Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
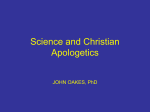
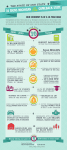
The Health of Women and Girls Factsheet Series Preconception Health in Michigan Michigan: Physical Activity Nutrition and Nutrition Physical and Activity Women’s Health: Summary Figure 1: Prevalence of women aged 18-44 years with self-reported positive indicators, or Summary of Key Points (2010 MI-PRAMS and 2011 those which would ideally increase over time with MI-BRFSS data presented in these factsheets) improved health; 2011 MIBRFSS and 2010 MI PRAMS. Most women aged 18-44 years did not have adequate fruit and vegetable Adequate Fruit and Vegetable Consumption * consumption, prenatal multivitamin use, 22.1 or physical activity Prenatal Multivitamin Use ^ 29.2 While prenatal multivitamin use was achieving and exceeding the HP 2020 Adequate Physical Activity * 18.7 Goal, several significant disparities were evident based on age, race, health 0 10 20 30 Percent 40 50 insurance status, educational attainment, and household income Figure 2: Prevalence of women aged 18-44 years with self-reported negative indicators, or The total prevalence of adequate physical those which would ideally decrease over time activity did not achieve the HP 2020 Goal, with improved health; 2011 MI BRFSS and 2010 and significant disparities were evident MI PRAMS. based on race, health insurance status, educational attainment, and household Overweight or obese * 26.9 income 28.7 Overweight Prenatal overweight or obese ^ 23.8 overweight (23.8%) or obese (21.3%) at the 21.3 Obese 0 10 20 30 40 Percent Over 46% of Michigan women were 50 60 time they became pregnant The prevalence of prenatal obesity was higher among black women compared to * MI-BRFSS: women aged 18-44 years ^ MI-PRAMS: women aged 18-44 years having a live birth white women The Health of Women and Girls Factsheet Series Preconception Health in Michigan Michigan: Physical Activity Nutrition and Nutrition Physical and Activity Overview of Preconception Health Why is Preconception Health Important? Preconception health refers to the health and well-being of women prior to becoming pregnant either for the first time or with subsequent pregnancies. Improving the preconception health of women can improve maternal and infant health outcomes.1,2,3 Preconception health encompasses biomedical, Fruit and Vegetable Consumption Folic Acid Supplementation Overweight and Obesity Exercise and Physical Activity For information regarding data sources, please reference the “Preconception Health in Michigan: Nutrition and Physical Activity” factsheet subtitled “Data Sources.” Healthy People 2020 Goals behavioral, and social factors. In 2010, nearly The Healthy People 2020 (HP 45% of Michigan mothers delivering live births 2020) Goals are a set of science- reported that the pregnancy was unintended based goals created by a national multi- (PRAMS data). Additionally, many women do disciplinary group with the objective of improving not seek prenatal care until eight weeks of gesta- the health and well-being of all people in the tion or later, at which time the period that carries United States.3 In the factsheets, the HP 2020 the highest risk for the fetus has already Goal is represented by a dashed line and an passed.3 Education and awareness of improved arrow demonstrating whether it is more desirable health of all women of reproductive age can help to be above or below the goal. improve future pregnancy outcomes. References Preconception Health Indicators 1. Centers for Disease Control and Prevention. Recommendations to improve preconception health and health care—United States. MMWR 2006; 55 (RR06):1-23 2. Broussard DL, et al. Core state preconception health indicators: a voluntary, multi-state selection process. Matern. Child Health J. 2011; 15(2):158168. 3. United States Department of Health and Human Services. “Healthy People 2020.” 2013. Available online: http://www.healthypeople.gov/2020/ default.aspx. Accessed May 10, 2013. A national committee of state program leaders and epidemiologists has identified broad health domains related to preconception health, and has proposed specific health indicators based on currently measurable data for women of reproductive age.2 Indicators are used to monitor public health status and help Suggested Citation assess progress toward national and state goals. Vanos H, Larder C, Fussman C, McKane P, Wahl R. Michigan Department of Community Health. “Preconception Health in Michigan: Nutrition and Physical Activity.” 2013. The information in these factsheets encompasses the Nutrition and Physical Activity Domain: The Health of Women and Girls Factsheet Series Preconception Health in Michigan Preconception Health in Michigan Nutrition Nutrition and and Physical Physical Activity Activity Fruit and Vegetable Consumption Overview: Low birth weight and prematurity are dent, none achieved associated with maternal dietary inadequacy statistical significance before becoming pregnant. The diets of mothers with low birth weight infants are frequently deficient in fruits and vegetables.1 Fruits and vegetables are important sources of vitamins, including folic acid and Vitamin A, which are essential for healthy fetal development. Growth of the placenta and fetus is most susceptible to Trends Over Time: Prevalence has slightly increased over the years of 2002-2009 Figure 1: Prevalence of women aged 18-44 years with self-reported adequate fruit and vegetable consumptiona by year, 2002-2011 Michigan BRFSS. 40 the effects of maternal nutrition during the pre-implantation period through the first few 30 Percent weeks of gestation.2 Typically, this occurs before pregnancies are confirmed. Women of reproductive age, especially those planning to become pregnant, can maximize future pregnancy health 20 10 by eating a well balanced diet including fruits, 0 2000 vegetables, and foods containing calcium, 2002 2004 2006 2008 2010 2012 2 protein, iron, Vitamin C, and folic acid. Preconception Health Indicator: Percentage of women aged 18-44 years who consume fruits (including juice) and vegetables at least 5 times Due to BRFSS methodology changes, 2011 BRFSS estimates cannot be compared to BRFSS estimates from previous years. a Consumption of fruits (including juice) and vegetables at least 5 times per day per day References HP 2020 Goal: Increase the contribution of fruits 1. Brundage SC. Preconception health care. Am. Fam. Physician 2002; 65(12):2507-2515 2. Gardiner PM, Nelson L, et al. The clinical content of preconception care: nutrition and dietary supplements. Am. J. Obstet. Gynecol. 2008; 199(6 suppl 2):s345-56 and vegetables to the diets of the population aged 2 years and older Key Points (MI-BRFSS, 2011) Most women aged 18-44 years did not Suggested Citation have adequate fruit and vegetable Vanos H, Larder C, Fussman C, McKane P, Wahl R. Michigan Department of Community Health. “Preconception Health in Michigan: Nutrition and Physical Activity.” 2013. consumption Although disparities in the data were evi- The Health of Women and Girls Factsheet Series Preconception Health in Michigan Preconception Health in Michigan Nutrition Physical Activity Michigan: Physical Activity Nutrition and and Nutrition Physical and Activity Fruit and Vegetable Consumption Figure 2: Prevalence of women aged 18-44 years with self-reported adequate fruit and vegetable consumptiona by age group, 2011 MI -BRFSS Figure 3: Prevalence of women aged 18-44 years with self-reported adequate fruit and vegetable consumptiona by race, 2011 MIBRFSS 50 50 40 40 29.8 23.8 Black Other 30 21.2 22.1 17.9 20 Percent Percent 27.4 30 22.1 20.6 Total White 20 10 10 0 0 Total 18‐24 25‐34 35‐44 Figure 4: Prevalence of women aged 18-44 years with self-reported adequate fruit and vegetable consumptiona by educational attainment, 2011 MI-BRFSS Figure 5: Prevalence of women aged 18-44 years with self-reported adequate fruit and vegetable consumptiona by household income, 2011 MI-BRFSS 40 20.9 40 23.6 30 27.7 25.4 30 16.7 Percent Percent 22.1 20 10 22.1 19.3 Total < $25,000 19.6 20 10 0 0 Total Less than High school high school graduate Some college College graduate $25,000 ‐ $49,000 $50,000 + a Consumption of fruits (including juice) and vegetables at least 5 times per day HP 2020 Goal: Increase the contribution of fruits and vegetables to the diets of the population aged 2 years and older The Health of Women and Girls Factsheet Series Preconception Health in Michigan Preconception Health in Michigan Nutrition Physical Activity Michigan: Physical Activity Nutrition and and Nutrition Physical and Activity Folic Acid Supplementation Overview: Maternal nutrition in the preconcep- tion period and during pregnancy is critically Prevalence of folic acid supplementation was lower than the HP 2020 Goal in wom- 1 important for fetal development. There is a en: considerable amount of evidence that synthetic folic acid supplementation in the preconception period and early gestation has protective mechanisms against several congenital malformations, 1,2,3 Aged 18-24 years Who were Black Enrolled in Medicaid and is also associated with or with no health decreased risk for low birth weight and small for insurance 1 gestational age. With dietary supplementation, certain congenital malformations called neural tube defects (such as spina bifida) can be With low educational attainment With low household income decreased by 60-70%.3,4 Folate is important for Trends Over Time: Prevalence has been the synthesis of DNA and protein, and for constant and consistently achieving and exceed- 2 regulation of DNA expression. For optimal ing the HP 2020 Goal over the years of 2004- protective effects, it is recommended that women 2010. begin folic acid supplementation at least three months prior to conception.4 Preconception Health Indicator: Percentage of References 1. Timmermans S, et al. Periconception folic acid supplementation, fetal growth and the risks of low birth weight and preterm birth: the Generation R study. Brit. J. Nutr. 2009:;102(5):777-785. 2. Boxmeer JC, et al. Preconception folic acid treatment affects the microenvironment of the maturing oocyte in humans. Fertil. Steril. 2008; 89(6):17661770. 3. Persad VL, et al. Incidence of open neural tube defects in Nova Scotia after folic acid fortification. Can. Med. Assoc. J. 2002; 167(3):241-245. 4. Centers for Disease Control and Prevention. Recommendations to improve preconception health and health care—United States. MMWR 2006; 55 (RR06):1-23 women aged 18-44 years having a live birth who took a multivitamin or prenatal vitamin daily during the month before conception Healthy People 2020 Goal: Increase the proportion of women delivering a live birth who took a multivitamin/folic acid prior to pregnancy to 33.1% Key Points (MI-PRAMS, 2010) Most women aged 18-44 did not have Suggested Citation adequate folic acid supplementation one Vanos H, Larder C, Fussman C, McKane P, Wahl R. Michigan Department of Community Health. “Preconception Health in Michigan: Nutrition and Physical Activity.” 2013. month prior to conception The Health of Women and Girls Factsheet Series Preconception Health in Michigan Preconception Health in Michigan Nutrition Physical Activity Michigan: Physical Activity Nutrition and and Nutrition Physical and Activity Folic Acid Supplementation Figure 1: Prevalence of women aged 18-44 years having a live birth with self-reported prepregnancy multivitamin or prenatal vitamin usea by age group, 2010 MI-PRAMS Figure 2: Prevalence of women aged 18-44 years having a live birth with self-reported prepregnancy multivitamin or prenatal vitamin usea by race, 2010 MI-PRAMS 60 40.1 50 50 34.9 40 40 29.2 30 HP 2020 Goal 33.1 % 20 Percent Percent 40.5 60 13.9 31.5 29.2 30 HP 2020 Goal 33.1% 19.3 20 10 10 0 0 Total 18‐24 25‐34 35‐44 Total Figure 3: Prevalence of women aged 18-44 years having a live birth with self-reported prepregnancy multivitamin or prenatal vitamin usea by educational attainment, 2010 MI- PRAMS White Black Figure 4: Prevalence of women aged 18-44 years having a live birth with self-reported prepregnancy multivitamin or prenatal vitamin usea by household income, 2010 MI-PRAMS 60 60 45.8 45.9 50 50 40 30 24.0 HP 2020 Goal 33.1% Percent 40 29.2 23.8 15.2 30 20 10 10 0 26.1 29.2 20 HP 2020 Goal 33.1% 18.4 0 Total Less than High school high school graduate Some college College graduate Total < $25,000 $25,000 ‐ $49,000 $50,000 + Figure 5: Prevalence of women aged 18-44 years having a live birth with self-reported pre-pregnancy multivitamin or prenatal vitamin usea by health insurance, 2010 MI-PRAMS 50 37.4 40 29.2 Percent Percent Other 30 HP 2020 Goal 33.1% 17.3 19.0 a Consumption of a multivitamin or prenatal vitamin daily for one month prior to conception. This is an estimation of folic acid intake. 20 10 0 Total Uninsured Medicaid Private The Health of Women and Girls Factsheet Series Preconception Health in Michigan Preconception Health in Michigan Nutrition Physical Activity Michigan: Physical Activity Nutrition and and Nutrition Physical and Activity Overweight and Obesity Overview: In the past 20 years, the prevalence Healthy People 2020 Goal: Reduce the propor- of obesity in pregnant women and women of tion of adults who are obese to 30.6% reproductive age has increased in many highincome countries.1 Key Points (MI-PRAMS, 2010) Maternal overweight has been associated with years having a live birth were classified increased risk of cesarean section and post- as either overweighta (23.8%) or obeseb operative complications for those deliveries, (22.6%) at the time they became pregnant gestational diabetes, and hypertension. Infants of overweight mothers are more likely to be Over 46% of Michigan women aged 18-44 The prevalence of prenatal obesity was admitted to neonatal intensive care units com- higher among Black women compared to pared to normal-weight mothers.2 White women In obese women, stillbirth is nearly twice as likely 1 compared to normal-weight women. Maternal a BCS ≥ 25 and < 30 based on self-reported height and weight BCS ≥ 30 based on self-reported height and weight b obesity has been associated with numerous Trends Over Time: Prevalence of prenatal over- other poor perinatal outcomes, including preterm weight and obesity has been constant over the delivery, cesarean section, heart defects, neural years of 2004-2010, and obesity has achieved tube defects, macrosomia (excessive birth (remained below) the HP 2020 Goal. weight), low Apgar scores, perinatal mortality, gestational diabetes, hypertension and References preeclampsia, and 1. Vasudevan C, Renfrew M, McGuire W. Fetal and perinatal consequences of maternal obesity. Arch. Dis. Child Fetal Neonatal Ed. 2011; 96(F):378-382 2. Galtier-Dereure F, Boegner C, Bringer J. Obesity and pregnancy: complications and cost. Am. J. Clin. Nutr. 2000; 71(5):1242s-1248s. 3. Centers for Disease Control and Prevention. Recommendations to improve preconception health and health care—United States. MMWR 2006; 55 (RR06):1-23 thromboembolic disease.1,2,3 These risks can be decreased with appropriate weight loss and nutrition in the preconception period.3 Preconception Health Indicator: Percentage of women aged 18-44 years with a Body Mass Index (BMI; weight in kg/height in m2) ≥ 25 but < 30 (overweight) or BMI ≥ 30 (obese) Suggested Citation Vanos H, Larder C, Fussman C, McKane P, Wahl R. Michigan Department of Community Health. “Preconception Health in Michigan: Nutrition and Physical Activity.” 2013. The Health of Women and Girls Factsheet Series Preconception Health in Michigan Preconception Health in Michigan Nutrition Physical Activity Michigan: Physical Activity Nutrition and and Nutrition Physical and Activity Overweight and Obesity Figure 1: Prevalence of women aged 18-44 years having a live birth who were overweighta or obeseb at the time they became pregnant by age group, 2010 MI-PRAMS Figure 2: Prevalence of women aged 18-44 years having a live birth who were overweighta or obeseb at the time they became pregnant by race, 2010 MI-PRAMS 50 24.1 50 31.4 30 HP 2020 Goal 30.6% obese 26.0 21.4 20.2 23.8 22.6 40 22.9 21.4 Overweight Obese 20 30 23.8 22.6 25.8 9.9 23.7 21.1 Overweight Obese 20 10 10 0 0 Total 18‐24 35‐34 35‐44 Total Figure 3: Prevalence of women aged 18-44 years having a live birth who were overweighta or obeseb at the time they became pregnant by educational attainment, 2010 MI-PRAMS White Black Other Figure 4: Prevalence of women aged 18-44 years having a live birth who were overweighta or obeseb at the time they became pregnant by household income, 2010 MIPRAMS 30.4 40 HP 2020 Goal 30.6% obese 40 24.9 26.3 24.0 30 23.8 20.6 22.6 23.6 22.8 30 20 Overweight Obese Percent 18.1 Percent 29.7 HP 2020 Goal 30.6% obese Percent Percent 40 HP 2020 Goal 30.6% obese 24.725.7 25.2 22.9 23.8 22.6 23.5 19.3 20 Overweight Obese 10 10 0 Total a Less than high school High school graduate Some college College graduate 0 Total <$25,000 $25,000 ‐ $50,000 + $49,000 BCS ≥ 25 and < 30 based on self-reported height and weight; bBCS ≥ 30 based on self-reported height and weight The Health of Women and Girls Factsheet Series Preconception Health in Michigan Preconception Health in Michigan Nutrition Physical Activity Michigan: Physical Activity Nutrition and and Nutrition Physical and Activity Exercise and Physical Activity Overview: Physical activity can help individuals minutes per week of vigorous intensity, or an maintain a healthy weight, and can also impact equivalent combination, and also participate in several other aspects of health. It can help lower muscle strengthening activities on two or more blood pressure, reduce the risk for heart attack, days per week, to 20.1%. stroke, type 2 diabetes, several forms of cancer, Key Points (MI-BRFSS, 2011) and osteoporosis, and reduce symptoms of depression and anxiety.1 have adequate physical activity Physical activity during the preconception period has been associated with decreased risk of ges- Most women aged 18-44 years did not Prevalence of adequate physical activity tational diabetes.2,3,4 Gestational diabetes has was significantly lower than the HP 2020 been associated with a predisposition to post- Goal in women: partum type 2 diabetes in mothers.2 Additionally, gestational diabetes and glucose intolerance during pregnancy can increase risk of cesarean section, childhood obesity, and diabetes in children and young adults.3,4 With low household income 3. Baptiste-Roberts K, Ghosh P, Nicholson WK. Pregravid physical activity, dietary intake, and glucose intolerance during pregnancy. J. Womens Health 2011; 20(12):1847-1851 4. tensity for 150+ minutes per week, or 75+ With low educational attainment Retnakaran R, et al. Pre-gravid physical activity and reduced risk of glucose intolerance in pregnancy: the role of insulin sensitivity. Clin. Endocrinolo. 2009; 70 (4):615-622 lent combination of the two aerobic physical activity of at least moderate in- 2. activity for 75+ minutes per week, or an equiva- Increase the proportion of adults who engage in With no health insurance Centers for Disease Control and Prevention. “Healthy weight—it’s not a diet, it’s a lifestyle!” 2011. Available online: http://www.cdc.gov/healthyweight/ physical_activity/index.html. Accessed May 13, 2013. who engage in either moderate physical activity Healthy People 2020 Goal: 1. in leisure-time physical activity, the percentage for 150+ minutes per week or vigorous physical Who were Black References Preconception Health Indicator: Among women aged 18-44 years who participate Tobias DK, et al. Physical activity before and during pregnancy and risk of gestational diabetes mellitus: a meta-analysis. Diabetes Care 2011; 34(1):223229 Suggested Citation Vanos H, Larder C, Fussman C, McKane P, Wahl R. Michigan Department of Community Health. “Preconception Health in Michigan: Nutrition and Physical Activity.” 2013. The Health of Women and Girls Factsheet Series Preconception Health in Michigan Preconception Health in Michigan Nutrition Physical Activity Michigan: Physical Activity Nutrition and and Nutrition Physical and Activity Exercise and Physical Activity Figure 1: Prevalence of women aged 18-44 years who participated in adequate aerobic physical activitya by race, 2011 MI-BRFSS Figure 2: Prevalence of women aged 18-44 years who participated in adequate aerobic physical activitya by health insurance, 2011 MIBRFSS 30 30 20.7 18.7 20 10 13.9 HP 2020 Goal 20.1% Percent Percent 20 11.6 HP 2020 Goal 20.1% 19.5 18.7 12.1 10 0 0 Total White Black Other Figure 3: Prevalence of women aged 18-44 years who participated in adequate aerobic physical activitya by educational attainment, 2011 MI-BRFSS Total No Health Insurance Health Insurance Figure 4: Prevalence of women aged 18-44 years who participated in adequate aerobic physical activitya by household income, 2011 MI-BRFSS 40 30 22.4 26.3 30 20 8.8 20 13.0 HP 2020 Goal 20.1% Percent Percent 18.7 17.0 18.7 19.6 HP 2020 Goal 20.1% 11.5 10 10 0 0 Total a Less than High school high school graduate Some college College graduate Total < $25,000 Either moderate physical activity for 150+ minutes per week or vigorous physical activity for 75+ minutes per week, or an equivalent combination of the two, and muscle strengthening activities on two or more days per week (of those reporting leisure physical activity) $25,000 ‐ $49,999 $50,000+ The Health of Women and Girls Factsheet Series Preconception Health in Michigan Preconception Health in Michigan Nutrition Physical Activity Michigan: Physical Activity Nutrition and and Nutrition Physical and Activity Data Sources Michigan Behavior Risk Factor Surveillance respond by mail. Data are self-reported and sub- System (MI-BRFSS) ject to recall bias.1 However, yearly findings can BRFSS is a joint effort of the CDC and state health depart- be applied to 98% of residents who deliver a live birth in Michigan.4 ments, and is available in all 50 states. It is a telephone health survey of adults aged 18 years and older, whom are selected by random-digit dialing.1 BRFSS methodology recently changed to include cell phone only respondents.2 BRFSS serves as a data source regarding health risk behaviors, preventive health practices, and References health care access. Data are all self-reported, so 1. Broussard DL, et al. Core state preconception health indicators: a voluntary, multi-state selection process. Matern. Child Health J. 2011; 15(2):158168. 2. Centers for Disease Control and Prevention. “BRFSS 2011 Survey Data and Documentation.” 2013. Available online: http://www.cdc.gov/brfss/ annual_data/annual_2011.htm. Accessed May 21, 2013. 3. Larder C, MI PRAMS Epidemiologist. Personal communication, May 14, 2013. 4. Grigorescu et al. Preconception Health Assessment Work Group. “Preconception Health in Michigan.” 2011. this surveillance method is subject to recall bias as people may not remember previous behaviors or health conditions. However, BRFSS is regarded as having moderate to high validity (accuracy).1 Michigan Pregnancy Risk Assessment Monitoring System (MI-PRAMS) PRAMS is a joint effort of the CDC and state health departments, and is available in 40 states and New York City.3 It is a mailed questionnaire sent to a stratified, random sample of women with a live birth in the previous 2-6 months3, gathering data on maternal attitudes, experiences, health behaviors and conditions, and health care access.1 Telephone follow-up is conducted for women who do not Suggested Citation Vanos H, Larder C, Fussman C, McKane P, Wahl R. Michigan Department of Community Health. “Preconception Health in Michigan: Nutrition and Physical Activity.” 2013.