Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
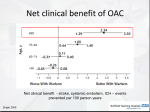
Efficacy and Safety of Apixaban Compared with Warfarin According to Patient Risk of Stroke and Bleeding in Atrial Fibrillation Presented by Renato D. Lopes, MD, PhD, Duke Clinical Research Institute, Duke University, USA for the ARISTOTLE investigators. Disclosures for Renato D. Lopes Institutional research grants from: Bristol-Myers Squibb Advisory board or consultancy for: Boehringer Ingelheim and Bristol-Myers Squibb Background • Warfarin is very effective at preventing stroke in patients with atrial fibrillation (AF), but it has several limitations. • The need to assure optimal benefit given the known bleeding risks of warfarin has led to the development of risk scores for thromboembolism and bleeding in patients with AF. • Scores are important tools to predict the risk of stroke and bleeding in patients with AF and to inform decisions regarding the use of antithrombotic therapy. • The value of these scores in guiding decision making in patients with AF receiving apixaban, a novel oral factor Xa inhibitor, is uncertain. Atrial Fibrillation with at Least One Additional Risk Factor for Stroke Inclusion risk factors Age ≥ 75 years Prior stroke, TIA or SE HF or LVEF ≤ 40% Diabetes mellitus Hypertension Randomize double blind, double dummy (n = 18,201) Exclusion Mechanical prosthetic valve Severe renal insufficiency Need for aspirin plus thienopyridine Apixaban 5 mg oral twice daily Warfarin (2.5 mg BID in selected patients) (target INR 2-3) Warfarin/warfarin placebo adjusted by INR/sham INR based on encrypted point-of-care testing device Primary outcome: stroke or systemic embolism Main Trial Results Stroke or systemic embolism ISTH major bleeding 21% RRR Apixaban 212 patients, 1.27% per year Warfarin 265 patients, 1.60% per year HR 0.79 (95% CI, 0.66–0.95); P=0.011 31% RRR Apixaban 327 patients, 2.13% per year Warfarin 462 patients, 3.09% per year HR 0.69 (95% CI, 0.60–0.80); P<0.001 Median TTR 66% Objectives We conducted this analysis of the ARISTOTLE population to assess the efficacy and safety of apixaban compared with warfarin according to CHADS2 and HAS-BLED scores in patients with AF. • Pre-specified outcomes: – Stroke or systemic embolism (primary efficacy outcome). – ISTH Major bleeding (primary safety outcome). – Mortality. • Post-hoc explored outcomes: – Intracranial bleeding. – Net clinical benefit (the composite of stroke, systemic embolism, major bleeding, and all-cause mortality). Methods The efficacy, safety, and balance of efficacy and safety of apixaban and warfarin were compared across patient risk categories classified by: 1.CHADS2 (low risk: 0-1, medium risk: 2, high risk: ≥3) and 2.HAS-BLED (low risk: 0-1, medium risk: 2, high risk: ≥3) scores. CHADS2 Risk factors History of CHF Hypertension Age ≥75 years Diabetes mellitus Previous stroke, TIA, or systemic embolism HAS-BLED +1 +1 +1 +1 +2 Risk factors Hypertension +1 (systolic BP >160 mm Hg) Abnormal renal function (dialysis, transplant, serum Cr ≥200 +1 µmol/L [2.6 mg/dL]) Abnormal liver function (chronic hepatic disease, bilirubin +1 >2×ULN, AST/ALT/ALP >3×ULN) History of stroke History of bleeding Labile INR +1 +1 +1 (INR <2 or >3 among patients on warfarin before randomization) Elderly (age >65 years) Use of antiplatelets, NSAIDs, or anti-inflammatory medications Drug and/or alcohol abuse +1 +1 +1 Statistical Analysis • Efficacy analyses included all randomized patients (18201 subjects). • The analyses of bleeding events included all patients who received at least one dose of study drug (18140 subjects). • Analyses based on interactions between treatment and categories of CHADS2 and HAS-BLED were performed using a Cox proportional hazards model. Baseline Characteristics CHADS2 0–1 (N=6183) 67·0 (60, 71) 30·3 CHADS2 2 (N=6516) 71·0 (63, 77) 36·1 CHADS2 ≥3 (N=5502) 75·0 (67, 79) 39·7 82·7 17·3 58·1 85·7 14·2 55·6 85·7 14·3 57·9 Age ≥75 yrs 9·3 36·1 50·1 Prior stroke, TIA, or SE 0·6 4·7 58·0 Heart failure or reduced LVEF 8·4 36·0 48·6 Diabetes 3·2 28·0 45·9 Hypertension requiring treatment 77·3 91·7 93·8 Normal >80 mL/min 52·8 40·9 29·0 Mild impairment 38·7 41·1 45·8 Moderate impairment 7·7 16·2 22·0 Severe impairment 0·4 1·3 2·9 Age, yrs, median (25th, 75th) Female, % Type of AF, % Persistent or permanent Paroxysmal Prior use of vitamin K antagonist, % Qualifying risk factors, % Renal function, % Correlation between CHADS2 and HAS-BLED scores HAS-BLED CHADS2 Total 0–1 2 ≥3 0–1 2980 (43) 2142 (32) 1061 (23) 6183 (34) 2 2621 (38) 2549 (38) 1346 (30) 6516 (36) ≥3 1275 (19) 2091 (31) 2136 (47) 5502 (30) Total 6876 (38) 6782 (37) 4543 (25) 18201 (100) Data presented at number (%). Stroke/Systemic Embolism ISTH Major Bleeding Intracranial Bleeding All-cause Mortality Net Clinical Benefit: Stroke, Systemic Embolism, Major Bleeding, or All-cause Mortality Limitations • The absence of patients with CHADS2 score of 0 does not permit an assessment of the benefit / risk profile of apixaban in this low-risk group of patients with AF. • We calculated labile INR based on one single INR value among warfarin-experienced patients at baseline and this is different from how labile INR was initially described (TTR less than 60%). • Our results were derived from a large clinical trial population that differs from an unselected clinical patient population. Conclusion • The benefits of apixaban compared with warfarin in reducing stroke or systemic embolism, all-cause mortality, and causing less bleeding are consistent across AF patients with a wide range of stroke and bleeding risks as assessed by the CHADS2 and HAS-BLED scores. • Patients with AF and at the highest risk of bleeding may have the greatest reduction (both relative and absolute) in intracranial bleeding with apixaban as compared with warfarin. Thank you