Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
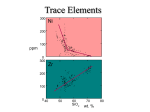
Le linee guida attualmente esistenti per la terapia dell’HAE PERCHÈ TRATTARE L’HAE? • Malattia potenzialmente letale • Inabilità durante gli attacchi • Bassa qualità di vita Perchè non trattare l’HAE? • Gli attacchi potenzialmente letali sono meno del 5% • Gli attacchi non determinano inabilità permanente • Pazienti per la maggior parte asintomatci CRITICITÀ NEL TRATTAMENTO DELL’HAE • Variabilità nella frequenza dei sintomi: • da paziente a paziente • nei diversi periodi della vita • Variabilità nella severità dei sintomi • Lunghezza del trattamento FINALITÀ DEL TRATTAMENTO DELL’HAE • Eliminare la mortalità • Ridurre il tempo durante il quale un paziente soffre per un attacco di HAE STRATEGIE TERAPEUTICHE PER L’HAE E PROBLEMI SPECIFICI • Prevenire gli attacchi • Trattare i pazienti quando stanno bene • Trattare i pazienti per tutta la vita • Ridurre la durata degli attacchi • Non aspettare a trattare un’attacco di HAE • Variabilità nella risposta INDICAZIONI AL TRATTAMENTO • Valutazione della severità della malattia • Misurare la lunghezza degli attacchi • Misurare la frequenza degli attacchi • Identificare la strategia ottimale • Efficacia dei trattamenti • Facilità di somministrazione dei farmaci RISULTATI DEL TRATTAMENTO • Misurare l’efficacia • Risultati riportati dai pazienti • Durata degli attacchi • Ospedalizzazione • Inabilità/complicanze • Misurare gli effetti collaterali • Strategie specifiche per l’HAE HAE Treatment Guidelines Consensus Meeting Gargnano 2010 Criteri di valutazione dell’HAE Agostoni et al 2004 J ALLERGY CLIN IMMUNOL PROPOSTE DAL MEETING DI GARGNANO 2010 • Sistemi per registrare i dati degli attacchi da parte dei pazienti • Facili da completare e inviare • Valutazione della severità • Valutazione della durata • Sistemi di registrazione dei dati per i medici • Unico datbase • Punteggio automatico DISEASE SCORING Gargnano 2010 ATTACK RECORDING • Starting of symptoms • Day and hour • Location of the attack • Performance status • I have no limitations • I can do my activities, but with limitations • I can not do my activities • I went/called the physician • I was admitted to the hospital • Days/hours • Medication • Type • Day and hour • Resolution of symptoms • Day and hour QUALITY OF LIFE QUESTIONNAIRE • At yearly follow up mild moderate severe Trattamento dell’attacco acuto nell’HAE 14 BOWEN ET AL J ALLERGY CLIN IMMUNOL 2004 BOWEN ET AL AACI, 2010 We recommend treating attacks as early as possible Trattamento dell’attacco acuto nell’HAE Evidence based data 16 TRATTAMENTO DEGLI ATTACCHI ACUTI: STUDI MULTICENTRICI, RANDOMIZATI, IN DOPPIO CIECO Study name * First author Year Journal Drug class Drug Controls CINRYZE Zuraw 2010 NEJM C1-inhibitor Cynrize placebo 68 yes IMPACT1 Craig 2009 J Allergy Clin Immunol C1-inhibitor Berinert # placebo 85 yes RHUCIN100 Zuraw 2010 J Allergy Clin Immunol C1-inhibitor Rhucin # placebo 58 yes FAST-1 Cicardi 2010 NEJM Bradykinin B2 receptor Icatibant antagonist placebo 56 no FAST-2 Cicardi 2010 NEJM Bradykinin B2 receptor Icatibant antagonist Tranexamic acid 74 yes EDEMA3 Cicardi 2010 NEJM Kallikrein inhibitor Ecallantide placebo 72 yes 2010 Ann Allergy Asthma Immunol Kallikrein inhibitor Ecallantide placebo 96 yes EDEMA4 Levy * name used in this systematic review # only most effective dosage considered § patients included in this systematic review n included stat patients § sign INIZIO DEL MIGLIORAMENTO DEI SINTOMI GRAFICO RIASSUNTIVO DELLE EVIDENZE CLINICHE Median time to the onset of symptoms relief Ratio treatment/control Kallikrein inhibitor FAST-2 FAST-1 Pooled - Bradykinin receptor antagonist RHUCIN100 IMPACT1 Pooled - C1-inhibitor 0,0 0,1 0,2 0,3 0,4 0,5 Ratio T/C 0,6 0,7 0,8 0,9 1,0 The lower the ratio, the better the treatment Confronto indiretto: non ci sono differenze tra i diversi trattamenti RISOLUZIONE COMPLETA DEI SINTOMI FIGURA RIASSUNTIVA DELLE EVIDENZE Median time to complete resolution of symptoms Ratio treatment/control FAST-2 FAST-1 Pooled - Bradykinin receptor antagonist RHUCIN100 IMPACT1 CINRYZE Pooled - C1-inhibitor 0,0 0,2 0,4 0,6 0,8 1,0 The lower 1,2 the ratio, the better the treatment Ratio T/C Confronto indiretto: non ci sono differenze tra i diversi trattamenti TRATTAMENTO IN ACUTO GARGNANO 2010 • All patients diagnosed with HAE due to C1-INH deficiency should have available at home: • C1-INH (pd 3000 units, rh 4200 units) or • Ecallantide (60 mg) or • Icatibant (60 mg) • Patients should be trained for self administration • All attacks are eligible for treatment as soon as they are recognized • Any of the above drug can be used for any location • Any location can be treated at home • Hospital recommended upon risk of laryngeal involvement Profilassi degli attacchi acuti di HAE 21 Agostoni et al J ALLERGY CLIN IMMUNOL 2004 • Long-term prophylactic treatment is indicated for patients with many harmful and disturbing edema episodes, usually patients with more than 1 attack per month. Longterm prophylaxis may be performed with attenuated androgens, antifibrinolytic agents, and C1-INH concentrate. • All of these medications are associated with potential adverse effects, limiting their use as standard, life-long prophylactic treatment. GOMPELS ET AL. CLIN EXP IMMUNOL 2005 • The regimen for each affected individual should be guided by the severity of the disease. Frequent attacks of peripheral angio-oedema (extremities, trunk), although unpleasant andannoying, are not dangerous and may not require (contingent upon the patient’s judgement) long-term prophylaxis. • Long-term prophylaxis with C1 INH may be necessary in patients where tranexamic acid or steroids are not effective, not tolerated or contraindicated. This may include those with underlying thromboembolic disease or during pregnancy. Prior to recommending regular therapy, access to C1 inhibitor for acute attacks should be optimized, by home therapy training if necessary. In exceptional cases where thisapproach does not provide sufficient symptom control, regular C1 inhibitor infusions of 500–1000 U twice weekly may be required. BOWEN ET AL. ALLERGY, ASTHMA & CLIN IMMUNOL, 2010 • Consider long-term prophylaxis with antifibrinolytics, attenuated androgens, or pdC1INH if more than one severe event per month occurs and if a treatment for acute attacks is not sufficiently effective or is not available. • It should be noted that: the number of events per year does not predict severity of the next event nor whether the first or next event will be an airway event. CRAIG ET AL. ANN ALLERGY ASTHMA IMMUNOL, 2009 Profilassi degli attacchi acuti di HAE Evidence based data 26 PROFILASSI DEGLI ATTACCHI Controls N° included patients cross-over design p <0.05 Aminocaproic placebo 5 yes yes AFs tranexamic placebo 12 yes yes NEJM androgen danazol placebo 9 yes yes 1977 Ann Int Med androgen methyltest placebo 4 yes yes 2002 JACI heparin heparin placebo 15 yes no placebo 6 yes yes placebo 22 yes yes First author Year Journal Drug class Drug Frank 1972 NEJM AFs Sheffer 1972 NEJM Gelfand 1976 Sheffer Weiler Waites 1996 NEJM vaporC1 inhibitor heated C1 inhibitor Zuraw 2010 NEJM C1 inhibitor C1inhibitor Study Id METANALISI DEI DIVERSI STUDI CLINICI 7.0 Drug RR (95% CI) 6.0 Aminocaproic acid 0.095 ^ (0.025-0.356) 5.0 Tranexamic acid 0.308 § (0.195-0.479) Pooled 0.204 (0.068-0.611) Danazol 0.023 ^ (0.003-0.162) Methyltestoren e 0.054 § (0.013-0.163) Pooled 0.044 (0.017-0.114) C1 inhibitor 0.491 § (0.395-0.607) 4.0 3.0 2.0 1.0 0.0 0.00 Better0.10 0.20 0.30 0.40 0.50 0.60 0.70 0.80 Relative risk Drug vs Placebo Red: Androgen; Blu: Antifibrinolytics; Green: C1 inhibitor Beware heterogeneity! ^ attacks per cycle § attacks per month PROFILASSI DEGLI ATTACCHI ACUTI GARGNANO 2010 Long term prophylaxis • Should be considered when optimized on demand therapy fails for a documented reason as for example: • > 24 days with angioedema per year or • >12 severe attacks per year • Drugs • androgens • >16 year • no pregnancy • C1-INH • when androgens contraindicated/not accepted/>200 mg danazol daily. • Doses should be titrated individually (usually two infusions of 1000 U. per week)