Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
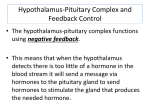
KING SAUD UNIVERSITY NURSING COLLAGE MASTER DEGREE 1431-1432H Nursing management for acute disease in: Respiratory system Endocrine system Hematology system Immunology system Done by : maha alonazi OBJECTIVE At the end of the lecture the master student well be able to : Know the most common of acute respiratory disease . Identify nursing management for RD . Know the most common of acute endocrine disease . Identify nursing management for ED . Know the most common of acute hematology & immunology disease . Identify nursing management for HD & ID . OUTLINE RESPIRATORY DISEASE : Anatomy of respiratory system . Croup. Acute epiglottitis Broncholitis . Pneumonia. Aspiration pneumonia . ARDS Asthma. ENDOCRINE DISEASE : Anatomy of endocrine system . Diabetes Mellitus Diabetic ketoacidosis . Diabetes Insipidus. SIADH . Hyperthyroidism. Hypothyroidism. Gigantism HEMATOLOGY & IMMUNOLOGY DISEASE : Anatomy of immune & hemato system . Anemia Sickle cell disease DIC Hemophilia Leuckemia Thalasmia ANATOMY OF RESPIRATORY SYSTEM Upper airway . Lower airway . Thoracic cavity . UPPER AIRWAY Ideally above larynx is the upper airway Practically speaking Nose, Larynx (Glottic opening and vocal cords) and trachea (Up to Carina). The upper airway is responsible for warming, humidifying and filtering air before it reaches the trachea. Nose Pharynx Larynx LOWER AIRWAY (LUNG) Trachea Lung Conducting Airways Gas exchange units (Alveoli) THORACIC CAVITY Diaphragm The chest wall SPECTRUM OF RESP. DISEASES Upper AW - Stridor, croup, laryngomalacia Lower AW - Asthma, bronchiolitis Lung Parenchymal edema Pleural - - Pneumonia, Pulmonary Empyema, Pneumothorax 12 WHEN WILL YOU SUSPECT UAW DIS.? Stridor Neck retraction Suprasternal retraction Sniffing position 13 ACUTE LARYNGOTRACHEOBRONCHITIS (CROUP) Definition : inflammatory swelling of the submucosa in the subglottic area & trachea ,bronchi ,bronchioles Commonest cause of acute stridor usually occure for child from age 3 month to 5 yrs . causes : Viruses: Parainfluenza. RSV . Sing & symptoms: barking cough. Hoarseness. stridor. Low fever. 14 (CROUP) MANAGEMENT Mild: Stridor at rest, cough Minimal handling Moderate to severe: Stridor at rest. Racemic epinephrine nebulization Dexamethazone IV or IM, also oral or Nebulized Budesonide Severe: Impending respiratory failure Intubation for 2-3 days. Improves in a week. Majority may not need intubation 15 X-ray Neck in croup Sharpened pencil appearance 16 NURSING MANAGEMENT provide medication as order . Provide cool & humidified oxygen as needed Check vital sign . Monitor pulse oximetry. Minimal handling. Provide quit environment . Enteral feeding may be considered in pt. with respiratory distress . Acute epiglottitis Definition :Is severe life threatening rapidly progressive infection of the epiglottis &aryepiglottic folds & surrounding tissue . Usually occurs in children aged 2-6 yrs but can occurs any any age. Caused: before the use of the HiB vaccine ( haemophilus influanzae type B) was the moust commonly identified cause of acute epiglotittis ,the usual cause in the vaccinated child is now streptococcus pyogenes, S.pneumoniae ,or staphylococcus aureus . Sing & symptom : Sudden onset of high fever. dysphagia. drooling,. muffled voice. soft stridor. inspiratory retractions. Normal Lateral neck 20 ACUTE EPIGLOTTITIS - MANAGEMENT Intubation by a skilled person IV Ceftriaxone O2 and other supportive management Usually extubatable in 3-4 days Antibiotics for 10 days. 21 NURSING MANAGEMENT Close monitoring . Arm restraint to prevent self extubation . Decreased movement of the ETT in the larynx . Deliver oxygen as necessary . CROUP EPIGLOTTITIS Age: Younger infants No fever Harsh stridor Parainfuenza virus Usually no antibiotics, no intubation Age: older children High fever, toxic Soft stridor, Drooling, muffled H influenza(Bacteria) Needs antibiotics and intubation 23 DO AND DON’T IN UAW DIS. Allow the patient in his position of comfort Do not separate the child from mother Do not force the child to lie down Do not make the child cry? Do not send the child for X-ray without accompanied by medical team Continuously monitor for the need for intubation. 24 BRONCHOLITIS Definition : acute inflammatory disease of the lower tract that result in obstruction of small airways . Causeas : viral infection . Sing & symptom : Cough. Wheezing . Prolong expiration. Irritability . Low grade fever . Tachypnea . Retraction . NURSING MANAGEMENT Maintained fluid & nutritional requirement Monitor child closely for respiratory failure. provide medication as order . Provide oxygen as needed or M.V if respiratory failure ,hypoxemia or apnea are developed . Check vital sign . Monitor pulse oximetry Prevent nosocomial infection by good HW. PNEUMONIA Pneumonia is infection of the lung caused most often by bacteria or viruses . Mode of transmission: 1-Inspiration. 2-Aspiration. 3-Circulation. Bypass of nasal defense Pulmonary aspiration (CNS, GER, TEF) Abnormal secretions or mucociliary clearance Underling chronic disease/nutrition Defect in the immune system Sign & symptom : Chills, fever and cough Stuffy nose Irritability Resp distress: expiratory grunting, nasoflaring, retraction, tachypnea, tachycardia. Cyanosis, air hunger, and occasionally apnea NURSING MANAGEMENT Monitor V\S ,ABG level ,oxygen saturation . Administered nebulization & oxygen at concentration as prescribed . Placed in high fowler position . Rendered chest physiotherapy . Encourage pt. to deep breathing & cough . Encourage pt. to increased fluid intake to liquefy secretion . Assess lung sound . Administered antibiotic as ordered . Avoid contact with people with URTI . ASPIRATION PNEUMONIA Definition :inflammation caused by pulmonary aspiration of gastric fluid produced direct injury to the mucosal surface of the respiratory tract . Causes :see table Sing & symptom : Cough ,fever . acute dyspnea. wheezing , crackles or absent breathing sound in the effected lobes , cyanosis, retraction , tachypnea . CAUSES OF ASPIRATION PNEUMONIA Altered level of consciousness Drugs, alcohol, anesthesia, seizures, CNS disorders Altered anatomy or function of trachea or esophagus Traceal or esophageal abnormalities, ETT, tracheostomy Altered function of swallow or esophageal motility Loss of normal reflexes which prevent aspiration of stomach contents, GER (worse with neuro or anatomical impairment) Inhalation injury Inhalation of toxic substances NURSING MANAGEMENT Monitor V\S ,ABG level ,oxygen saturation . Administered nebulization & oxygen at concentration as prescribed . Placed in high fowler position . Rendered chest physiotherapy . Encourage pt. to deep breathing & cough . Encourage pt. to increased fluid intake to liquefy secretion . Assess lung sound . Administered antibiotic as ordered . ARDS Definition :acute lung injury & noncardiogenic pulmonary edema . Causes : Gastric aspiration. Toxic inhalation . Pulmonary infection . FBA . Sing & symptom : Stage 1 :(1-2 day) : mild tachypnea, hypoxemia,anxiety or restlessness. Stage2 :(2-3 day) :cyanosis in room air ,tachycardia,retraction . Stage 3:(3-10 day ):symptom change from distress to failure (inability to oxygenate & ventilate,alveolar collapse desaturation ,high oxygen requirement . Stage 4 : (after 10 day ):development of pulmonary fibrosis & progressive impairment of oxygenation are observed . NURSING MANAGEMENT Encourage coughing & deep breathing in awake pt. Frequent position change with CPT as needed . Reduce abdominal distention by NGT if necessary . Check vital sign . Monitor pulse oximetry . Do VBG & ABG analysis . Provide supplemental oxygen for pt. with adequate ventilation . Provide medication such as sedative ,analgesic ,neuromuscular blocking agents ,bronchodilator as ordered . Provide high calories & high protein diet. ASTHMA (CHRONIC DISEASE ) Definition :obstructive pulmonary disease characterized by airway inflammation with mucosal edema,thick secretion that cause plugging & hyperreactivity of the tracheobronchial tree that result in bronchospasm of the smooth muscle . Causes :inflamatory mediators are thought to stimulate the vagus nerve ( cholinergic stimulation )causing smooth muscle constriction & increased production of mucus. Sing & symptom: Tachycardia. Tachypnea. Cynosis. Expiratory wheezing in severe case. Inspiratory & expiratory wheezing . Hypoxemia . NURSING MANAGEMENT Monitor pattern of breathing & V\S at regular interval . Assess S & S of respiratory distress . Administer oxygen & nebulization as indicated . Assess lung sound . Monitor pulse oximetry & ABG level as indicated . Encourage rest in between activity to prevent fatigue & encourage deep breathing . 1- Endocrine glands : secrete hormones directly into the bloodstream ( adrenal , pancreas ,thyroid glands) 2-Exocrine glands :secrete biochemical substances that are released into ducts to be delivered to target organs ( salivary ,sweat glands ) Major glands : 1-Hypothalamus-pituitary complex .(ACTH,TSH,ADH,Oxytocin ) 2-Thyroid gland.(T3,T4) 3-Parathyroid gland.(PTH) 4-Adrenal gland.(sex hor. Cortisol,epinephrine,norepinephrine ) 5-Islets of langerhans in the pancreas.insullinbeta cell, glucagon-alpha cell, somatostatin-delta cells 6-Gonads.estrogen,progesterone,testosterone . FIG 1. PITUITARY HORMONES AND THEIR TARGET ORGANS. DIABETES MELLITUS Definitions Type I: Insulin-dependent mellitus (IDDM) It is autoimmune disease that result in the T-cell-mediated destruction of the beta pancreatic cells .it is the most common form of diabetes in infants & children & requires insulin replacement therapy . Type II: Non-insulin-dependent diabetes mellitus (NIDDM) Is associated with obesity ,strong family history & older age .it is not autoimmune process but instead due to insulin resistance enough insulin is produced to prevent ketoacidosis. it can treated by oral hypoglycemia agents , diet.exercise . DIABETES MELLITUS Diabetic ketoacidosis Is the absence of insulin & cellular uptake of glucose is inhibited & glucose production by the liver is increased & glucose utilization decreased resulting in hyperglycemia . Etiology : is related to inadequate endogenous insulin secretion . Acute stress, infection ,trauma , high dose of steroide . TABLE 1. SIGNS AND SYMPTOMS Symptoms Hyperglycemia Metabolic acidosis (gap acidosis) Dehydration, shock Kussmaul breathing Cardiac arrhythmia Sodium imbalance Potassium imbalance Mental status changes Hyperosmolality Ketonuria Glucosuria Management Fluid Electrolytes Insulin Monitoring NURSING MANAGEMENT Monitor V\S & blood sugar level . Provide 3 regular diabetic meals with in between snacks as tolerated . Check weight daily \weekly as indicated . Observed for circulation on feet . Monitor intake & output . Check urine for protein & ketones . Monitor S\S of hypo & hyperglycemia . Administered insulin regimen as prescribed . TABLE 3. CLINICAL OBSERVATION IN DEHYDRATION Examination Dehydration Skin turgor Skin (touch) Buccal mucosa/lips Eyes Tears Fontanelle CNS Pulse rate Pulse quality Capillary refill Urine output Older Child: 3% (30mL/kg) 6% (60mL/kg) 9% (90mL/kg) Infant 5% (50mL/kg) 10% (10mL/kg) 15% (150mL/kg) Mild Normal Normal Moist Normal Present Flat Consolable Normal Normal Normal Normal Moderate Tenting Dry Dry Deep set Reduced Soft Irritable Slightly increased Weak =2 sec Decreased Severe None Clammy Parched/cracked Sunken None Sunken Lethargic/obtunded Increased Feeble/impalpable >3 sec Anuric TABLE 4. INSULIN PREPARATION Insulin Onset (hr) Rapid acting NovoLog Humalog 0.17-0.33 0.25-0.5 Short acting Regular 0.5-1 Intermediate acting NPH Lente Long acting Ultralente Basal Lantus 1-4 1-4 4-10 5 Peak (hr) Duration (hr) 1-3 0.5-1.5 3-5 6-8 1-5 3-10 4-14 4-14 10-24 12-24+ 8-30 18-36 No pronounced peak 20-24+ SYNDROME OF INAPPROPRIATE ANTIDIURETIC HORMONE Characterized by inappropriate, excessive secretion of ADH Occurs in the face of low serum Na and low serum osmolality Clinical signs and symptoms are secondary to increased blood volume and hyponatremia. PATHOPHYSIOLOGY OF SIADH ETIOLOGY AND RISK FACTORS Conditions associated with SIADH Meningitis, Head trauma, Cerebral tumors, Cerebral hemorrhage, Chornically ill or malnourished, Spinal surgery SIGNS AND SYMPTOMS Low urine output and the absence of hypovolemia Headache, confusion, lethargy, altered LOC, coma or seizures Nausea and vomiting Weight gain Filling pressures (normal or increase) Hypertension and tachycardia MANAGEMENT Serum sodium: normalized over 24 to 48 hours Monitoring: intake & output , specific gravity, serum electrolytes and osmolality, & daily weights. NURSING MANAGEMENT Monitor intake & output Monitor specific gravity. Monitor serum electrolytes and osmolality daily weights. DIABETES INSIPIDUS Characterized by a decrease in both urine concentrating ability and water conservation. Types of DI Central Common form in children and critical care environment, deficiency of ADH due to failure of the hypothalamus to synthesize or failure of the posterior pituitary to secrete or both . Nephrogenic Characterized by normal secretion of ADH by the posterior pituitary but the distal tubule & collecting ducts in the kidney are resistant to the effects of ADH . DIABETES INSIPIDUS Etiologyy : Central Pituitary and head trauma, CNS infections, cerebral edema, cerebral hemorrhage or infarct, congenital, familial, idiopathic Nephrogenic Chronic renal disease, polycystic kidney disease, pregnancy, starvation SIGNS AND SYMPTOMS Large quantity of dilute urine Hypernatremia Serum hyperosmolality Polyuria Urine osmolality Polydipsia Signs of dehydration Altered mental status DIABETES INSIPIDUS Management Central Use fluid or ADH replacement therapy Nephrogenic Difficult to treat, Sodium-restricted diet NURSING MANAGEMENT Monitor intake and output. Daily weights. Frequent hemodynamic. Neurologic assessments. Assess signs of dehydration. Assess urine & electrolytes result . Monitor specific gravity. DIFFERENTIATION BETWEEN DI AND SIADH DI SIADH Serum sodium >145 mEq/L <135 mEq/L Urine sodium Low High Serum osmolality >300 mOsm/kg <275 mOsm/kg Urine osmolality <300 mOsm/L >800mOsm/L <1.005 >1.020 High Low Urine specific gravity Urine output THYROID GLAND It is the largest endocrine gland. It lies in front of the neck; it is formed two lobes connected by an isthmus which crosses the trachea. THYROID GLAND The thyroid gland secretes the following hormones: 1-Thyroxine (tetraiodothyronine = T4) and (triiodothyronine, = T3) both hormones are iodine containing amino acid. 2-Calcitonin: it is a calcium lowering hormone, polyeptide in nature, secreted from parafollicular cells of thyroid gland. It lowers the plasma calcium level. Actions of T4 and T3: Increase oxygen consumption and enhances the metabolism of all the body tissues. Increase protein synthesis in the kidney, muscle and liver. They stimulate growth. They increase activity of most of enzymes in the cells. Increase the rate of glucose absorption, uptake, and utilization by tissues. Increase the metabolism of fat from its stores and use its fat for production of energy and it decreases the level of plasma cholesterol. Accelerates the heart rate and it is an erythropoietic factor. It increases appetite, the motility and secretions of gastro – intestinal tract. Are important for normal development and maturation of Central Nervous System. HYPERTHYROIDISM Hyperthyroidism(Grave’s disease): Overactivity of the Thyroid Gland, In healthy people, the thyroid makes just the right amounts of two hormones, T4 and T3. Hyperthyroidism is a condition caused by the effects of too much thyroid hormone on tissues of the body. CAUSES There are several causes of hyperthyroidism. Most often, the entire gland is overproducing thyroid hormone. This is called Graves' disease. Less commonly, a single nodule is responsible for the excess hormone secretion. We call this a "hot" nodule. Thyroiditis (inflammation of the thyroid) can also cause hyperthyroidism. SYMPTOMS AND SIGNS Palpitations Heat intolerance Nervousness Insomnia Breathlessness Increased bowel movements Light or absent menstrual periods Fatigue Fast heart rate Trembling hands Weight loss Muscle weakness Warm moist skin Hair loss Enlargement of the thyroid gland (goiter). Protrusion of the eye balls due to excessive growth and degeneration of tissues behind the eye. TREATMENT Anti-thyroid Drugs Radioactive Iodine Treatment Surgical Removal of the Gland or Nodule NURSING MANAGEMENT Monitor V\S . Assess skin turgor & mucous membrane for signs of fluid deficit . Monitor intake & output . Monitor weight daily . Provide high calorie food . Provide quiet ,calm ,cool environment Inspected skin frequently HYPOTHYROIDISM condition leading to the deficiency in the production of thyroid hormone. Iodine deficiency is the most common cause of hypothyroidism worldwide but it can be caused by any number of other causes such as several conditions of the the thyroid gland, or less commonly, the pituitary gland or hypothalamus. Before Puberty (cretinism): Mal development or complete absence of gland in a new born gives the signs and symptoms of cretinism at the age of about 6 months when the mother’s milk becomes deficient in thyroxin, it is characterized by: Mental retardation due to defective of nerve fibers, which lead to delayed mile stones as (sitting walking and speech). Retarded growth, the height is less than one meter. Intolerance to cold weather and decrease BMR. Abdominal muscle weakness, with protruded viscera and protruded enlarged tongue. Infantile sexual organs. Thick skin. Raised serum cholesterol level. After Puberty Myxoedema: This due to atrophy of the thyroid glands or due to thyroidectomy for any reason. It is characterized by: Slow mental activity. Increase sensitivity to cold, the BMR decreased (30 to 40). The hair is coarse and sparse, dry skin, firm non pitting oedema. Sexual hypo function in female, there is irregular cycle, in male there is impotence. Loss of appetite and decrease motility of the gastrointestinal tract which leads to constipation. Deficient erythropoiesis leading to anaemia. SING & SYMPTOM Fatigue. Cold intolerance increased sensitivity to cold Constipation Depression. muscle cramps and joint pain Thin, brittle fingernails Coarse hair Decreased sweating Dry, itchy skin Weight gain and water retention Bradycardia. Thinning of the outer third of the eyebrows (sign of Hertoghe). Abnormal menstrual cycles. CAUSES Iodine deficiency is the most common cause of hypothyroidism worldwideor a deficiency in stimulating hormones from the hypothalamus or pituitary. Congenital hypothyroidism is very rare accounting for approximately 0.2‰ Hypothyroidism can result from postpartum thyroiditis, a condition that affects about 5% of all women within a year of giving birth. Hypothyroidism can also result from sporadic inheritance, sometimes autosomal recessive. CLASSIFICATION Primary: Thyroid gland: The most common forms include Hashimoto's thyroiditis (an autoimmune disease) and radioiodine therapy for hyperthyroidism. Secondary: Pituitary gland: Occurs if the pituitary gland does not create enough thyroidstimulating hormone (TSH) to induce the thyroid gland to produce enough thyroxine and triiodothyronine. Although not every case of secondary hypothyroidism has a clear-cut cause, it is usually caused by damage to the pituitary gland, as by a tumor, radiation, or surgery.[Secondary hypothyroidism accounts for less than 5% or 10% of hypothyroidism cases. Tertiary: Hypothalamus: Results when the hypothalamus fails to produce sufficient thyrotropin-releasing hormone (TRH). TRH prompts the pituitary gland to produce thyroidstimulating hormone (TSH). Hence may also be termed hypothalamic-pituitary-axis hypothyroidism. It accounts for less than 5% of hypothyroidism cases. TREATMENT Hypothyroidism is treated with the levorotatory forms of thyroxine (levothyroxine) (L-T4) and triiodothyronine (liothyronine) (L-T3). NURSING MANAGEMENT Monitor vital signs . Monitor ECG tracing to detect arrhythmias . Provide warm environment. Provide high fiber diet . Administered prescribed stool softener . Administered medication as prescribed . Encourage increase intake of fluids . Provided warm drink . GROWTH HORMONE (SOMATOTROPIN) HGH is synthesized and secreted from the anterior pituitary gland Effects of growth hormone on the tissues of the body can generally be described as anabolic (building up). In addition to increasing height in children and adolescents, growth hormone has many other effects on the body: Increases calcium retention, and strengthens and increases the mineralization of bone Increases muscle mass through sarcomere hyperplasia Promotes lipolysis Increases protein synthesis Stimulates the growth of all internal organs excluding the brain Plays a role in homeostasis Reduces liver uptake of glucose Promotes gluconeogenesis in the liver Contributes to the maintenance and function of pancreatic islets Stimulates the immune system High levels of growth hormone may indicate: Acromegaly Gigantism Growth hormone resistance Pituitary tumor. Low levels of growth hormone may indicate: Growth hormone deficiency. Hypopituitarism. EXCESSIVE GROWTH HORMONE SECRETION Gigantism is the result of excessive growth hormone secretion that begins in young children or adolescents. It is a very rare disorder, usually resulting from a tumor of somatotropes. One of the most famous giants was a man named Robert Wadlow. He weighed 8.5 pounds at birth, but by 5 years of age was 105 pounds and 5 feet 4 inches tall. Robert reached an adult weight of 490 pounds and 8 feet 11 inches in height. He died at age 22. Acromegaly results from excessive secretion of growth hormone in adults. GROWTH HORMONE DEFICIENCY The effects of growth hormone deficiency vary depending on the age at which they occur. In children, growth failure and short stature are the major manifestations of GH deficiency, with common causes including genetic conditions and congenital malformations. It can also cause delayed sexual maturity. Dwarfism: It is deficiency of growth hormone in young age. The rate of development is decreased so the child who has reached the age of 10 years has the body of 4 years. The dwarf is short and mentally normal. TREATMENT For excessive secration : drugs like octreotide (somatostatin agonist) and bromocriptine (dopamine agonist) can be used to block GH secretion because both somatostatin and dopamine negatively inhibit GHRH-mediated GH release from the anterior pituitary. For deficiency: injection of GH. NURSING MANAGEMENT provide medication as order . Measure weight & height . Check weight daily \weekly as indicated . Assess GH level . Educate pt. & family about the important of follow up . ADRENAL GLAND DYSFUNCTION Hypo function of adrenal cortex: (Addison disease): It is due to adrenal cortical insufficiency. It is characterized by: Loss of appetite, vomiting, and diarrhea i.e. gastro intestinal disturbances. Muscle weakness due to decrease of anabolic effect of androgens. Decrease sodium and increase potassium in the blood. (Water moves intracellular, ----- the blood volume decreases and hypotension occur. Hypoglycemia. Decrease sexual function. The Bronze hyper pigmentation of the skin due to high level of ACTH secondary to low level of glucocorticoids. ACTH has melanocytic stimulating activity. CUSHING'S SYNDROME Cushing's syndrome is a hormone disorder caused by high levels of cortisol in the blood. This pathology was described by Harvey Cushing in 1932.[The syndrome is also called Itsenko-Cushing syndrome, hyperadrenocorticism or hypercorticism) Hyper function of Adrenal Cortex (Cushing's Syndrome): It is characterized by: Wasting and weakness of muscle, (catabolic effect). Increase sodium and water retention in the blood (leading to oedema and hypertension with decrease level of plasma potassium). Redistribution of fat, the extremities are thin, there are accumulation of fat in the abdominal wall, face (MOON) and the upper back (buffalo trunk). Hyperglycemia. Gonadal disturbances. The skin is thin. the hypothalamus releases corticotropinreleasing hormone (CRH), which stimulates the pituitary gland to release adrenocorticotropin (ACTH). ACTH travels via the blood to the adrenal gland, where it stimulates the release of cortisol. Cortisol is secreted by the cortex of the adrenal gland from a region called the zona fasciculata in response to ACTH. Elevated levels of cortisol exert negative feedback on the pituitary, which decreases the amount of ACTH released from the pituitary gland. Strictly, Cushing's syndrome refers to excess cortisol of any etiology. One of the causes of Cushing's syndrome is a cortisol secreting adenoma in the cortex of the adrenal gland. The adenoma causes cortisol levels in the blood to be very high, and negative feedback on the pituitary from the high cortisol levels causes ACTH levels to be very low. Cushing's disease refers only to hypercortisolism secondary to excess production of ACTH from a corticotrophic pituitary adenoma. This causes the blood ACTH levels to be elevated along with cortisol from the adrenal gland. The ACTH levels remain high because a tumor causes the pituitary to be unresponsive to negative feedback from high cortisol levels. Cushing's Syndrome was also the first autoimmune disease identified in humans. CAUSES : Exogenous vs. endogenous Hormones that come from outside the body are called exogenous. hormones that come from within the body are called endogenous. The most common cause of Cushing's syndrome is exogenous administration of glucocorticoids prescribed by a health care practitioner to treat other diseases (called iatrogenic Cushing's syndrome). This can be an effect of steroid treatment of a variety of disorders such as asthma and rheumatoid arthritis, or in immunosuppression after an organ transplant. Administration of synthetic ACTH is also possible, but ACTH is less often prescribed due to cost and lesser utility. Endogenous Cushing's syndrome results from some derangement of the body's own system of secreting cortisol. Normally, ACTH is released from the pituitary gland when necessary to stimulate the release of cortisol from the adrenal glands. In pituitary Cushing's, a benign pituitary adenoma secretes ACTH. This is also known as Cushing's disease and is responsible for 70% of endogenous Cushing's syndrome. In adrenal Cushing's, excess cortisol is produced by adrenal gland tumors, hyperplastic adrenal glands, or adrenal glands with nodular adrenal hyperplasia. Finally, tumors outside the normal pituitaryadrenal system can produce ACTH that affects the adrenal glands. This final etiology is called ectopic or paraneoplastic Cushing's syndrome and is seen in diseases like small cell lung cancer . SING & SYMPTOM rapid weight gain particularly of the trunk and face "moon face “ with sparing of the limbs (central obesity ). A common sign is the growth of fat pads along the collar bone and on the back of the neck (buffalo hump) . Other symptoms include hyperhidrosis (excess sweating),. Telangiectasia (dilation of capillaries). Thinning of the skin (which causes easy bruising and dryness particularly the hands and other mucous membranes, purple or red striae (the weight gain in Cushing's syndrome stretches the skin, which is thin and weakened, causing it to hemorrhage) on the trunk, buttocks, arms, legs or breasts, proximal muscle weakness (hips, shoulders). Hirsutism (facial male-pattern hair growth). Baldness and/or cause hair to become extremely dry and brittle. In rare cases, Cushing's can cause hypercalcemia which can lead to skin necrosis (osteoporosis ). The excess cortisol may also affect other endocrine systems and cause, for example, diabetes mellitus menstrual disorders such as amenorrhea in women and decreased fertility in men infertility due to elevations in androgens. signs include polyuria (and accompanying polydipsia), persistent hypertension (due to cortisol's enhancement of epinephrine's vasoconstrictive effect) and insulin resistance (especially common in ACTH production), leading to hyperglycemia (high blood sugar) and insulin resistance which can lead to diabetes mellitus. Patients frequently suffer various psychological disturbances, for example, euphoria , depression and anxiety. Haematology and Immunology Cell differentiation from stem cells Anatomy and Physiology 1- Red blood cells (RBCs, erythrocytes): Develop from erythroid precursor cells Reticulocytes represent the stage of maturation Mature RBCs have a life span of 120 days Hemoglobin: large, complex, iron-containing protein. Responsible for the RBCs oxygen-carrying abilities. RBC: transport oxygen from the lungs to the tissues Hgb A, normal adult hemoglobin Hemoglobin F ( fetal Hgb) present in large concentrations in the fetus, decrease after birth and minimally present in children and adults. Normal RBC production requires iron, folic acid and Vit B12. THE IMMUNE SYSTEM 2-Leukocytes (white blood cells) group that serve to protect the organism. Neutrophils: the largest component of total circulating WBCs, 60 – 70%. Originate and mature in bone marrow Polymorphonucleated (PMNs or poly): mature form of neutrophil Band: unsegmented – appearing nucleus Neutrophilia: increased number of circulating neutrophils Anatomy Neutropenia: decreased number of circulating neutrophils (<1500/mm3) WBCs mature in bone marrow for 10 days Eosinophils: 2 – 5% of the circulating WBC. Eosinophilia: increased number of eosinophils Eosinopenia: decreased number of eosinophils Basophils: smallest portion of granulocytes, 1% of WBC Basophilia increased number of circulating basophils Basopenia decreased number of circulating basophils Mononuclear phagocytes Monocytes 3 – 8% of circulating WBCs Monocytosis increase in the number of circulating monocytes Monocytopenia decrease in the number of circulating monocytes Macrophages: have long life span. Lymphocytes (lymphoid lineage): primary immune cells Lymphocytes: 10 – 40% of the ciculating WBCs Lymphocytosis: increase number of circulating lymphocytes Lymphopenia: decrease in number of circulating lymphocytes T lymphocytes or T cells: 65 – 85% of all lymphocytes Clusters of differentiation (CD) Helper T cells (CD4) Suppressor T cells (CD8) Cytotoxic or killer T cells (CD8) Lymph nodes of the body Anatomy B Lymphocytes or B cells: constitute up to 35% NK cells constitute 5 – 8% of the total lymphocyte count Memory cells – have CD. Programmed to recognize the original invading microorganism on subsequent invasions. WBC Functions Defense: protect the body’s internal environment from “nonself” antigens or microorganisms invasion. Assists the immune system in discriminating “self” from “nonself” or “altered self” Second line of defense: involves the inflammatory response, phagocytosis . 3-Platelets (thrombocytes) 1. 2. Megakaryoblasts: mature into megakaryocytes Characteristics: minute, round or oval discs. Platelet count: 150, 000 to 400, 000/mm3. Maintain normal hemostasis & vascular integrity when a blood vessel wall is injured. Anatomy 4-Plasma factors: 1. Procoagulants: aka plasma clotting factors. Promotes coagulation. 2. Anticoagulants: inhibit coagulation Circulating anticoagulants: antithrombin III, protein C, protein S 3. Coagulation: depends on the balance between the procoagulants and the anticoagulants Nomenclature for coagulation factors Factor Synonym I Fibrinogen II Prothrombin III Tissue thromboplastin IV Calcium V Proaccelerin VI Not assigned VII Proconvertin VIII Antihemophilic factor (AHF|) IX Plasma thromboplastin component (Christmas factor X Stuart factor (Stuart-Prower factor) XI Plasma thromboplastin antecedent (PTA) XII Hageman factor XIII Fibrin-stabilizing factor (FSF) ANEMIA Anemia is defined as a reduction below normal in the volume of red blood cells volume or hemoglobin concentration. Classification of Anemias Anemias can be classified by two approaches: Etiologic factors. Morphologic factors. I. Etiologic Factors: Anemias resulting from impaired or decreased production: The production of the RBCs and Hb can be impaired by: Nutritional deficiency (e.g.folate, iron, B12). Bone marrow failure (e.g. irradiation, malignancy). Interference with bone marrow activity (e.g. infection, chronic diseases). Anemias resulting from accelerated destruction of RBCs (Hemolytic): There are causes that can shorten the life span of the cell, which can be: Corpuscular Causes: Defect in cell membrane: Hereditary erythrocytosis. Defect in cell enzyme: G6PD deficiency. Defect in cell hemoglobin: Sickle cell anemia, Thalassemia. Extracorpuscular causes: Immune: blood transfusion. Non- immune: - burns. - Snake venoms. Anemias resulting from excessive blood loss: Acute blood loss: (bleeding) Alteration in vital signs doesn’t occur unless 20% or more of blood lost occur. Shock occurs with losses of 40% of blood volume. Chronic blood loss: (occult bleeding, Ancylostoma) II. Morphologic Factors: The characteristic changes in RBCs’ size, shape, color is described as below: Cell size: for example, normocytes (normal), microcytes (smaller than normal), or macrocytes (larger than normal). Shape- irregularly shape RBCs; for example, poikilocytes (irregularly shaped cell), spherocytes (globular cells), and drepanocytes (sickle cells). Staining characteristics or color: Reflects the hemoglobin concentration; for example, normochromic (Sufficient or normal amount) or hypochromic (reduced amount). SING & SYMPTOM General Manifestation: Dyspnea on exersion. Muscle weakness. Easy fatigability. Frequent resting. Shortness of breath. Poor sucking (infants). Pale skin: waxy pallor seen in severe anemia. Tachycardia. Cardiac dilatation gradually develops. Central nervous system manifestations: Headache. Dizziness. Night headache. Irritability. Slowed thought processes. Decreased attention span. Apathy. Depression. Shock [blood loss anemia]: Poor peripheral perfusion. Skin is moist and cool. Low blood pressure. Increased heart rate. Anemias Caused by Defect in Hemoglobin Formation Sickle cell anemia (SCA). Thalassemia. SICKLE CELL ANEMIA This disorder is characterized by severe chronic hemolytic disease resulting from premature destruction of the brittle poorly deformable erythrocytes. In which normal adult hemoglobin A (Hgb A) is partly or completely replaced by abnormal sickle hemoglobin (Hgb S). It is a genetically determined (autosomal reccesive) disease. SICKLE CELL ANEMIA sickle cell anemia, the number of red blood cells is low because sickle cells don't last very long. Sickle cells usually die after only about 10 to 20 days. The bone marrow can't make new red blood cells fast enough to replace the dying ones. Normal red blood cells are disc-shaped and look like doughnuts without holes in the center. They move easily through your blood vessels. Red blood cells contain an iron-rich protein called hemoglobin. This protein carries oxygen from the lungs to the rest of the body. Sickle cells contain abnormal hemoglobin called sickle hemoglobin or hemoglobin S. Sickle hemoglobin causes the cells to develop a sickle, or crescent shape. Sickle cells are stiff and sticky. They tend to block blood flow in the blood vessels of the limbs and organs. Blocked blood flow can cause pain, serious infections, and organ damage. CAUSES : Sickle cell anemia is inherited from both parents. Sickle cell disease is much more common in people of African and Mediterranean descent. It is also seen in people from South and Central America, the Caribbean, and the Middle East. Someone who inherits the hemoglobin S gene from one parent and normal hemoglobin (A) from the other parent will have sickle cell trait. People with sickle cell trait do not have the symptoms of true sickle cell anemia. SING & SYMPTOM : Severe sudden chest pain . Splenomegaly in the young children . Impaied growth & development . Attacks of abdominal pain. Bone pain. Breathlessness. Delayed puberty. Fatigue. Fever. Paleness. Rapid heart rate. Ulcers. on the lower legs (in adolescents and adults). Yellowing of the eyes and skin (jaundice). The main objectives of medical treatment are: Bed rest to minimize energy expenditure and oxygen use. Hydration through oral and intravenous therapy. Electrolyte replacement. Analgesics for severe abdominal and joint pain. Blood replacement to treat anemia. Antibiotics to treat any existing infection. NURSING MANAGEMENT Administer blood products as ordered . Improve oxygenation . Prevent iatrogenic anemia . Provide adequate nutrition with high iron . Administered iron replacement as ordered . Monitor vital signs . Assess pt. for palpitation , SOB, dizziness. Administered parenteral vitamin B12 as prescribed . Assess knowledge of present condition .reinforced importance of therapeutic home management & OPD follow up . Assessed dietary intake . Provided diet high in iron . Advised to rest in between activities . Assessed level of fatigue , sleeping pattern , and activity that causes fatigue To reduce sickle cell crises, take the following precautions: To prevent oxygen loss, avoid: Demanding physical activity (especially if the spleen is enlarged) Emotional stress Environments with low oxygen (high altitudes, nonpressurized airplane flights) Smoking Known sources of infection To make sure you're getting enough fluids: Avoid too much exposure to the sun Have fluids on hand, both at home and away Recognize signs of dehydration. To avoid infection: Consider having the child wear a Medic Alert bracelet Have the child vaccinated as recommended by the health care provider Share the above information with teachers and other caretakers, when necessary They should take supplements of folic acid (essential for producing red blood cells) because red blood cells are turned over so quickly. Antibiotics and vaccines are given to prevent bacterial infections, which are common in children with sickle cell disease. Blood transfusions are used to treat a sickle cell crisis. Nursing Diagnosis: 1. Altered nutrition, less than body requirements related to reported inadequate iron intake, knowledge deficit regarding iron reach foods. Goal: Patient will receive adequate supply of iron. Intervention: Provide diet counseling to care giver, especially in regard to food source of iron (e.g. meat, liver, fish, egg yolks, green leafy vegetable, nuts, whole grains, infants cereals and dry cereals). Expected Outcomes: Child receive at least minimum dailyrequirement of iron. Nursing Diagnosis: 2-Risk for injury related to abnormal hemoglobin, decreased ambient oxygen, and dehydration. Patient Goal 1: Will maintain adequate tissue oxygenation. Nursing Intervention: Explain measures to minimize complications related to physical exertion and emotional stress to avoid additional tissue oxygen needs. Prevent infection. Avoid low-oxygen environment. Expected Outcome: Child avoids situations that reduce tissue oxygenation. Patient Goal 2: Will maintain adequate hydration. Nursing Intervention: Calculate recommended daily fluid intake (1600 ml/m3/day) and base child’s fluid requirements on this minimum amount (specify) to ensure adequate hydration. Increase fluid intake above minimum requirements during physical exercise/emotional stress and during crisis to compensate for additional fluid needs. Give parents written instructions regarding specific quantity of fluid required to encourage compliance. Encourage child to drink to encourage compliance. Teach family signs of dehydration to avoid delay in rehydration therapy. Stress importance of avoiding overheating as source of fluid loss. Expected Outcome: Child drinks an adequate amount of fluid and shows no signs of dehydration. Nursing Diagnosis: 3. Anxiety /fear related to diagnostic procedures, transfusion. Goal: Patient, family will become knowledgeable about the disorder. Intervention: Prepare the child for tests. Remain with the child during tests and initiation of transfusion. Explain purpose of blood components. Expected Outcomes: Child and family display minimal anxiety. Child and family demonstrate an understanding of the disorders, diagnostic tests and treatment. Nursing Diagnosis: 4. Activity intolerance related to generalized weakness, diminished oxygen delivery to tissues. Goal: Patient will receive adequate rest. Intervention: Provide diversional play activities that promote rest and quite but prevent boredom and withdrawal. Choose appropriate roommate of similar age and interests who requires restricted activities. Plan nursing activities to provide sufficient rest. Assist with activities requiring exertion. Expected Outcomes: Child plays and rests quietly and engages in THALASSEMIA Thalassemia is a blood disorder passed down through families an inherited autosomal recessive blood disease in which the body makes an abnormal form of hemoglobin, the protein in red blood cells that carries oxygen. The disorder results in excessive destruction of red blood cells, which leads to anemia. CAUSES : Hemoglobin is made of two proteins: Alpha globin and beta globin. Thalassemia occurs when there is a defect in a gene that helps control production of one of these proteins. There are two main types of thalassemia: 1-Alpha thalassemia : occurs when a gene or genes related to the alpha globin protein are missing or changed (mutated). 2-Beta thalassemia : occurs when similar gene defects affect production of the beta globin protein. Alpha thalassemias occur most commonly in persons from southeast Asia, the Middle East, China, and in those of African descent. Beta thalassemias occur in persons of Mediterranean origin, and to a lesser extent, Chinese, other Asians, and African Americans There are many forms of thalassemia. Both alpha and beta thalassemia include the following two forms: Thalassemia major Thalassemia minor Thalassemia major : occurs if the baby receive the defective gene from both parents. Thalassemia minor: occurs if the baby receive the defective gene from only one parent. Persons with this form of the disorder are carriers of the disease and usually do not have symptoms. β-Thalassemia Major(Cooley’s Anemia) It is most common form of thalassemia in the world. More common in countries around Mediterranean Sea. It is inherited as autosomal genetic disorder of both genes controlling ß- chain synthesis (homozygous). Normal postnatal hemoglobin (Hgb A) is composed of two α and two β- polypeptide chains, in thalassemia major there is a partial or complete deficiency in the synthesis of β- chain of Hgb molecule. Consequently, there is a tremendous increase in the synthesis of α- chains and у chains. SIGN & SYMPTOM The most severe form of alpha thalassemia major causes stillbirth (death of the unborn baby during birth or the late stages of pregnancy). Children born with thalessemia major (Cooley's anemia) are normal at birth, but develop severe anemia during the first year of life. SINGS & SYMPTOM Unexplained fever. Poor feeding. Markedly enlarged spleen. Headache. Bone pain. Decreased exercise tolerance. Anorexia. Frequent epistaxis. Hemochromatosis. Hemosiderosis. Other Features: Small stature. Delayed sexual maturation. Protrusion of the abdomen (hepato- splenomegaly). Bone Change (older children if untreated): Enlarged head. Prominent frontal and parietal bosses. Flat or depressed bridge of the nose. Enlarged maxilla. Protrusion of the lip and upper central incisors and eventual malocclusion. TREATMENT : Patients with thalassemia minor usually do not require any specific treatment unless they have very low HB. Treatment for patients with thalassemia major includes chronic blood transfusion therapy. iron chelation therapy to remove excess iron from the body. splenectomy . Bone marrow transplant may help treat the disease in some patients especially children. THERAPEUTIC MANAGEMENT: Blood Transfusion. Chelation Therapy Nursing Diagnosis: Anxiety / fear related to diagnostic procedures, transfusion. Activity intolerance and comfort altered related to hematomas in tissues and joints. High risk for bleeding after minor hematomas related to deficiency of coagulation factor. Pain related to bleeding in joints. Impaired physical mobility related to hemorrhage in joints and tissues. Altered family process related to child with chronic illness. Planning: The objectives of nursing care can be divided into immediate needs and long-term goals: Prevent bleeding. Recognize and control bleeding. Prevent crippling effect of bleeding. Support family and prepare for home care. Identify persons at risk. Implementation: 1. Prevent Bleeding: Prophylactic administration of AHF. Appropriate exercises to strengthen muscles and joints and to allow age appropriate activity. To prevent oral bleeding, some readjustment in terms of dental hygiene may be related to, minimize trauma to the gums such as use of a water-irrigating device, softening the toothbrush in warm water before brushing. A peripheral fingerstick is better for blood samples and subcutaneous route is substituted for IM whenever possible. Neither aspirin nor any aspirin- containing compound should be used. Acetaminophen (Tylenol) is a suitable aspirin substitute, DISSEMINATED INTRAVASCULAR C OAGULATION DIC DIC is aserious bleeding disorder resulting from accelerated normal clotting with a subsequent decrease in clotting factors & platelets leading to uncontrolled bleeding . Etiology : it is always a result of another disease or condition ,it is often associated with shock ,infection ,hemolytic processes such as transfusion of mismatched blood . Sing & symptom : 1- bleeding: can occur any where in the body following trauma or normal activity or spontaneously . 2- specific sing & symptom : Slow,persistent ,prolonged bleeding from minor injuries . Uncontrollable hemorrhage subsequent to dental extraction or irritation of the gums . Epistaxis especially after facial injury . Hematuria. Ecchymosis ( petechiae are rare ). Bleeding into joints (hemarthrosis )which may lead to severe joint deformity . HEMOPHILIA Is a disorder of hemostasis of one or more clotting factor. Type : 1-hemophilia A: deficient in factor VIII,called classic hemophilia . 2- hemophilia B: deficient in factor IX : called christmas disease . Etiology : sex link recessive traits occur almost exclusively in male ,female carriers transmit the disease Hemophilia (Classic Hemophilia) It is one of the commonest (95%)congenital coagulation disorders due to deficiency or functional abnormality of factor VIII demonstrated as a sex- linked ressive trait (male is diseased and female is carrier). Blood clotting occurring in 3 phases, each is dependent on the preceding phase. The basic defect of hemophilia (A) is a deficiency of factor VIII (antihemophilic factor AHF). AHF is produced by the liver and is necessary for formation of thromboplastin in phase I of blood coagulation. The less AFH in the blood, the more severe the disease. The frequency and severity of bleeding are related to level of factor VIII deficiency: Clinical severity Factor VIII Activity Bleeding Tendency Severe 1% _Spontaneous bleeding without trauma. Moderate 1%-5% _Bleeding with trauma. Mild 5%- 50% _Bleeding with severe trauma or surgery. Sing & symptom : 1-Bleeding Skin : petechia ,purpura , hematoma . Head :gingival bleeding & epistaxis . GI: hematemesis & melena . Renal: hematuria . Nuro :headache , altered LOC. CV: symptom of shock . 2-platelet cunt is decreased . 3-prolong coagulation test . TEATMENT The primary therapy for hemophilia is replacement of the missing clotting factor. Vigorous therapy is instituted to prevent chronic crippling effects from joint bleeding. If replacement therapy is begun immediately, local measures such as ice applications and splinting are seldom needed. Other drugs may be included in the therapy plans depending on the source of the hemorrhage. Corticosteroids are used to treat inflammation in the joints; nonsteroidal antiinflammatory drugs such as aspirin, indomethasin (Indocin) and phenylbutazona (Burazolidin) should not be used because they inhibit platelet function. NURSING DIAGNOSIS: Anxiety / fear related to diagnostic procedures, transfusion. Activity intolerance and comfort altered related to hematomas in tissues and joints. High risk for bleeding after minor hematomas related to deficiency of coagulation factor. Pain related to bleeding in joints. LEUKEMIA It is a malignant disorder involving bone marrow dysfunction manifested by anemia, thrombocytopenia, and abnormal proliferation of white cells, which results in harmful filtration into tissues. It is the most common malignancy in childhood (30%), peak incidence 2-8 years of age. Incidence among males is greater than females’ 2:1. Etiology: Although the exact cause is unknown, but multiple factors believed to be responsible: ionizing radiation, chemicals (benzene compound, heavy metals), drugs (Alkylating agents), and chromosomal abnormalities (Down syndrome), and familial predisposition. Classification: Leukemia is classified according to its predominant cell type and level of maturity as described by the following: Lympho for Leukemias involving the lymphoid or lymphatic system. Myelo for those of myeloid (bone marrow) origin. Blastic and acute for those involving immature cells. Cytic and chronic for those involving mature cells. In children two forms are generally recognized: Acute lymphoid leukemia (A.L.L.) and acute nonlymphoid leukemia (A.N.L.L) or (A.M.L). A.L.L includes lymphatic, lymphocytic, lymphoblastic and lymphoblastoid leukemia. A.N.L.L. type includes granulocytic, myelocytic, monocytic, myelogenous, monoblastic and monomyeloblastic. Common symptoms of chronic or acute leukemia may include: Swollen lymph nodes that usually don't hurt. Fevers or night sweats. Frequent infections. Feeling weak or tired. Bleeding and bruising easily (bleeding gums, purplish patches in the skin, or tiny red spots under the skin). Swelling or discomfort in the abdomen (from a swollen spleen or liver). Weight loss for no known reason. Pain in the bones or joints. TREATMENT pharmaceutical medications, typically combined into a multi-drug chemotherapy regimen. Some are also treated with radiation therapy. In some cases a bone marrow transplant is useful Nursing diagnosis: 1. High risk for infection related to depressed body defenses. Goal: Patient will experience minimized risk of infection. Intervention: Place child in private room. Advise all visitors and staff to practice hand washing. Screen all visitors and staff for signs of infection. Use aseptic technique. Evaluate child for any potential sites or infections. Provide nutritionally complete diet for age. Nursing diagnosis: 2. High risk for injury (hemorrhage) related to interference with cell proliferation. Goal: Patient will exhibit no evidence of bleeding. Intervention: Use all measures to prevent infection, especially in ecchymotic area. Use local measures to stop bleeding. Restrict strenuous activity that could result in accidental injury. Involve child in responsibility for limiting activity when platelet count drops. Administer platelets as prescribed. Expected Outcome: Nursing diagnosis: 3. Altered nutrition less than body requirement related to loss of appetite. Goal: Patient will receive adequate nutrition. Intervention: Encourage parents to relax pressure placed on eating. Allow child any food tolerated. Improve quality of food selections when appetite increases. Stress expected increase in appetite from steroid. Take advantage of any hungry period, sever small snakes. Allow child to be involved in food preparation and selection. Make food appealing. Remember usual food practices of children in each age group. Expected Outcome: Nutrition intake is adequate. REFERENCES www.nlm.nih.gov/medlineplus/ency/hptt. Medical –surgical nursing ,health & illness prespectives ,seventh edition . www.ar.wikipedia.org/wiki/ www.en.wikipedia.org/wiki/Thalassemia