Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
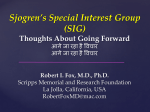
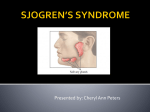
3/3/2014 The Patient with Pain All Over “All the Pearls in 50 Minutes” Gerald F. Falasca, M.D. Rheumatology Johnson City, TN March 26, 2014 GOALS • Become a better diagnostician. • Diagnose undifferentiated connective tissue disease (UCTD) and primary Sjogren syndrome. • Understand treatment of UCTD, polymyalgia, fibromyalgia, and polymyositis. A 70 year old woman presents with widespread pain, stiffness and fatigue. She recently started keeping a water bottle at her bedside. Physical exam is remarkable for slight synovitis of hands & wrists, and presence of all fibromyalgia tender points. Lab data is notable for sed rate of 30 mm/hr but normal CRP at 0.7 mg/dl (nl 0 ‐ 1.0 mg/dl), elevated C4 at 36 mg/dl. RF, CCP & ANA are negative. What is the most likely diagnosis? 1 3/3/2014 A. Paraneoplastic syndrome B. Polymyalgia rheumatica C. Rheumatoid arthritis D. Fibromyalgia E. Primary Sjogren syndrome CONDITIONS ASSOC. WITH WIDESPREAD PAIN – Fibromyalgia – Influenza – Depression – Hypothyroidism – Anxiety – Hepatitis C – Drugs (statins, fibrates) – Hyperparathyroidism – Drug seeking behavior – Ankylosing spondylitis – Sjogren’s / UCTD – Lyme disease – Rheumatoid arthritis – Sarcoidosis – SLE – Polymyalgia rheumatica – Hypermobility – Osteomalacia (<10 ng/ml) – Peripheral neuropathy – Bone marrow abnormalities CONDITIONS ASSOC. WITH WIDESPREAD PAIN • Fibromyalgia • Drugs (statins, bisphosphonates, aromatase inhibitors) • Sjogren’s / UCTD / SLE • Polymyalgia rheumatica • Hypermobility • Ankylosing spondylitis • Osteomalacia 2 3/3/2014 Primary Sjogren’s • • • • Fatigue Pain all over Sicca Many persons with Sjogren’s fulfill criteria for fibromyalgia. Iannuccelli C et al. Fatigue and widespread pain in systemic lupus erythematosus and Sjögren's syndrome: symptoms of the inflammatory disease or associated fibromyalgia? Clin Exp Rheumatol. 2012 Nov‐Dec;30(6 Suppl 74):117‐21 What’s in a name?? • Sjogren’s (primary) vs. undifferentiated connective tissue disease – Sometimes hard to distinguish initially – Both can be associated with widespread pain. – As is SLE. What Are the Clues? • • • • • • • • Sicca symptoms Acrocyanosis Raynaud’s Family history Puffy hands Peripheral arthralgias Photosensitivity Alopecia 3 3/3/2014 Sjogren’s - History • Use of eye drops? • Can you eat crackers w/o water? • Keep water on night table? • Physical Exam: Nothing specific! – Sometimes small joint puffiness – Peripheral neuropathy 4 3/3/2014 Sjogren’s - Diagnosis • You Can Diagnose Dry Eyes and Dry Mouth in Your Office! • Phenol Red Thread Test – Zone-Quick™ • Saxon Test of Salivary Flow Phenol Red Thread Test (Zone-Quick™) • Alternative to the Schirmer test • Takes 15 seconds; convenient screening test • A test for dry eyes (not a direct test for Sjogren’s!) I De Monchy et al. Combination of the Schirmer I and phenol red thread tests as a rescue strategy for diagnosis of ocular dryness associated with Sjögren's syndrome. Invest Ophthalmol Vis Sci. 2011 Jul 15;52(8):5167‐73. 5 3/3/2014 Saxon Test of Salivary Flow • Takes 2 minutes • Requires a scale that can measure to 0.1 gram (costs $100). • Uses 4” x 4” medical gauze sponge. Kohler PF, Winter ME. A Quantitative Test for Xerostomia: The Saxon Test, an Oral Equivalent of the Schirmer Test. Arthritis Rheum. 28(10) 1128‐32, 1985. 6 3/3/2014 Saxon Test • Weigh the gauze in the cup • Patient chews gauze for 2 min. • Weigh gauze again in cup. Saxon Test • Most persons produce about 4g of saliva in 2 minutes. • Abnormal if < 2.75 g in 2 minutes. • Should D/C anticholinergic meds day before to avoid false positive. • Anxiety may also give false positive. 7 3/3/2014 Sjogren’s / UCTD - Lab • • • • • • • • • SSA / SSB – insensitive! ESR often up – a little! ANA – speckled or negative CRP high normal (0.7 to 0.9 mg/dl) Check RNP antibody Check ACE level Check ANCA Check SPEP Check C4 (may be high or low!) HIGH ACE LEVELS • • • • • • • Sarcoidosis NIDDM Hyperthyroidism Renal disease Cirrhosis TB Gaucher • • • • • • Sjogren’s Histoplasmosis ? Berrylosis Leprosy Amyloidosis Silicosis Sjogren’s – Systemic Tx* • • • • • Hydroxychloroquine Low-dose prednisone Methotrexate Cyclosporine Fibromyalgia treatments (for symptoms) *None of these is FDA approved for systemic Sjogren’s 8 3/3/2014 Polymyalgia Rheumatica • • • • • • • • Pain all over; sudden onset. Age > 50 (usually >70!) Weight loss Shoulder limitation of motion (periarthritis) Proximal muscle tenderness Sed rate > 50 mm/hr Anemia Prompt response to low dose prednisone Polymyalgia Rheumatica • 10-15% progress to giant cell arteritis. • Responds well to treatment. • This is a potentially serious disease that is treatable. From onmyfrontporch.com 9 3/3/2014 PMR – More Features • Bilateral shoulder limitation of motion • Synovitis (large > small joint) • Bilateral carpal tunnel synd. • Profound AM stiffness, gelling • Strength is normal (just painful). • Proximal muscle tenderness is different from FM tender points. PMR – DDx (Pain, Stiffness +/- High ESR) • • • • • • Fibromyalgia Polymyositis Rheumatoid arthritis Lupus Hypothyroidism Malignancy PMR or GCA - Lab Features • High ESR > 40 mm/hr, often 100. – Occasionally normal! • Elevated CRP. • Anemia, sometimes < 10g/dl. • High alk phos (1/3 patients), sometimes ALT, AST. • Low albumin. • High globulins (polyclonal) • CK, ANA, RF normal! 10 3/3/2014 PMR – When to Biopsy? • 15-20% of PMR patients have GCA. • PMR + Headache = Biopsy. • PMR + Any other symptom of temporal arteritis = biopsy. • ESR/CRP not normalizing on low dose pred. (3-4 weeks) PMR - Treatment • Prednisone 15-20 mg/d • Dramatic response (1-2 days) • Try tapering by 2.5 mg/mo till 10 mg/d, then more slowly (by 1 mg/mo). • Follow ESR, CRP monthly. Check BMP, CBC occasionally. • Inform patient symptoms of GCA to report immediately. PREDNISONE in ELDERLY • • • • • Calcium + Vit D DEXA T/C bisphosphonate Eye exams: cataracts & pressure ↓K, ↑glucose 11 3/3/2014 Amer. College of Rheum. • Recommendations for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis 2010 • Arthritis Care & Research, Vol. 62, No. 11, November 2010, pp 1515– 1526 • DOI 10.1002/acr.20295 PMR - Course • Many patients don’t follow textbook. • Many patients require chronic steroids (2-5 mg/d). • May progress to GCA, even 5 years later. • Relapses occur. ESR may be normal with relapses. WIDESPREAD NIGHT PAIN • • • • • PMR Peripheral neuropathy Fibromyalgia Depression Malignancy (HPO) 12 3/3/2014 CHRONIC INFLAMMATION The Telltale Signs • Anemia, normocytic or slightly microcytic • High platelets • Low albumin • High globulin Statin Myopathy • Dose related • Risk lowest with pravastatin, fluvastatin, rosuvastatin. Graham DJ et al. Incidence of hospitalized rhabdomyolysis in patients treated with lipid‐lowering drugs. JAMA. 2004;292(21):2585. Ridker PM et al. Rosuvastatin to prevent vascular events in men and women with elevated C‐reactive protein. N Engl J Med. 2008;359(21):2195 Statin Myopathy Risk Factors • • • • • • Hypothyroidism Renal insufficiency ALS Congenital myopathies SLCO1B1*5 variant Interacting drugs Vladutiu GD. Genetic predisposition to statin myopathy. Curr Opin Rheumatol. 2008;20(6):648. 13 3/3/2014 Statin Myopathy Syndromes • • • • Myalgias CK elevation, asymptomatic Myositis, rhabdomyolysis Persistent autoimmune myopathy Mohassel P et al. The spectrum of statin myopathy. Curr Opin Rheumatol. 2013 Nov;25(6):747‐52 Thompson PD et al. Statin‐associated myopathy. JAMA. 2003;289(13):1681. WHAT IS FIBROMYALGIA? • A syndrome of widespread pain and fatigue associated with multiple tender points and nonrestorative sleep. • More than 3 months • Normal blood tests MAJOR SYMPTOMS • • • • “Non-restorative” sleep Chronic fatigue Ache all over Presence of “tender points” (1990 criteria) 14 3/3/2014 OTHER SYMPTOMS • Fatigue • Sleep Disturbance • Headaches (migraine or tension) • GI symptoms (IBS) • Irritable bladder • Panic attacks (20%) • Vasospasm (40%) • • • • • Dysmenorrhea Dry mouth Poor memory TMJ Subjective swelling The Common Associates of Fibromyalgia • • • • Migraine headaches Irritable bowel Irritable bladder Panic attacks Who gets FMS? • • • • Up to 2% of population. Most common in middle-aged women 8-9 females to 1 male approx. Patients with RA, SLE and ankylosing spondylitis often meet criteria. • Tends to run in families. 15 3/3/2014 TRIGGERS OF FLARES The Usual Culprits • • • • • Unaccustomed exertion Anxiety or emotional stress Inadequate or unrestful sleep Cold exposure, changes in weather Soft tissue injuries FMS – THE ACR CRITERIA American College of Rheumatology 1990 (There are also 2010 criteria pending) • Widespread pain, 3 months duration • Above and below waist; bilateral • Axial pain (shoulders, back, chest) – 10 of 18 tender points • "Painful," not just "tender" • 4 kg force (9 lb.) needed • Wolfe F, Smythe HA: Arthritis Rheum 33:160, 1990 Pathogenesis 16 3/3/2014 THE CONTROL POINTS – Distal, dorsal third of forearm – Midfoot, dorsal 3rd metatarsal – Dorsal, 3rd metacarpal – Thumbnail – Forehead Mimics of Fibromyalgia • • • • • • Sjogren’s, RA, SLE Spondyloarthropathy Polymyalgia rheumatica Myositis (statin myopathy) Hypothyroidism Depression PREDISPOSED PERSONALITY TRAITS • • • • • • • Reliable, hardworking Attention to detail, tries to please People-oriented, sensitive Internalizes conflict & stress Slightly higher anxiety level Difficulty learning to relax Occupation: elementary school teacher 17 3/3/2014 Clues that Fibro May Be Due to a Connective Tissue Disease • • • • • • • Acrocyanosis or True Raynaud’s Dry eyes and mouth Hand involvement Family history of autoimmunity Low C4 Elevated C4 Positive ANA, high ESR A DIAGNOSTIC CHALLENGE • More lab evaluations • More imaging studies • More surgery (back, neck, abdominal, gynecologic.) THE BASIC LAB EVAL. – CBC – Comp. metabolic panel – ANA – TSH – ESR, CRP – CK 18 3/3/2014 THE COMPLETE LAB EVAL. • CBC • CMP • ANA* • ESR, CRP • SSA/SSB • • • • • • TSH C3, C4, C2 ACE level SPEP ANCA* 25 OHD • RNP • CK *If positive, then follow up with subtyping. Pathogenesis • • • • • • Genetics Altered pain processing Sleep disturbance Neurohumoral perturbation Autonomic abnormalities Immunologic abnormalities NEUROENDOCRINE ABNORMALITIES • • • • • Reduced 24 hour free cortisol Heart rate fluctuations, orthostasis Blunted pituitary response Impaired growth hormone secretion Low IGF-1 levels 19 3/3/2014 • FMS is associated with chronic low back pain (CLBP). • 19% of pts with CLBP have FM tender points Weiner, DK. J Am Geriatr Soc. 2006 Jan;54(1):11-20. Does Fibromyalgia Predispose to a Poorer Surgical Outcome? A cause of prolonged post-op recovery in many studies. . TREATMENT PRINCIPLES FOR FMS – Patient education – Improve sleep hygiene – Aerobic exercise – Medications – Possibly treat anxiety, depression 20 3/3/2014 TREATMENT - 1 • Reassurance: – Not life threatening – Not crippling – Can be lived-with TREATMENT - 2 • IMPROVE SLEEP HYGIENE – Get enough sleep. – Don’t take your troubles to bed. – Avoid caffeine, nicotine, alcohol (late in day) 21 3/3/2014 TREATMENT - 3 • PHARMACOLOGIC (FDA Approved) – Duloxetine (Cymbalta®) – Milnacipran (Savella®) – Pregabalin (Lyrica®) Duloxetine ClinicalTrial TREATMENT - 4 • PHARMACOLOGIC – Amitriptyline – Cyclobenzaprine – Gabapentin 22 3/3/2014 POLYMYOSITIS – Weakness is the key, not pain • Stairs, combing hair, getting out of car – Waddling gait – May have arthralgias, myalgias – CK, ESR may be normal in 10%! 23 3/3/2014 A 70 year old woman presents with widespread pain, stiffness and fatigue. She recently started keeping a water bottle at her bedside. Physical exam is remarkable for slight synovitis of hands & wrists, and presence of all fibromyalgia tender points. Lab data is notable for sed rate of 30 mm/hr but normal CRP at 0.7 mg/dl (nl 0 ‐ 1.0 mg/dl), elevated C4 at 36 mg/dl. RF, CCP & ANA are negative. What is the most likely diagnosis? A. Paraneoplastic syndrome B. Polymyalgia rheumatica C. Rheumatoid arthritis D. Fibromyalgia E. Primary Sjogren syndrome E.Primary Sjogren syndrome • Sicca • Synovitis • Elevated C4, elevated ESR, high normal CRP. 24 3/3/2014 25