Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
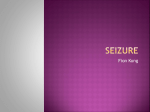
UNIVERSA - - Juli September 2006 Vol. 25, No.3 Number of pre-treatment seizure as prognostic factor of convylsive epilepsy in childhood and young adult onset Efek hipoglikemik daging buah ma h kota dewa (Phaleria Macrocarpa (Scheff.) Boerl.) terhadap kadar gula darah pada manusia sehat setelah pembebanan glukosa Pengaruh olahraga aerobik terhadap kadar estradiol pada wanita pascamenopause : studi randomsasi selama 12 minggu The relationship between maternal blooc zinc level and the size of newborn baby Diagnosis dan penatalaksanaan hand-arm vibration syndrome pada pekerja pengguna alat yang bergetar Nutrition and .immune system in the elderly Universa Medicina Jurnal Kedokteran Trisakti DAFTAR IS1 Halaman Editorial : Psychosomatic medicine, past and future.. A. Prayitno ............................................... Tips of Today Life-threatening malfunction of implantable cardiac devices................................ Number of pre-treatment seizure as prognostic factor of convulsive epilepsy in childhood and young adult onset.. ........................................................................ Rizaldy Pinzon, Harsono, Imam Rusdi i ... 111 105 Efek hipoglikemik daging buah mahkota dewa (PhaleriaMacrocarpa (Scheff.) Boerl.) terhadap kadar gula darah pada manusia sehat setelah pembebanan glukosa.. ............. 114. Meiyanti, Hedi R. Dewoto, Fransiscus D. Suyatna Pengaruh olahraga aerobik terhadap kadar estradiol pada wanita pascamenopause: studi randomisasi selama 12 minggu.. ............................................................ 121 Martiem Mawi, Reza Tandean, Jemmy Hermawan, MR. Rachmawati, Lie T. Merijanti, Nugroho Abikusno fie relationship between maternal blood zinc level and the size of newborn baby.. ...... 127 Widagdo, Harmon Mawardi, Firda Fairuza, Meiharty B. ZulkiJli, Tjahaya Bangun, Augustine Matatula, Slamet Zaeny Diagnosis dm penatalaksanaan hand-arm vibration syndrome pada pekej a pengguna alat yang bergetar.. ................................................................................... 133 Diana Sarnara Nutrition and immune system in the elderly.. .................................................... 140 R i m K, Kusumaratna Number of pre-treatment seizure as prognostic factor of convulsive epilepsy in childhood and young adult onset Rizaldy Pinzon", Harsono**, dan Imam Rusdi** 'Neurology Department, Dr. Haulussy District ~ o s ~ i t~aml b o n "Neurology Department, Gadjah Mada University School of Medicine ABSTRACT Epilepsy is one of the most common neurological disorders with complex problem. The role of number of pretreatment seizure is not conclusive yet. A historical cohort design was conducted to evaluate the role of number ofpretreatment seizure as predictive factor of remission. The subjects were epilepsy patients with onset 2-25 years old with convulsive seizure manfestation that at least had taken medication for 2 years. This study included 110 epilepsy patients, consisted of 42.7% male and 57.3%female. Six months remission with 2 years medication were achieved in 86patients (78.2%). The sign $cant predictive factors for not achieving 6 months remission are seizure type, number ofpre treatment seizure, and the presence of neurological dejcit. Twelve months remission were on[y achieved by 48 patients (43.6%). The sign$cant predictive factors for not achieving 12 months remission were high number ofpretreatment seizure, the presence of neurological dejcit, and the incompliance of treatment program. The average numbers of breakthrough seizure were sign$cant[y higher in patients with high number of pre treatment seizure, presence of neurological dejcit, partial type of epilepsy, and non-compliancepatients. Most epilepsy patient achieved 6 months remission with treatment, but on[y about hayof them achieved 12 months remission. High number of pre treatment seizure was sign $cant poor predictive factors for achieving remission. The strongest poor prognostic factors were the presence of neurological deficit. Keywords: Epilep~y,childhood, young adult, pre treatment seizure Jumlah bangkitan sebelum terapi rutin obat anti epilepsi sebagai faktor prognosis epilepsi masa anak-anak dan dewasa muda ABSTRAK Epilepsi merupakan salah satu penyakit neurologi utama dengan masalah yang kompleks. Peran jumlah bangkitan sebelum terapi rutin sebagai faktor prognosis sampai saat ini masih kontroversial. Sebuah rancangan kohort historikal digunakan untuk menilai peran jumlah bangkitan sebelum terapi sebagai salah satu faktor prediktor remisi epilepsi. Subyek penelitian adalah pasien epilepsi dengan onset pada usia 2-25 tahun, yang telah mendapat terapi minimal selama 2 tahun. Hasil penelitian diperoleh dari 110 pasien epilepsi, terdiri dari 42,794 laki-laki dan 57,3% perempuan. Remisi minimal 6 bulan dengan terapi 2 tahun tercapai pada 86 pasien (78,2%). Faktor prediktor tercapainya remisi adalah tipe bangkitan, jumlah bangkitan sebelum terapi, dan ada tidaknya defisit neurologi penyerta. Remisi 12 bulan tercapai pada 48 pasien (43,696). Faktor prediktor remisi yang penting adalah jumlah bangkitan sebelum terapi, adanya defisit neurologi, dan kepatuhan terhadap program terapi. Jumlah bangkitan dalam program terapi secara signifikan lebih tinggi pada kelompok dengan jumlah bangkitan sebelum terapi yang tinggi, pasien dengan defisit neurologi, tipe epilepsi yang parsial, dan pasien yang tidak patuh. Sebagian besar pasien epilepsi dapat mencapai remisi 6 bulan, namun hanya kurang lebih separuh pasien yang mencapai remisi 12 bulan. Jumlah bangkitan yang tinggi sebelum terapi merupakan faktor prediktor buruk tercapainya remisi. Faktor prediktor yang paling bermalaa untuk tidak tercapainya remisi adalah adanya defisit neurologi yang menyertai epilepsi. Kata kunci: Epilepsi, anak-anak, dewasa muda, jumlah bangkitan sebelum terapi Korespondensi : "Rizaldy Pinzon Neurology Department Dr M Haulussy District Hospital Ambon Elnail : [email protected] B'nzon, Warsono, %us& INTRODUCTION Prognostic factor of convuljive epihpsy in childhood and young adult onset of convulsive seizure. Epilepsy is o n e o f t h e most common neurological disorder with complex additional METHODS problems.(')Epilepsy patients have greater probability for being injured, death, social Research design stigma, fear, anxiety, cognitive disturbance, and Historical cohort design was used in this psychiatric disorder.t2)Theestimated number of study. This design was used to follow up the epilepsy patients worldwide in 2000 are 50 cohort that had been established in the past. A million patients, 37 million patients among them good quality secondary data was needed to are primary type, and 80% lives in developing support the historical cohort study.('*) countries.(')Epilepsy is a chronic disorder that commonly cause medical and quality of life Subjects problem among the sufferer.(3)Epilepsy affect The subjects of this study were childhood the patients, the family, and the neighb~rhood.(~)and young adults onset with convulsive epilepsy Adequate information should be given to the that have taken medication for at least 2 years. patients and their family. Adequate information The point to start t h e follow up was the is very important for enhancing the compliance beginning of medication administration. The inclusion criteria were: (i) childhood and young of therapeutic p r ~ g r a m . ' ~ , ~ ) The main concept of prognosis in epilepsy adult onset epilepsy (2-25 years old), (ii) is the chance for achieving remission and convulsive type of seizure, (iii) had been taken probability of premature death.(') The other medication for minimally 2 years, (iv) obtained p r o g n o s t i c c o n c e p t s a r e q u a l i t y o f life, clinical service for the epilepsy in Sardjito psychosocial status, the neurological function, General Hospital, (v) accompanied with parents and ability for formal edu~ation.(~)Recurrent and or relative at hospital visit, and (vi) had prolonged seizure are believed for causing brain completed medical record. The exclusion criteria damage. Epilepsy is also thought to be a are (i) subject who refused to join the study, and progressive disease. The brain damage is caused (ii) the patients and the family were not sure by prolonged exposure to the excitatory amino about the number of pre treatment seizure. acid (particularly gl~tamate).'~) The development of new epileptic focus in recurrent and prolonged Clinical variable seizure are believed to be facilitated phenomenon The measurement of prognostic factors (kindling model of epilepsy). Primary epileptic performed for each clinical variable, number of focus can induce the surrounding brain area, and pre-treatment seizure, and compliance of c a u s e s a b n o r m a l paroxysmal electrical treatment program. T h e clinical a n d activity.('O)The recurrent electrical stimulation demographic factors that were measured were also causes increasing brain sensitivity and sex, age, type of epilepsy, the origin of epilepsy, permanent declining of seizure threshold.(") the presence of neurological deficit, and EEG Previous studies showed that the role of number profile. Patients were classified into 2 main of pre-treatment seizure as prognostic factors groups based on the number of pre-treatment is still controversial. seizure, namely high number of pre-treatment The aim of this study is to measure the role seizure when the seizure exceeded 10 times of pre-treatment seizure as prognostic factors before treatment. Outcome The primary outcome is minimally 6 months c o n t i n u o u s remission in 2 years treatment. The secondary outcome is 12 months continuous remission and average of months with positive breakthrough seizure. The use of 6 months remission is based on the review of Carpay, et al.(I3)which showed that 2 6 months was a profile of good remission. Patients that achieved 6 months continuous remission had great probability of achieving full remission. Statistical analysis The probability for achieving remission was described with relative risk, the precision o f m e a s u r e m e n t w a s s h o w n with 9 5 % confidence interval. The presence of confounding factors were controlled by multiple logistic regression analysis. The survival analysis with Kaplan-Meier method use to describe the probability for achieving remission in particular time. The statistical package programs used in this study were SPSS 10.0 and Epi Info 6.0. RESULTS Patients characteristic The data were obtained from 110 patients with convulsive epilepsy, consist of 47 (42.7%) male and 63 (57.3%) female. The characteristic of the patients were showed in Table 1. More than 30% patients took their routine medication after more than ten convulsive seizure, and only 18.2% cases had been treated after their first seizure. Among the group that had been treated after their first seizure, most of them had general tonic clonic seizure. In contrast, of 11 patients with partial complex seizure. 81.8% were treated after > I 0 times s e i z u r e . T a b l e 2 s h o w e d n u m b e r o f pre treatment seizure among the subjects. Table 1. Characteristic of patients Characteristic Sex male female Age at onset . <5 years old 5-12 years old > 12 years old Type of convulsive seizure general partial idiopathic epilepsy symptomatic epilepsy Number of pre treatment seizure 510 > 10 EEG recording normal abnormal no data The history of febrile seizure present absent Family history of epilepsy present absence History of status epilepticu present absence t Neurological deficit present absence t N Percentage 47 63 42.7% 57.3% 32 38 40 29.1% 34.5% 36.4% 88 22 65 45 80% 20% 59.1% 40.9% 73 37 66.4% 33.6% 17 81 12 15.5% 73.6% 10.9% 31 79 28.2% 71.9% 13 97 11 3 % 88.2% 12 98 10.9% 89.1% 17 93 15.5% 84.5% Table 2. Number of pre treatment convulsive seizure among the study subjects Number of pre treatment seizure N Percentage 1 times 2 times 3-5 times 6- 10 times > 10 times 20 21 20 12 37 18.2% 19.1% 18.2% 10.9% 33.6% fi'nzon, 3ianon0, Rmd? &ognostic factor of convuhive epilepsy Table 3. The significant predictive factors for 6 months remission Characteristic Type of seizure General tonic clonic Simple partial Complex partial Number of pre-treatment seizure 5 10 > 10 Neurological deficit Absence Presence *RR = Proportion of six months remission RR* (95% CI) P 81.8% 81.8% 45.5% l .OO (0.74 - 1.34) 0.56 (0.29 - 0.87) 0.68 0.013' 84.9% 64.9% 0.76 (0.59 - 0.98) 0.016' 82.8% 52.9% 0.63 (0.405 - 0.92) 0.006. relative risk Six months remission Six months remission during treatment was achieved in 86 patients (78.2%). Table 3 showed the significant predictive factors for achieving 6 months remission. Table 3 showed that complex partial seizure, high number of pretreatment s e i z u r e , and the presence of neurological deficit were significantly poor predictive factors for achieving 6 months remission. Sex, age of onset, origin of epilepsy, history of febrile seizure, history of status epilepticus, family history of epilepsy, compliance of therapeutic program, and, EEG pattern were not significant predictive factors. Twelve months remission The 12 months remission during treatment was achieved in 4 8 (43.6%) patients. Table 4 showed the significant prognostic factors for achieving 12 months remission. Table 4 showed that significant predictive factors for 12 months remission were number of pre treatment seizure, c o morbidity of neurological deficit, and compliance of treatment program. None of the patients with complex partial seizure achieved 1 2 months remission Table 4. The significant predictive factors for 1 2 months remission Characteristic Proportion of 12 months remission RR* (95% CI) P 50.7% 29.7% 0.587 (0.34-0.92) 0.036' 49.5% 1 1.8% 0.238 (0.06-0.889) 0.004. 5 1.4% 30.0% 0.583 (0.345-0.986) 0.029. 50% 36.4% 0% 0.73 (0.32-1.63) NA 0.039 Number of pre-treatment seizure 5 10 > 10 Neurological deficit Absence Presence Compliance of treatment Compliance Incompliance Type of seizure General tonic clonic Simple partial Complex partial * RR = relative risk: NA= not available Table 5. Average of months with positive breakthrough seizure in the first year of anti epileptic treatment Characteristic Mean rt SD P Type of seizure General tonic clonic Simple partial Complex partial Number of pre-treatment seizure 2.81 k 2.78 3.45 k 3.59 6.64 k 3.29 0.00 1' 2.86 k 2.60 4.03 =t3.29 0.0 16' 2 10 > 10 Neurological deficit Presence Absence Compliance of treatment Compliance Non compliance 4.94 k 2.82 2.95 =t3.06 0.014' 2.76 k 3.03 4.13 k 3.07 Breakthrough seizure Breakthrough seizure was defined a s number of month with positive seizure during an anti-epileptic treatment. The average number of breakthrough seizure was significantly higher in patients with partial type of epilepsy, high number pre-treatment seizure, incompliance, and the presence of neurological deficit (Table 5). 0.026' N u m b e r o f pre-treatment seizure a n d the probability for achieving remission The proportion of six months remissions were lower in patients with high number of pretreatment seizure. Similar result was shown in 12 months remission. (Table 6 and Table 7). Table 6. The trends of 6 months remission rate in patients with number of pre-treatment seizure Number of pre-treatment seizure 1 times 2 times 3-5 times 6- 10 times > 10 times Six months remission Yes No 20 (100%) 0 (0%) 17(81%j 4 ( I9%) 18 (90%) 2 (1 0%) 7 (58.3%) 5 (4 1.7%) 24 (64.8%) 13 (35.2%) p (chi square for trend) 0.0 14 Table 7. The trends of 12 months remission rate in patients with number of pre-treatment seizure Number of pre-treatment seizure 1 times 2 times 3-5 'times 6-10 times > 10 times Twelve months remission Yes No 13 (65%) 12 (57.1%) 7 (35%) 5 (4 1.7%) 10 (27%) 7 (35%) 9 (42.9%) 13 (65%) 7 (58.3%) 27 (73%) p (chi square for trend) 0.0079 Prognosticfactor of convuhive epilepsy Bnzon, Xatsono, msd? 1.2 1 0 - 8. .6 - - No of seizure I 4. 2 <I= 10 r - + I ,,,r - J , r: > 10 ,J 00. C-,,,,,d + -2 0 2 a, 8 6 10 12 14 Time of remission (months) Figure 1. The probability of achieving 6 months remission during first year therapy based on the status of pre-treatment seizure Patients with high number of pre-treatment seizure also had significantly lower probability for achieving 6 months remission during the first Year of treatment (Figure 1). Table 8. The multiple logistic regression for not achieving 6 months remission during treatment Prognostic factors High number of pre-treatment seizure Complex partial seizure The presence of neuroloaical deficit B 1.104 1.323 1.440 SE 0.493 1.036 0.578 Exp (B) I OR* 3.017 3.755 4.220 95% CI 1.149 - 7.924 0.811-13.903 1.359 - 13.101 P 0.025' 0.202 0.013* *OR = odds ratio Table 9. The multiple logistic regression analysis for not achieving 12 months remission during treatment Prognostic factors B SE Exp (B) I OR* 95% CI The presence of neurological deficit partial type of epilepsy High number of pre-treatment seizure Non compliance of treatment program *OR = odds ratio 2.086 1.440 0.548 1.071 0.817 0.639 0.465 0.475 8.056 4.222 1.730 2.917 1.623 - 39.975 1.207 - 14.766 0.682 - 4.387 1.173 - 7.257 P 0.01 1' 0.024~ 0.248 0.02 I * Multiple logistic regression analysis Table 8 and 9 showed the significant predictive factors of remission i n multiple logistic regression analysis. The multiple logistic regression analysis showed that high number of pre-treatment seizure and the presence of neurological deficit were the poor prognostic factors for achieving 6 months remission. The presence of neurological deficit, partial type of epilepsy, and non compliance of treatment program were the poor prognostic factors for achieving 12 months remission. aspartate (NMDA) receptor and excitatory input, (ii) the loss of inhibition, and (iii) neuronal reorganization.'") The experimental study showed that recurrent seizure inhibit cell multiplication, inhibited myelin accumulation, and d i s r u p t e d i n t e r cell connection.(18) Glutamate is a very important factor o f neuronal damage, the neuronal damage is primarily mediated by excessive glutamate release, and not because of hypoxic theory.(I9) lThe most vulnerable area of secondary damage through recurrent and prolonged seizure is limbic system. The sprouting and permanent reorganization is primary noted in DISCUSSION mossy fibers synaptic c o n n e ~ t i o n . ( ' ~ There .*~) are 3 hypothesis of the role of mossy fibers: (i) This study showed that high number of t h e damage o f mossy f i b e r s will induce pre-treatment seizure was one of the prognostic sprouting and induce subsequent seizure, (ii) factors in convulsive epilepsy. The role of the damage of mossy fibers will cause hypo number of pre-treatment seizure was based on activity of inhibition function, and (iii) the the theory that prolonged and recurrent seizure survive mossy fibers will change in nature, and caused neuronal damage and development of very excitable and cause sub sequent seizure.(Ig) new epileptic foci. The neuronal damage is Based on the kindling theory, Reynolds(20) mediated by excessive excitatory of amino suggested that anti epileptic drug must be aCid.(10.11.14) prescribed soon for preventing structural S e i z u r e induced s u b s e q u e n t s e i z u r e change due to epilepsy. The prevention of through facilitation phenomenon. This concept development of secondary epileptic foci can known as kindling model of epilepsy. Electrical also be performed by optimal control of seizure. abnormality from primary focus can induce the Poor medication program and seizure control surrounding area and develop paroxysmal will cause chronic and refractory epilepsy.(I6) e l e c t r i c a l a b n o r m a l i t y . ( l O 'T h e p r e v i o u s The result of previous studies were still experimental study showed that the neuronal inconsistent. The prospective study of 479c h a n g e s s u r r o u n d i n g t h e f o c u s w e r e childhood onset epilepsy showed that patients permanent.(IS)Thekindling phenomenon also who exceeded 10 times of pre-treatment seizure observed in experimental s u b convulsive have lower probability of remission rate. The s t i m u l a t i o n . T h e s e n s i t i v i t y o f neuron risk of breakthrough seizure is significantly increased, and there will be permanent declining lower in patients with low number of preof seizure threshold.(g) treatment seizure ( < l o ) (15% vs 52%, RR= T h e process of developing secondary 0.28, p<0.001).(2') Other prospective study epileptic foci also mediated by long term showed that the risk of refractory epilepsy was potentiation mechanism and mirror effect.(I6) significantly higher in patients with > 20 times The steps of development of secondary epileptic pre-treatment seizure (5 1% vs 29%, RR= 1.8, foci were: (i) stimulation o f N-methyl d- p<0.00 There were significant linear trend Prognosticfactor of convulsive epihpsy finzon,Hanono, Kush that high number of pre-treatment seizure was associated with probability of refractory. Other studies did not confirm the role of pre-treatment seizure as prognostic factors. ) Community based study by C o ~ k e r e l l (in~ ~792 epilepsy patients showed that high number of pre-treatment seizure was not associated with poor prognostic factors for 5-year remission. Prospective study in 446 childhood onset epilepsy showed that there was no significant risk difference for achieving remission i n patients with low (<25) and high number of pretreatment seizure ( R R = l . 17, 95% CI=0.791 .76).(24) The clinical implications of this study are that seizure must be recognized soon, and optimal treatment is needed for preventing chronic and intractable epilepsy. Early optimal treatment is also needed for preventing injury, premature death, cognitive impairment, and psychosocial ~ t i g m a . ( ~ ~A. ' ~randomized ) controlled trial compared the risk of recurrent seizure between patients with early therapy (soon after first seizure) and patients with late therapy (after recurrent seizure). The result showed that risk of recurrence in two year period was higher in patients with late therapy (RR= 2.8,95% CI= 1.9-4.2).(") Study by Gilad, et a1.(28)in 87 general tonic clonic epilepsy showed that probability of seizure free was significantly higher (p<O.Ol) in patients with early treatment program. The other significant predictive factors of remission are type of epilepsy, compliance of treatment, and neurological deficit. Partial type of epilepsy, particularly complex partial seizure is associated with poor prognosis.(29)This study failed to show that symptomatic epilepsy had worse prognosis than idiopathic epilepsy. The most reasonable reason was an inadequate diagnosis of symptomatic epilepsy in this study. In most cases diagnosis was only based on history. In childhood onset of epilepsy the good prognostic factors are: ( i ) the absence o f neurological deficit, (ii) normal psychomotor function, (iii) normal IQ, (iv).age of onset > 2 years old, (v) low number of pre-treatment seizure, (vi) normal EEG recording, and (vii) early response to treatment.c30) The compliance of treatment program is also an important factor. Simple and single treatment r e g i m e n t w i l l i m p r o v e t h e compliance.(3')A d e q u a t e c o u n s e l i n g a n d information about long treatment program and the importance of regular medication also enhance the compliance.(32)There are four main factors that enhancing the treatment compliance: (i) support form the physicians, (ii) support form the family, (iii) positive prospective of epilepsy, and (iv) high motivation.(33) CONCLUSIONS Most epilepsy patients achieved 6 months remission with treatment, but only about half of them achieved 12 months remission. High number of pre treatment seizure was one of the significant poor predictive factors for achieving remission. The other prognostic factors were type of epilepsy, incompliance of treatment program, and the presence of neurological deficit. The strongest poor prognostic factors were the presence of neurological deficit. References 1. 2. 3. 4. World Health Report. Epilepsy in the world health report, mental health: new understanding, new hope. Geneva: World Health Organization; 2001. Shafer PO. Improving the quality of life in epilepsy: non medical issues too often overlooked. Postgrad Med Online 2002; 1 1 1: 1. Mills N, Bachmann M, Harvey I, McGrowen M, Hine 1. Patient's experience of epilepsy and health care. Fam Pract 1997; 14: 1 17-23. Meliala L. Aspek psikososial epilepsi. Simposium penatalaksanaan mutakhir epilepsi. Yogyakarta; 1992. Brodie MJ, Dichter MA. Antiepileptic drugs. N Engl J Med 1996; 334: 168-75. Smith D, Chadwick D. The management of epilepsy. J Neurol Neurosurg Psychiatry 2001 ; 70: ii 1 5 4 21. Harsono. Epilepsi. 1" ed. Yogyakarta: Gadjah Mada University Press, 200 1. Dreifuss FE. Prognosis of childhood seizure disorders: present and future. Epilepsia 1994; 35 (suppl2): S30-S4. Sadzot B. Epilepsy: a progressive disease? Br Med J 1997; 314: 91. Morrell F. Secondary epileptogenesis in man. Arch Neurol 1985; 42: 3 18-35. Holmes GL. Epilepsy in the developing brain: lessons fiom the laboratory and clinic. Epilepsia 1997; 38: 12-30. Page RM, Cole GE, Timmreck TC. Basic epidemiological methods and biostatistics. A practical guide book. London: Jones and Bartlet Publisher; 1996. Carpay HA, Arts WFM, Geerts AT, Stroink .H. Epilepsy in childhood: an audit of clinical practice. Arch Neurol 1998; 55: 668-73. Chapman AG. Glutamate and epilepsy, glutamate and glutamine in the brain. J Nutr 2000; 130: 1043s-45s. Holmes GL, Ben-Ari Y. The neurobiology and consequences of epilepsy in developing brain. Pediatr Res 200 1;49: 320-5. Fong GCY. Fong JKY. Recent advances in the diagnosis and management of epilepsy. Hong Kong Med J 2001; 7: 73-84. Browne TR. Holmes GL. Handbook of epilepsy, 2"ded. New York: Lippincott Williams; 2000. Kulkarini SK. George B. Significance on long term potentiation (LTP) in cognitive functions and epilepsy. Indian J Pharmacother 1999; 3 1: 14-22. Lowenstein DH. Alldredge BK. Status epilepticus. N Engl J Med 1998; 338: 970-6. Reynolds EH. Controversies in management: do anticonwlsants alter the natural course of epilepsy? Treatment should be started as early as possible. Br Med J 1995; 3 10: 176-7. Carnfield C, Camfield P, Gordon K, Dooley J. Does the number of seizures before treatment influence ease ofcontrol or remission of childhood epilepsy? not if the number is 10 or less. Neurology 1996; 46: 41-4. Kwan P, Brodie MJ. Early identification of refractory epilepsy. N Engl J Med 2000; 342: 3149. Cockerell OC, Johnson AL, Sander JWAS, Shorvon SD. Prognosis of epilepsy: a review and further analysis ofthe first nine years ofthe british national general practice study of epilepsy. A prospective population based study. Epilepsia 1997; 38: 3 146. Arts WFM, Geerts AT, Brouwer OF, Peters ACB, Stroink H, Donselaar CAV. The early prognosis of epilepsy in childhood: the prediction of poor outcome. The Dutch study of epilepsy in childhood. Epilepsia 1999; 40: 726-34. Sperling MR, Bucurescu G, Kim B. Epilepsy management: issues in medical and surgical treatment. Postgrad Med 1997; 102: 1. Permca E, Beghi E, Dulac 0 , Shorvon S, Tomson T. Assesing risk to benefit ratio in antiepileptic drug therapy. Epilepsy Res 2000; 41: 107-39. Berg AT, Shimar S, Levy SR, Testa FM, Rapaport SS, Beckerman B, et al. Two year remission and subsequent relapse in children with newly diagnosed epilepsy. Epilepsia 200 1; 44: 1553-62. Gilad R,Lamp1 Y, Gabbay V, Eshel Y, Pinhas IS. Early treatment of a single generalized tonic clonic seizure to prevent recurrence. Arch Neurol 1996; 53: 1149-52. Singhvi JP, Sawhney IMS, Lai V, Pathak A, Prabhakar S. Profile of intractable epilepsy in a tertiary refereal centre. Neurol India 2000; 48: 35 16. Placencia JG. Epilepsy in childhood, brain and mind magazine, State University of Campinas, Brazil; 1997. Cavazos JE, Lum F, Spitz M. Seizure and epilepsy: overview and classification. Med J 2002; 4: 3. Beydoun A, Passaro EA. Appropriate use of medications for seizures: guiding principles on the path of efficacy. Postgrad Med 2002; 111: 69-82. Kyngas H. Predictors of good compliance in adolescents with epilepsy. Seizure 2001; 10: 5493.