Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
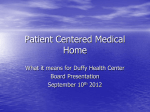
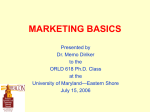
State Innovation Models (SIM) Award: Community Integrated Medical Home A Framework for Health Care Reform Raquel E. Samson, MPH Deputy Director Health Systems and Infrastructure Maryland Department of Health & Mental Hygiene DHMH Health System and Infrastructure Administration Organizational Structure DHMH Public Health Health System and Infrastructures Administration Primary Care Access and Workforce Population Health and Quality School Health Local Health Department Core Funding 3 The Affordable Care Act: Better Health, Better Care, Lower Costs Better Health Prevention Fund and National Strategy Better Care Delivery System Reforms Community Transformation Grants Value-Based Purchasing Tobacco Shared Savings Partnership for Patients Lower Costs Rate Review Medical Loss Ratio Delivery System Reforms Obesity Lydia L. Ogden, PhD, MPP, CDC Director, Office of Health Reform - September 13, 2011 The Logic of Health Reform Improved Health Outcomes Expanded Insurance Coverage • Conditions are amenable to care • Social determinants of health addressed High Value Care • Medicaid & CHIP • Exchanges • High Quality • Delivered Efficiently Expanded Access to Care • Emphasis on primary care • Assumes supply sufficient to meet demand Effective Care • In and out of clinical environment • Patient selfefficacy, health literacy, adherence Reduced Health Spending • Population health and spending are the sum of individual health and spending Lydia L. Ogden, PhD, MPP, CDC Director, Office of Health Reform - September 13, 2011 Social Determinants of Health Integration of public health and the medical delivery system is required if our goal is to improve health of the individual and population. Delivering Care in the Appropriate Setting Higher Cost Lower Cost State Innovation Models (SIM) Grant Solicitation • Released by Center for Medicare & Medicaid Innovation (CMMI) at CMS to develop, implement, and test new health care payment and service delivery models at the state-level • Maryland received “Model Design” award – $2.37 million – 6-month planning grant (April 1 – August 31, 2013) – Opportunity to apply for “Model Testing” award for up to $60 million to fund implementation over a 4 year period. • “State Innovation Plan” that articulates the Community Integrated Medical Home (CIMH) model in detail and basis for Model Testing application to CMMI Community-Integrated Medical Home (CIMH) • Integration of a multi-payer medical home model with community health resources is to improve health care quality, experience and to lower cost. • 4 pillars: 1) 2) 3) 4) Primary care Community health Strategic use of new data Workforce development • CIMH is a framework with certain programmatic standards that allows for innovations across payers Community-Integrated Medical Home Local Health Improvement Coalition (LHIC) Engagement Process • Complement medical care by linking high-need patients with wrap-around community-based health services • Capacity of LHICs will be strengthened • Recommend Community Health Worker role • Use new data and mapping resources to “hot-spot” high utilizers and bring them into CIMH New Data Resources • Chesapeake Regional Information System for our Patients (CRISP) State Wide Health Information Exchange developing mapping tools for “hot-spotting” • DHMH will expand Virtual Data Unit • Maryland Health Care Commission to assess and plan expansion of All-Payer Claims Database (APCD) Sample Hot-Spotting Map CRISP Workforce Development and CIMH Readiness • Community Health Worker development – Inventory of training programs and CHW models – Identify best practices for integration of CHW into medical practices and broader health care system – Will present findings at LHIC stakeholder engagement process • Technical assistance and CIMH readiness – – – – Identify various ongoing TA and develop recommendation for streamlining Convene TA providers and chart path forward Identify and describe quality improvement efforts in local communities Assist in scaling up of promising QI models Population Health Improvement at All Levels of Health Need A Secondary Prevention and Effective Care Coordination – Aim for 80% PCP participation in medical home (currently at 50%)--including a new state-certified PCMH--to cover 80% of Marylanders. Enhanced community-based preventive interventions in collaboration with PCMH super utilizers chronically ill & at risk of becoming super utilizer B “Hot Spotting” – Deploying effective complementary community-based supports that “wrap around” the primary care medical home; patient assessment determines range of services offered C chronically ill but under control healthy 6 Million Marylanders Promoting and Maintaining Health through the Built Environment, Structured Choice & Effective Primary Prevention – Aim for 80% uptake of USPSTF grade A/B preventive services. Make the healthy choice the easy choice by creating defaults through effective town planning and other behavioral economic 14 approaches. B “Hot Spots” Designing Community Intervention Models for Maryland overlap – “super-utilizers” (needs further operational definition) – chronically ill at higher-risk super utilizers • Assess, understand, and care for the whole person, addressing all types of risk to health – Customize intervention plan based on assessment and participant needs, preferences, and values – Mindset is longitudinal not episodic chronically ill at risk of becoming super utilizer Greatest ROI Potential • Best return on investment (ROI) opportunities appears to be among chronically ill and under control healthy DRAFT Roles/Responsibilities for Care Managers & Community Health Professionals Community Health Team PCMH with office-based care manager(s) Community Team Leader + CHWs CM PCMH Community-Clinical Integration PCMH without office-based care manager(s) Community Team Leader + CHWs PCMH CM 16 Eight-Component Model of Coordinated School Health Comprehensive School Health Education Family & Community Involvement Mental health issues Asthma Physical Education Diabetes Violence/bullying School-site Health Promotion for Staff School Health Services Teen pregnancy Academic achievement Healthy School Environment Nutrition Services Counseling, Psychological & Social Services Source: ASTHO: Making the Connection www.thesociety.org Wellness policies HIV prevention ETC! Community-Integrated Medical Home Example: Pediatric Asthma HOSPTIAL UTILIZATION DATA (CRISP) Community Health Team • Environmental assessment • Individualized asthma education • Evidence based intervention • Support/Implement care plan • Support social service referrals • Accompany to appointments SBHC and/or School Nurse • • • • • Prevention/Asthma education Ongoing nursing assessments Develop/Implement care plan Treatment Academic follow-up PCP • • • • Assessment/Diagnose Treatment/Medications Care Plan Care coordination Specialist • Diagnose/Treatment • Care Plan/follow-up • Prescribe medication Community-Integrated Medical Home School Health Contacts Karen Matsuoka, PhD Director, Health Systems and Infrastructure Administration [email protected] Raquel Samson, MPH Deputy Director, Health Systems and Infrastructure Administration Director, Office of Primary Care Access [email protected] Angela Wakhweya, MD, MSc Director, Office of School Health [email protected] Cheryl De Pinto, MD, MPH Medical Director, Office of School Health [email protected]