Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
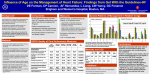
Online Appendix for the following JACC article TITLE: Changes in Myocardial Infarction Guideline Adherence as a Function of Patient Risk: An End to Paradoxical Care? AUTHORS: Apurva A. Motivala, MD, Christopher P. Cannon, MD, Vankeepuram S. Srinivas, MBBS, MS, David Dai, MSc, Adrian F. Hernandez, MD, MPH, Eric D. Peterson, MD, MPH, Deepak L. Bhatt, MD, MPH, Gregg C. Fonarow, MD ___________________________________________________________ APPENDIX Funding: The Get With The Guidelines Program (GWTG) is funded by the American Heart Association (AHA). The program is also supported in part by unrestricted educational grants to the AHA by Pfizer, Inc., New York, NY, and the Merck-Schering Plough Partnership (North Wales, PA), who did not participate in the design, analysis, manuscript preparation or approval. Disclosures: Apurva A. Motivala: none; Christopher P. Cannon: Research grants/support: Accumetrics, AstraZeneca, Bristol-Myers Squibb/Sanofi Partnership, GlaxoSmithKline, Intekrin Therapeutics, Merck, Novartis, Takeda ;Advisory Board (but funds donated to charity)-Bristol-Myers Squibb/Sanofi Partnership; Clinical Advisorequity in Automedics Medical Systems; Vankeepuram S. Srinivas: none; David S. Dai: none; Eric Peterson: Bristol Myers Squibb-Sanofi, Merck-Schering Plough; Adrian F. Hernandez: Merck, Johnson & Johnson, AstraZeneca; Deepak L. Bhatt: Research grants from Astra Zeneca, Bristol-Myers Squibb, Eisai, Sanofi Aventis, The Medicines Company; Gregg C. Fonarow: Bristol Myers Squibb-Sanofi, Merck-Schering Plough, Pfizer, AstraZeneca STUDY METHODS: Data Source: The GWTG-CAD program is a large, multicenter, observational registry started in 2000 to support and facilitate improvement of the quality of care for patients with cardiovascular disease. The GWTG Program uses a web-based patient management tool (PMT, Outcome Sciences Inc., Cambridge, MA) to collect clinical data and provide decision support with real-time online reporting features. The GWTG-CAD program enrolls patients hospitalized with a confirmed diagnosis of CAD (ICD-9 codes 410414 included). Trained data abstractors at participating hospitals in GWTG-CAD collected detailed information on baseline demographic and clinical characteristics, in-hospital care processes and outcomes, and discharge treatment using a standardized set of data elements and definitions. Using an internet-based system, data quality was monitored to assure the completeness and accuracy of the submitted data. Outcome Sciences, Inc. serves as the data collection and coordination center for GWTG. As collected data are used primarily used for institutional quality improvement and de-identified patient information was collected anonymously through retrospective chart review, individual informed consent was not required under the common rule. Participation in GWTG required approval of the institutional review board of each hospital. The Duke Clinical Research Institute serves as the data analysis center and has an agreement and Institutional Review Board approval to analyze the aggregate de-identified data for research purposes. Study patients: The study sample was drawn from 312,278 patients enrolled in the Get With The Guidelines-Coronary Artery (GWTG-CAD) database across 279 participating sites between January 2, 2000 and December 30, 2008 (after excluding sites with less than 30 admissions). Out of these, 119,948 patients with a discharge diagnosis of MI (with and without ST-segment elevations) were analyzed. Myocardial infarction was defined as presentation with symptoms of ischemia in association with positive cardiac enzymes. After excluding another 7100 patients who were transfer-outs, a total of 112,848 patients were analyzed (Figure 1). Of patients and hospitals included in the study past medical history data was complete in 82.1% of patients (83.1% for low risk group, 79.2% for intermediate risk group, and 83.9% for high risk group). We evaluated treatment rates among eligible patients only with contraindications to therapies determined and documented by their treating clinicians. Development/validation of a risk stratification model: After further excluding patients with missing gender or death information (3224 patients), a developmental sample consisting of 60% randomly selected MI patients from the study sample (109,624 patients) was used to create a risk score to divide the population into risk groups. After selecting a relevant list of risk factors (age, sex, race, body mass index, ST segment elevation MI, history of smoking, diabetes, hypertension, hyperlipidemia, renal insufficiency, hemodialysis, heart failure, stroke, peripheral vascular disease, prior myocardial infarction (MI), COPD, chronic depression, atrial fibrillation/flutter) based on prior models and clinical insight, we used univariate as well as multivariate, logistic regression analysis to identify factors independently associated with in-hospital mortality and a risk model was devised (Appendix 3). Model discrimination was assessed using C statistics. This risk stratification model was validated in the remaining 40% of MI patients in our cohort and had a discrimination C-statistic of 0.75. Statistical Analysis: Using this validated risk score, patients in our study sample were stratified into tertiles: low (0-3%), intermediate (3-6.5%), and high (>6.5%) inhospital mortality rates. Their baseline and presenting characteristics, in-hospital and discharge therapies were compared. Categorical variables are expressed as frequencies and percentages and were compared between groups using Pearson’s Chi-square test. Continuous variables are expressed as means and were compared between groups using KruskalWallis test. In examining the association between the risk and measure outcomes, a multivariable logistic regression was used to estimate the marginal effects of risk. The Generalized Estimating Equation (GEE) method with exchangeable working correlation structure was used to account for within-hospital clustering, because patients at the same hospital are more likely to have similar responses relative to patients in other hospitals (i.e. within-center correlation for response). The method produces estimates similar to those from ordinary logistic regression, but the estimated variances of the estimates are adjusted for the correlation of outcomes within each hospital. The GEE method was also used to examine the trend effect among each risk group. Furthermore, we evaluated if any trends observed were due to better documentation of contra-indications of therapies (as determined by the treating clinicians) over time. A p-value of <0.05 was considered statistically significant for all tests. All analyses were performed using SAS software version 9.1 (SAS Institute, Cary, NC). STUDY LIMITATIONS Although our sample consists of a large number of medical centers all over the US, participation in GWTG is purely voluntary and thus these findings may not be reflective of centers that are not included in the quality initiative. Data were collected by medical chart review and depend upon the accuracy and completeness of documentation. As such, a proportion of patients reported to be eligible for treatment who did not receive recommended therapies may have had contraindications or intolerance to specific interventions that were present but not documented. Also, the prevalence in the use of objective risk scores was not documented. Counseling regarding lifestyle interventions may have been provided but not recorded in the medical record. The improvements in performance and quality measures over time may have been influenced by factors other than GWTG-CAD participation such as secular trends. As GWTG does not collect data on post-discharge treatment or outcomes, the full implications of these improvements in process measure treatment rates for patients at low, intermediate and higher risk over time could not be directly explored. Table 1: Baseline and presenting characteristics LOW RISK INTERMEDIATE HIGH RISK RISK P-value (<3%) (3%-6.5%) (>6.5%) N=36,541 N=36,542 N=36,541 52±9 yrs 65±10 yrs 79±9 yrs <0.0001 Female gender 8747 (24%) 12476 (34%) 18894 (52%) <0.0001 Caucasians 27692 (76%) 28212 (77%) 28815 (79%) <0.0001 Blacks 3426 (9%) 2705 (7%) 2159 (6%) <0.0001 Hispanics 2188 (6%) 2176 (6%) 1869 (5%) n/a Asians 805 (2%) 995 (3%) 1424 (4%) n/a 28±3 27±3 26±4 <0.0001 21730 (60%) 11525 (32%) 3820 (11%) <0.0001 Diabetes Mellitus-insulin treated 1523 (5%) 2129 (7%) 2532 (8%) <0.0001 Diabetes Mellitus-non-insulin 3793 (13%) 3819 (13%) 3327 (11%) <0.0001 Hypertension 19200 (63%) 18843 (65%) 21119 (69%) <0.0001 Hyperlipidemia 18917 (62%) 13830 (48%) 9361 (31%) <0.0001 Chronic renal insufficiency 333 (1%) 1272 (4%) 5511 (18%) <0.0001 ESRD on hemodialysis 37 (0.1%) 268 (1%) 1274 (4%) <0.0001 Age (mean±SD) BMI (mean±SD) Smoking Prior MI 5241 (17%) 5200 (18%) 6687 (22%) <0.0001 CVA/TIA 544 (2%) 1670 (6%) 5282 (17%) <0.0001 Peripheral Vascular Disease 835 (3%) 2030 (7%) 4309 (14%) <0.0001 COPD/Asthma 1891 (6%) 3590 (12%) 6517 (21%) <0.0001 Heart Failure 846 (3%) 2419 (8%) 8232 (27%) <0.0001 Anemia 358 (1%) 776 (3%) 1909 (6%) <0.0001 Prior PCI 834 (3%) 705 (2%) 490 (2%) <0.0001 Prior Bypass Surgery (CABG) 402 (1%) 571 (2%) 544 (2%) <0.0001 STEMI 7315 (20%) 8990 (25%) 8116 (22%) n/a NSTEMI 20335 (56%) 16358 (45%) 14966 (41%) n/a HR (mean±SD;bpm) 80±19 82±22 86±23 <0.0001 SBP (mean±SD;mmHg) 138±28 137±29 135±31 <0.0001 LDL (mean±SD;mg/dL) 113±42 103±39 94±35 <0.0001 HDL (mean±SD;mg/dL) 36±11 39±12 41±14 <0.0001 183±147 147±108 120±82 <0.0001 HbA1C 8±2 8±2 7±1.5 <0.0001 Ejection Fraction (mean) 50% 47% 44% <0.0001 TG (mean±SD;mg/dL) All results in expressed as total (percentage) unless stated otherwise SD: Standard Deviation Table 2: Management and Outcomes LOW RISK INTERMEDIATE HIGH RISK RISK P-value (>6.5%) (<3%) (3%-6.5%) N=36,541 N=36,542 Per-cutaneous intervention (in-hospital) 22983 (71%) 19988 (64%) 13926 (47%) <0.0001 Coronary Artery Bypass Graft (in-hospital) 3385 (10%) 3582 (11%) 2431 (8%) <0.0001 3 4 5 <0.0001 34734 (95%) 31746 (87%) 23339 (64%) <0.0001 Discharged to skilled nursing 686 (2%) 2344 (6%) 7064 (19%) <0.0001 Death 500 (1%) 1473 (4%) 4132 (11%) <0.0001 Length of stay (median days) Discharged home All results in expressed as total (percentage) unless stated otherwise SD: Standard Deviation N=36,541 Table 3: Performance Measures (among eligible patients only) LOW RISK INTERMEDIATE HIGH RISK RISK (<3%) (3%-6.5%) P-value (>6.5%) MI/angina patients receiving aspirin within 24 hrs of presentation Patients discharged on aspirin Patients with LDL>100 who receive lipid lowering agents Patients discharged on β-blockers N=36,541 N=36,542 N=36,541 21852/22440 21996/22800 22830/24277 (98%) (97%) (94%) 33424/34193 31584/32444 26849/28094 (98%) (97%) (96%) 11797/12432 8921/9602 (93%) 5256/6153 (95%) 30823/31839 26705/28117 (97%) (97%) (95%) Patients with documented LV systolic 4752/5202 5840/6546 (89%) 6303/7656 dysfunction discharged on ACEi/ARBs (91%) Current smokers who receive smoking 20253/21099 10139/10929 2858/3322 (96%) (93%) (86%) 32537/36019 31450/35453 28458/33958 (90%) (89%) (84%) Composite Performance measure for 100% compliance <0.0001 <0.0001 (85%) 32198/33166 cessation advice <0.0001 <0.0001 <0.0001 (82%) <0.0001 <0.0001 All results in expressed as total (percentage) unless stated otherwise LDL: Low density lipoprotein, LV: Left ventricle, ACEi: Angiotensin Converting Enzyme inhibitors ARBs: Angiotensin Receptor Blockers Table 4: Quality Measures (among eligible patients only) LOW RISK INTERMEDIATE HIGH RISK RISK P-value (<3%) (3%-6.5%) (>6.5%) N=36,541 N=36,542 N=36,541 MI pts who receive 18796/20280 18198/20268 18174/20977 -blockers≤24 hrs (93%) (90%) (87%) 85/138 mins 84/140 mins 92/156 mins <0.0001 37/54 mins 39/55 mins 44/60 mins 0.004 Door-PCI time for STEMI/LBBB <0.0001 (N=17,787) (median/mean) Door-tPA time for STEMI/LBBB (N=2143) (median/mean) Patients with a recorded LDL Patients with last recorded BP <140/90 mm Hg Patients who receive statins or lipid lowering agents Patients discharged on ACEi/ARBs Patients that received cardiac rehabilitation referral or physical activity recommendations Overweight patients that receive wt. management and physical activity recommendations Diabetic treatment amongst DM patients Diabetic teaching amongst DM patients 26694/35594 25095/34657 20149/31439 (75%) (72%) (64%) 23593/27667 21321/25896 18917/24222 (85%) (82%) (78%) 32323/34842 30354/33760 24022/30247 (93%) (90%) (79%) 25735/33258 24694/31715 20396/27677 (77%) (78%) (74%) 28441/35594 26136/34657 22574/31439 (80%) (75%) (72%) 21022/24033 16978/20008 11217/13891 (88%) (85%) (81%) 4697/5191 4844/5561 4147/5034 (91%) (87%) (82%) 495/5191 528/5561 367/5034 (10%) (10%) (7%) All results in expressed as total (percentage) unless stated otherwise <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 LBBB: Left bundle branch block, LDL: Low density lipoprotein, ACEi: Angiotensin Converting Enzyme inhibitors ARBs: Angiotensin Receptor Blockers Table 5: Temporal trends for improvement among each category Unadjusted Adjusted Outcome Category O.R. Lower CI Upper CI AMI patients without contraindications that receive ASA<24 hrs (High Risk per Year Increase) 1.14 1.07 1.21 p Value <.0001 O.R. 1.22 Lower CI 1.11 Upper CI 1.33 P Value <.0001 Unadjusted Outcome Defect-free measure Current smokers that receive smoking cessation advice Patients discharged on Beta Blockers Patients discharged on aspirin Patients with LDL>100 who receive lipid lowering drugs Patients with documented LVSD discharged on ACE Inhibitors or ARB Opportunity Composite Measure Adjusted Category O.R. Lower CI Upper CI p Value O.R. Lower CI Upper CI P Value (Intermediate Risk per Year Increase) 1.13 1.05 1.22 0.0009 1.21 1.11 1.31 <.0001 (Low Risk per Year Increase) 1.20 1.07 1.35 0.002 1.30 1.14 1.47 <.0001 (High Risk per Year Increase) 1.28 1.22 1.34 <.0001 1.32 1.25 1.40 <.0001 (Intermediate Risk per Year Increase) 1.29 1.21 1.37 <.0001 1.33 1.25 1.42 <.0001 (Low Risk per Year Increase) 1.31 1.21 1.42 <.0001 1.37 1.26 1.49 <.0001 (High Risk per Year Increase) 1.54 1.40 1.69 <.0001 1.62 1.45 1.81 <.0001 (Intermediate Risk per Year Increase) 1.61 1.44 1.82 <.0001 1.70 1.49 1.94 <.0001 (Low Risk per Year Increase) 1.64 1.44 1.87 <.0001 1.76 1.53 2.03 <.0001 (High Risk per Year Increase) 1.17 1.08 1.27 0.0003 1.33 1.19 1.48 <.0001 (Intermediate Risk per Year Increase) 1.14 1.03 1.26 0.01 1.30 1.15 1.47 <.0001 (Low Risk per Year Increase) 1.07 0.93 1.22 0.36 1.23 1.04 1.45 0.018 (High Risk per Year Increase) 1.10 1.00 1.22 0.05 1.34 1.21 1.48 <.0001 (Intermediate Risk per Year Increase) 1.06 0.92 1.21 0.43 1.28 1.10 1.49 0.0012 (Low Risk per Year Increase) 1.02 0.84 1.25 0.82 1.26 1.00 1.59 0.05 (High Risk per Year Increase) 1.12 1.07 1.16 <.0001 1.22 1.15 1.30 <.0001 (Intermediate Risk per Year Increase) 1.08 1.04 1.13 0.0003 1.18 1.12 1.25 <.0001 (Low Risk per Year Increase) 1.09 1.05 1.14 <.0001 1.25 1.18 1.33 <.0001 (High Risk per Year Increase) 1.35 1.28 1.41 <.0001 1.29 1.21 1.37 <.0001 (Intermediate Risk per Year Increase) 1.33 1.26 1.41 <.0001 1.28 1.19 1.37 <.0001 (Low Risk per Year Increase) 1.33 1.25 1.43 <.0001 1.28 1.18 1.39 <.0001 (High Risk per Year Increase) 1.24 1.18 1.30 <.0001 1.30 1.23 1.37 <.0001 (Intermediate Risk per Year Increase) 1.24 1.16 1.32 <.0001 1.30 1.21 1.39 <.0001 Unadjusted Outcome Adjusted Category O.R. Lower CI Upper CI (Low Risk per Year Increase) 1.25 1.15 1.37 p Value <.0001 O.R. 1.33 Lower CI 1.22 Upper CI 1.45 P Value <.0001 In examining the association between the risk groups and the outcomes, a multivariable logistic regression was used to estimate the marginal effects of the risk groups. The Generalized Estimating Equation (GEE) method with exchangeable working correlation structure was used to account for within-hospital clustering, because patients at the same hospital are more likely to have similar responses relative to patients in other hospitals (i.e. within-center correlation for response). The method produces estimates similar to those from ordinary logistic regression, but the estimated variances of the estimates are adjusted for the correlation of outcomes within each hospital. As the patient characteristics such as age, gender, race, BMI, and medical histories have been used to classify the different risk groups, we do not include them as the adjusted variables here. The adjusted variables are the hospital characteristics (bed size, region, heart transplants, academic, interventional, residents, CT surgery on site, primary PTCA performed for AMI). Opportunity Composite Measure: Calculated as the total number of successes across all patients, divided by the number of opportunities for all performance measures for which they are eligible. Table 6: Temporal trends in documentation of contra-indications to therapies Low risk group: Admit year ACEi/ARB Aspirin Beta blocker Lipid Lowering agents 2002 0% 2.04% 3.88% 0% 2003 0% 2.24% 5.34% 0.41% 2004 0.26% 1.93% 6.09% 0.37% 2005 2.47% 3.3% 5.16% 1.22% 2006 7.85% 4.19% 6.42% 2.16% 2007 9.77% 4.25% 7.03% 2.2% 2008 10.89% 4.61% 8.27% 2.72% Intermediate risk group: Admit year ACEi/ARB Aspirin Beta blocker Lipid Lowering agents 2002 0% 2.08% 3.99% 0.98% 2003 0% 3.39% 6.44% 0.58% 2004 0% 3.06% 7.57% 0.60% 2005 5.71% 3.81% 6.28% 1.06% 2006 11.22% 6.88% 7.83% 2.78% 2007 14.80% 7.41% 8.81% 3.69% 2008 19.06% 8.59% 8.85% 4.38% High risk group: Admit year ACEi/ARB Aspirin Beta blocker Lipid Lowering agents 2002 0% 5.12% 7.48% 1.07% 2003 0% 7.39% 10.03% 0.68% 2004 0.81% 8.22% 10.07% 1.79% 2005 8.4% 7.45% 9.97% 1.56% 2006 16.75% 11.52% 9.92% 4.02% 2007 23.52% 12.35% 11.05% 6.25% 2008 27.63% 13.33% 12.10% 7.16%