HR. Changing cancer incidence in Kampala, Uganda, 1991–2006. Int J Cancer 2010; 126: 1187–95. Curado MP, Edwards B, Shin HR, et al. Cancer incidence in five continents. Lyon: International Agency for Research on Cancer, 2007. Jha P. Avoidable global cancer deaths and total deaths from smoking. Nat Rev Cancer 2009; 9: 655–64. Dikshit R, Gupta PC, Ramasundarahettige C, et al. Cancer mortality in India: a nationally representative survey. Lancet 2012; 379: 1807–16. Sankaranarayanan R, Swaminathan R. Verbal-autopsy-based projection of cancer deaths in India. Lancet 2012; 379: 1770–72. WHO. National cancer control programmes: policies and managerial guidelines (second edition). Geneva: World Health Organization, 2000. www.thelancet.com/neurology Published online June 1, 2012 DOI:10.1016/S1470-2045(12)70211-5