Survey
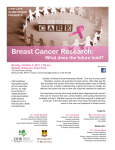
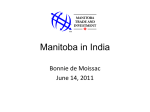
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
PROFESSOR SABINE MAI Nuclear remodelling of telomeres Professor Sabine Mai discusses a collaborative project that seeks to understand the mechanisms at play in the hitherto uncharted 3D nuclear space during normal to cancerous cellular transformation is known to occur during tumour development, however it is never studied as a function of cellular transformation in 3D nuclei of primary cells from the same lineage. 3D telomere profiling (3D-TP) is a powerful platform technology that provides a unique measure of genomic instability applicable across a wide range of malignancies. At what stage is 3D-TP in its development, and how does it measure genomic instability? To begin, could you describe how you came to study the mechanisms and consequences of three-dimensional (3D) nuclear remodelling of telomeres in cancer? Our work has focused on genomic instability and on mechanisms that initiate and/or drive that instability. We soon realised that there are very early changes in nuclear structure that were associated with the development of a cancerous phenotype and that we therefore needed to focus on the interphase nucleus and the remodelling of its nuclear architecture. When reviewing the literature, it became apparent that there was not a unified way of looking at nuclear changes in cancer and that multiple cell lines and endpoints had been used. We decided to dedicate our efforts to primary, immortalised and tumour cells (not cell lines) of the same lineage to truly understand what was happening in the 3D nuclear space during cellular transformation from normal to cancerous. To define what is a ‘normal’ nuclear architecture we chose to study telomeres which are the ends of chromosomes. The rationale behind this was that telomeres can be used to ‘mark’ chromosome positions in the interphase nucleus. Telomere dysfunction We have just started to explore the scope of the potential of the 3D teleomere analysis in cancer diagnosis, prognosis and monitoring. Our group and many collaborating partners within Canada and abroad have applied this 3D telomere profiling technology in numerous different tumour settings: from Hodgkin’s lymphoma to prostrate and thyroid cancer and acute myeloid leukaemia. Ongoing studies focus on breast cancer, oesophageal cancer and cholangiocarcinoma. We are anticipating that 3D telomere analysis will be a platform technology applicable across many malignant and premalignant processes. TeloView, a computer program for 3D telomere analysis, has been automated in collaboration with Applied Spectral Imaging and we are currently performing 3D telomere scanning of 15,000 cells per hour. We are now planning the clinical trials needed for validation of 3D-TP as a clinical biomarker. How might measurements of genomic instability applicable across a wide range of malignancies, sample types, and clinical scenarios predict biologic activity of a given malignancy and guide cancer management in a patient-specific manner? 3D-TP will define the level of genomic instability that is characteristic for malignancy and changes as the disease progresses. Once trials are complete, we hope to be able to use 3D-TP to better define the risk of progression and likelihood of response to therapy in patients at diagnosis and develop treatments appropriate to the biology of the malignancy. Could you describe the process involved in obtaining 3D-TP stratified patient samples? One of the major strengths of this technology is that the 3D-TP testing can be performed on a variety of sample types including tumour biopsies, blood and buccal smears. Formalynembedded and fresh frozen samples can also be used. After removal of paraffin or fixation of cells, the telomeres are labelled with a florescent probe. The microscope is equipped with an automated image capture system (Telo Scan) which is able to image over 15,000 individual nuclei per minute. Analysis of the data generated then produces a 3D image of the individual cells and cell populations within the nucleus. What are the challenges associated with integrating genomic technologies into clinical practice? Taking a laboratory observation and integrating it into clinical practice is a complex process that includes many cycles of bench to bedside and back to bench. Our initial observations must be confirmed in independent patient cohorts and then demonstrated to guide treatment in a way that is independent of current established prognostic testing. This process involves collaboration between clinicians, scientists, healthcare analysts and policy makers. Have you forged international partnerships to implement 3D-TP? How important is collaboration to your work? Collaborations are key. Without the multidisciplinary skills the different members of our team bring to the table, this work could not have been as successful as it is. Importantly, now at the verge of clinical diagnostic trials, the expertise of all clinical collaborators is advancing the work, its depth and speed. WWW.RESEARCHMEDIA.EU 117 PROFESSOR SABINE MAI Novel 3D cancer genomics A team at the Manitoba Institute of Cell Biology, University of Manitoba, is investigating how novel 3D telomere profiling can radically change cancer screening, diagnosis and prediction of prognosis RECENT TECHNOLOGICAL ADVANCES are having a significant impact on many areas of cancer research. Cancerous cells are marked by genomic instability and one of the most powerful platforms for current hitech development lies in this area. A research group at the Manitoba Institute of Cell Biology, headed by Dr Sabine Mai, is using 3D quantitative fluorescent in situ hybridisation (FISH) and next-generation sequencing (NGS) in the hope of optimising this technology for practical clinical use in cancer treatment. be separated according to increasing degrees of genomic instability, which has correlated with the progression of malignancy”. Moreover, integrating the 3D-TP measures of instability with NGS will enable the researchers to analyse the genomic changes associated with progression in instability. By identifying and categorising patients into levels of genomic instability before performing NGS, the team will increase the chances of identifying driver mutations. Telomeres are repeating DNA sequences at the ends of chromosomes that are involved in the replication and stability of DNA molecules. On the realisation that the 3D telomere organisation of normal cells differed from that of tumour cells, Mai and her team set about developing tools that would be able to quantify these differences. In collaboration with Dr Yuval Garini, a Professor of Physics and Nanotechnology at Bar Ilan University in Israel, they created TeloView, a computer program that measures the parameters that define variations between normal and tumour cells. As part of their research programme, the scientists are seeking to address the unique diagnostic challenges associated with prostate cancer, plasma cell dyscrasias and Hodgkin’s lymphoma. Crucially, by using 3D-TP, this will be the first time researchers have tackled these difficulties in relation to these three types of cancers. “These measurements include telomere numbers, telomere sizes, telomere positions during the cell cycle, telomere distances from the nuclear periphery and from the nuclear centre,” Mai explains, the combined results of which provide a quantitative tool for determining whether a cell is normal or cancerous. The benefits of this instrument are many, one of which is the early detection of cancer, as she asserts: “If specific profiles are detected that correlate with early onset, moderate or severe disease, treatment regimens can be attempted early on to slow down or prevent the development of full blown disease”. 3D TP ANALYSIS Telomere dysfunction is known to occur during tumour development, and can result in enormously elevated rates of chromosomal alterations. To determine the position of chromosomes, the group tag the telomeres in nuclei and then image them in 3D using a process similar to that of CT scans, but at 200 nm steps through each nucleus. 3D images of the nuclei are subsequently rendered to display the results observed in the nucleus, and this is known as 3D telomere profiling (3D-TP). 3D-TP analysis is highly advantageous because, as Mai further elucidates: “Clinical material can 118 INTERNATIONAL INNOVATION ADDRESSING DIAGNOSTIC CHALLENGES Prostate cancer poses a diagnostic challenge because not all patients with this disease need treatment. Indeed, men with non-aggressive prostate cancer can live for years with no negative impact on quality of life. Careful monitoring of prostate cancer may be all that is required, rather than surgery and treatment with drugs, which can lead to unwanted and severe side-effects. Thus, there is a need for a novel diagnostic process that can determine whether a patient would benefit from watchful waiting or prostatectomy and radiation therapy, both of which can cause impotence and/or incontinence. In collaboration with clinicians Drs Drachenberg and Saranchuk (CancerCare Manitoba), the team is evaluating the effectiveness of 3D-TP for this type of diagnostic decision-making. Mai asserts: “We postulate that the tumours with the greatest genomic instability as measured by 3D-TP will have the most aggressive disease and the group of patients demonstrating this should receive treatment earlier”. Indeed, categorising patients in this way would mean that diagnoses are far more accurate and could potentially lead to a personalised approach to the treatment of the disease. PLASMA CELL DYSCRASIAS AND HODGKIN’S LYMPHOMA In cases of plasma cell dyscrasias there is currently no way to predict the risk of a patient progressing from monoclonal gammopathy of undetermined significance (MGUS) or smouldering myeloma (SMM) to multiple myeloma (MM). Working with clinical collaborator Dr Ade Olujohunbghe (CancerCare Manitoba), the researchers are able to define specific profiles for each patient group, allowing them to detect and develop transition FIGURE 1. Classical Hodgkin’s lymphoma of mixed cellularity type, LMP1 positive. Bi-nuclear Reed-Sternberg cell surrounded by a corona of lymphocytes. Nuclear DNA of lymphocytes (DAPI, blue) contains multiple small to mid-sized telomeres (red), whereas the central nuclei of the Reed-Sternberg cell are free of telomeres and also show DNA free holes; this cell is a real, end-stage cancer cell, a ‘ghost-cell’unable to undergo further mitoses. Image provided by Dr Hans Knecht. INTELLIGENCE MECHANISMS AND CONSEQUENCES OF THREE-DIMENSIONAL (3D) NUCLEAR REMODELLING OF TELOMERES IN CANCER OBJECTIVES To research the primary, immortalised and tumour cells (not cell lines) of the same lineage to truly understand the mechanisms at play in the 3D nuclear space during cellular transformation from normal to cancerous. KEY COLLABORATORS These include: Dr Yuval Garini • Dr Yvon Cayre • Dr Francis Wiener • Dr George Klein • Dr Marie Henriksson • Dr Nir Katzir • Dr Konrad Huppi • Dr Marc Tischkovitz • Dr Fabio Morato de Oliveira • Dr Anu Tamm Dr Marie Punab • Dr Vera Cappelletti From Canada: FIGURE 2. Nuclear staining with DAPI (blue) highlights chromatin organisation in the Reed-Sternberg cell of Hodgkin’s lymphoma, imaged with super resolution microscopy. Image provided by Christiaan Righolt, PhD student in Dr Mai’s lab. profiles that are presently undeterminable by any other method. Similarly, although the majority of Hodgkin’s lymphoma is treatable, 20 per cent of patients with this cancer do not respond to treatment and will die of their disease. Mai explains: “One of the challenges with Hodgkin’s lymphoma is that the malignant cell population is a minor component of the tumour mass and there has not been a method to study the nuclear stability in the clinic”. Working with clinical collaborator Dr Hans Knecht from the University of Sherbrooke and Dr Donna Wall from CancerCare Manitoba, she states that: “3D-TP can define different profiles for the malignant Hodgkin’s and Reed-Sternberg cells within the lymphoma which are predictive of clinical behaviour”. This approach allows the group to develop a personal profile for each patient using the trial information. Those profiles will then be categorised according to the stage of Hodgkin’s lymphoma, in other words how stable, aggressive and curable it is, and this will have a considerable impact on the way patients are treated after diagnosis. FROM BENCH TO CLINIC The ultimate aim of the project is to guide personalised patient management in cancer. After the first year of validating previous 3D-TP observations, the second phase of the project will focus on demonstrating the potential impact of 3D-TP on personalised management in the medical world. Integrating such new genomic technologies into clinical practice can be challenging. However, the strength of this investigation lies in the involvement of many frontline practitioners, and the valued evaluation of potential end-users in the clinical trial period. They hope to identify issues that may affect the clinicians’ acceptance of the tests and are also aiming to study the likely impact of 3D-TP on patients and their families in order to provide qualitative research input on the important aspects of the ‘cancer journey’. The ultimate aim of the project is to guide personalised patient management in cancer University of Sherbrooke: Dr Hans Knecht, Dr Regen Drouin • McGill University: Dr William Foulkes • CancerCare Manitoba: Dr Donna Wall, Dr Don Houston, Dr Rajat Kumar, Dr Ade Olujohunbghe • Prostate Center, CancerCare Manitoba: Dr Jeff Saranchuk, Dr Darrel Drachenberg • University of Manitoba: Dr Kathleen Gough, Dr Jim Davie, Dr Michael Mowat, Dr Sabine Hombach-Klonisch, Dr Thomas Klonisch, Dr Catalena Birek • The Hospital of Sick Kids: Dr Uri Tabori, Dr Cynthia Hawkins • The British Columbia Cancer Agency: Dr Kim Chi • Zeiss Canada: Dr Oliver Prange FUNDING Canadian Institutes of Health Research CONTACT Mai is confident that the clinical team will push the project to its final goal. Furthermore, the researchers have the full support of Diagnostic Services of Manitoba, a not-for-profit corporation responsible for all of Manitoba’s public laboratory services and for rural diagnostic imaging services, and the Winnipeg Regional Health Authorities. The key now is to keep the momentum going: “We have to keep this positive interaction going at each stage of the project to ensure its full uptake,” she affirms. Professor Sabine Mai, PhD Senior Investigator, Manitoba Institute of Cell Biology Professor, University of Manitoba Director, The Genomic Centre for Cancer Research and Diagnosis If the integration challenges are overcome, the advancements of this technology could radically change cancer screening, diagnosis and prediction of prognosis, leading to optimal management and monitoring. And it is the potential for progress from ‘bench to clinic’ that excites Mai the most. She envisions 3D-TP having a considerable impact on the delivery of healthcare: “If we succeed, we can change the way patients are diagnosed and treated”. The team expects to have licensure in Canada, US and EU with commercialisation, through licensure and development of a diagnostic testing company. Notably, they aim to have 3D-TP in clinics in the next five years. T +1 204 787 2135 E [email protected] Manitoba Institute of Cell Biology CancerCare Manitoba 675 McDermot Avenue, Room ON6026 Winnipeg, Manitoba Canada, R3E 0V9 www.umanitoba.ca/institutes/manitoba_ institute_cell_biology SABINE MAI is Professor of Physiology, Biochemistry and Medical Genetics, Human Anatomy and Cell Science at the University of Manitoba. She completed her PhD in Molecular Biology at the University of Karlsruhe. She has received grants from CIHR, CIHR RPP, Myeloma Canada, CancerCare Manitoba, Terry Fox Research Institute, Leukemia and Lymphoma Society of Canada, and CFI LEF among other funding awards. WWW.RESEARCHMEDIA.EU 119