Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
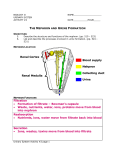
The Roles of the Nephron of the 120 ml of blood that is filtered by the kidneys each minute, only I ml (that's less than I%) turns into urine that will eventually leave the body (after approximately 300 - 400 mis of it accumulates to fill the bladder!) That leaves 119 ml of fluid called filtrate to be returned back to the blood stream. Good thing, otherwise you would have to micturate (pee, urinate) once every 3 minutes and drink 1 L of fluid every 10 minutes in order to maintain Homeostasis!!! The one million nephrons in each human kidney are amazingly efficient at selectively removing wastes from the blood while at the same time conserving water, salt ions, glucose and other needed materials. The nephrons accomplish this task in 3 main steps; these 3 steps are also called the 3 main roles of the nephron: Filtration, Reabsorption and Secretion. Fiftratffln Filtration is aecomplished by the movement of fluids from the blood into the Bowman's capsule. Beabsorpttort Reatuorptias wolves the selective transfer of essential solutes and water back into the blood. Secretion Secretion Involves the movement of wastes from the blood into the mphron. 1. Filtration The renal artery carries blood into the kidney (approximately 600 mis of blood enters a kidney each minute). The renal artery then branches into arterioles which then branch intoaspecialized capillaries called the glomerulus. Because of the great difference in diameter between the renal artery and the glomerul us, blood entering the glomerulus is under very high pressure. This pressure forces about 20% of the blood plasma (about 120m1 of the 600 ml) out of the glomerulus and across the membrane of Bowman's capsule. Bowman's capsule acts to "filter" or separate some of the substances that are located in blood plasma from others. This is because some substances are small enough to fit through the pores of the membrane of Bowman's capsule and some are too large and thus do not enter Bowman's capsule with the rest of the blood plasma. Water, salt ions (sodium, potassium and choride), glucose molecules, amino acids and urea molecules are all small enough to go through the membrane pores into Bowman's capsule. Blood cells (rbc, wbc and platelets) and proteins on the other hand are too large to leave the capillaries or enter Bowman's capsule. The fluid inside of Bowman's capsule gets a name change; it is now called "filtrate" because it is blood plasma that has been filtered, This filtrate is identical to blood plasma minus the blood cells and proteins. Filtrate is said to be isotonic to blood plasma with respect to its concentration of water, salt ions, glucose, amino acids and urea. The filtrate will then proceed from Bowman's capsule through the rest of the nephron in the following order: proximal convoluted tubule, loop of henle, distal convoluted tubule and finally the collecting tubule. From the collecting tubule, the filtrate will enter the pelvis of the kidney and be called urine. 2. Reabsorption Useful materials such as sugars and salt ions are reabsorbed back into the blood stream. That is, materials that could still be used by the body are sent back to the blood. Reabsorption happens as filtrate passes sequentially through the nephron. Materials re-entering the blood stream do so through the capillary network surrounding the nephrons. In short, "good" stuff is sent from the nephron back into the blood. A. Proximal Convoluted Tubule (PCn: As the filtrate enters the PCT approximately 80% of the salt ions (sodium and potassium), glucose and amino acids are ACTIVELY TRANSPORTED out of the PCT and back into the blood stream by special "pumping" cells located in the walls of the PCT. The process of active transport requires energy. Energy in the form of ATP is supplied by the numerous mitochondria that are embedded in the walls of the PCT. Because of ionic attraction, negatively charged chloride ions (CI-) will flow passively out of the PCT as they are attracted by the positively charged sodium and potassium ions (Na+, K+). As the concentration of the above mentioned solute molecules drops inside of the PCT, water then diffuses out of the PCT and into the capillary network passively by the process of OSMOSIS. The lining of the PCT contains microvilli to increase the surface area over which this reabsorption can occur. B. Descending Loop of Henle: As the filtrate travels into the descending Loop of Henle, both sodium and potassium ions passively diffuse from the salty tissues of the surrounding medulla BACK INTO the Loop of Henle. (Although this is reabsorption of materials, the materials are not going back into the blood stream at this point). At the same time, water continues to move out of the Loop of Henle and into the capillary network by osmosis. The filtrate at this point is more concentrated (hypertonic) with respect to salt ions than it was in the PCT, both because water has been removed from it, and because salt ions have been again added to it. C. AscendineLoop of Henle As the filtrate proceeds up into the ascending Loop of Henle, the choride ions are actively pumped back out of the nephron. Because of ionic attraction, sodium ions then passively follow the chloride ions out of the tubule and into the tissues of the medulla. These ions only move into the medulla and not back into the blood stream. Since the ascending Loop of Henle is impermeable to water, water cannot leave this part of the nephron. Because of this, the filtrate gets more dilute again. Because the opposite happens in the ascending and descending Loops of Henle, the process is called the COUNTER CURRENT MECHANISM. The process is also known as the CHLORIDE SfUFT. D. Distal Convoluted Tubule (DCT) As the filtrate passes through this part of the nephron, water continues to passively diffuse out of the nephron and back into the blood. Water continues to diffuse out of the DCT because the surrounding tissues of the medulla are now very salty due to so much sodium and chloride ions accumulating there. The salty tissues attract the water out of the DCT because the medulla is hypertonic with respect to salt concentration when compared with the salt concentration of the filtrate (now hypotonic). Water that enters the medulla will then diffuse back into the blood stream. Because of the continual re-absorption of water, the filtrate becomes more and more concentrated with wastes, mainly urea. The amount of water that diffuses can be regulated by a hormone called ADH. The amount of water that diffuses from the DCT back into the blood depends on the needs of the body; if the body is dehydrated, more water will go back into the blood, and less will be left in the nephron to make less urine. The opposite occurs if the body is over hydrated. E. Collectin g Tubule C The same thing that occurs in the DCT also occurs in the CT 3. Secretion Occurring at the same time as reabsorption is a process called secretion. Secretion is when a cell releases a substance to its outside... in this case, non-useful and toxic substances are ACTIVELY TRANSPORTED from the blood into the nephron - usually in the regions of the distal and proximal convoluted tubules. Substances which are secreted include excess acid (H+) or base (OH-) ions, excess glucose (high glucose levels are found in diabetic urine or urine of someone who has recently consumed a large amount of sugar-this is the kidney's way of helping to ensure that the blood sugar level doesn't get too high), ammonia, and drugs (this is why urine is used from many drug tests - the breakdown of many drugs including marijuana, cocaine, heroin, sleeping pills, codeine and many other medications can be detected even in minute amounts in the urine). The process of secretion ensures that materials that are potentially harmful to the body are quickly disposed of by being "dumped" into the fluid that is about to become urine. Secretion happens mainly in the regions of the DCT and CT but some also occurs in the PCT. In short, secretion involves "bad" stuff being removed from the blood being sent to the urine. The Counter Current Mechanism of the Nephron The loop of Henle works toward the goal of water conservation. Animals that live in a terrestrial environment need to be careful not to waste water. It is clearly a waste,if water is in short supply, to release too much water with the urine. As a result there needs to be a mechanism to encourage water out of the urine and back into the blood. The loop of Henle creates that mechanism in terrestrial animals. There i s no way of actively capturing water in the urine that is passing through the collecting ducts. It would almost seem too late to capture the water that is already on its way out of the body. However, the nifty nephron creates a trick with its loop of lienle to get the of the loop after chlorine. The sodium rushes out by diffusion because of its 'fatal attraction' to chlorine. The chlorine and the sodium ions collect and dominate the fluids outside the loop of I-fenle creating a salty environment. This salty environment catches the attention of the water that is passing through the nearby collecting duct. The collecting duct is permeable to water but not permeable to the salt. Water can. not resist moving into the salty medulla. The salt creates an osmotic pressure that pulls the water out of the collecting duct by osmosis. (Water has a 'fatal attraction' to salty solutions.) Once the water is out of the duct it is no longer destined for elimination but can' now be picked up by the nearby. ,Mood capillaries and returned to be used by;.body systems. Meanwhile, back at the loop of`-•Henle, trouble is starting. The ascending loop is water out of the collecting duct before it leaves running out of salt. There is no need to worry. It does so by creating a salty The salt trick can continue because the environment in the medulla area of the descending loop in its wisdom is stealing back kidney. the salt that the ascending loop is so generously the kidney, The ascending loop of Henle actively releasing. This helps to keep a constant flow of transports chlorine ions out of the filtrate with salt inside the loop for the ascending lope to Chlorine builds up in the pump out . Because of the generosity gfthe fluids of the medulla by active transport. ascending loop and the stinginess of the Because it is a negative ion, it creates a cause descending loop a salt trade or salt current is for the sodium ion, which is positive, to rush out established as the salt moves ouc of the carrier proteins. ascen ding loop and into the descending loop, This salt current established by the loop of lienle maintains an environment that attracts water out of the ducts containing urine and back into the blood. This process is called the counter current mechanism. (ER 25 Nctwp ruti"n -i^ Urea _, EXCRETION AND WE BALANCING OF WATER AN i Tubular secretion How Materials Move Into and Out of the Nephron As Urine Forms. As a Al. nephron extends through the kidney's cortex and medulla and dumps urine into the collecting duct, various substances enter and leave the filtrate. Broken lines represent segments of the nephron wall that are permeable to water, while solid lines represent wall segments impermeable to water. Narrow arrows represent passive diffusion of materials into or out of the nephron tubule, while wide arrows represent active transport against concentration gradients. Filtration activities are shown in blue, tubu.l 'eabsorption activities in green, and tubular secretion in yellow. U ne is shown as yellow. traces nephron function and material movements step by step. The t Cl I FI2u Cw^^1ed ^- t om) wastes and needed substances filtered into capsule ` blood with high proportion of waste products • 0 • • • .• •• • :`•a • • 0 reabsorption of needed products FU",t.Ic r1<3.N4 Cliff ysr aL ^G'`^ blood with lower proportion of wastes and reabsorbed nutrients and ions ^"- flow of flit:ate o: Jr -)e ^"" c CtIVe :: r r, of Na4' Pas ve Ci Ii nsW r of Na+ pd.tijl'Je L:t.`usif. it rd H,C) !ggmre5 indwam sodium concentration in hundred i r iiinormality