Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Diagnosis of hepatitis,
cholecystitis, liver
cirrhosis.
Chronic hepatitis polyetiological chronic
liver inflammatorydestructive nature with
moderate fibrosis and
preserved lobular
structure, lasting more
than 6 months.
Etiology: the onset and progression of infectious and
noninfectious nature is crucial defective immune
response to damage liver tissue. Hepatitis viral, toxic
and alcoholic lesions developed not only as a result of
damages which the agent, but also as a result of an
immune reaction cell type against hepatocytes.
Damage liver hepatotoxic viruses emerging area of
immune cytolysis of hepatocytes in which the virus
persists and there are its markers - surface antigens of
viruses. Induces immune cytolysis: antibodies fixed on
the surface of hepatocytes exhibit a cytotoxic effect and
induce cytotoxic T-lymphocytes against liver cells. At the
same cells transformed with K-cells (killer), sensitized to
hepatocytes caused by migration of cells formed
inflammatory infiltrate, composed in viral hepatitis
include lymphocytes, macrophages, fibroblasts.
Clinical manifestations of hepatitis
and cirrhosis of the liver:
Asthenic syndrome.
Asthenic phenomena accompany most
liver diseases are often the first signs of
illness.
Characterized by weakness, decreased
performance, increased fatigue, loss of
previous interests reduction initiatives.
Changing emotional background of the
man - depressed mood, depression,
irritability episodes
Diarrheal syndrome
Dyspeptic symptoms, early signs of liver
damage.
Dry and bitter taste in the mouth - most often
met symptoms.
Nausea, vomiting, belching.
Discomfort right subcostal area - a
characteristic feature. The equivalent symptom
is a feeling of heaviness in the epigastrium,
constant bloating.
Decreased appetite combined with intolerance
of many products.
Constipation particularly pronounced in portal
hypertension.
Diarrhea alternating with constipation.
There slimming down to cachexia.
Abdominal pain.
The most easy option - a feeling of
heaviness, pressure in the upper
abdomen. Monotone pain in the right
upper quadrant due to stretching of the
fibrous membrane of the liver, most
often appear after eating.
Pain can be long or sharp. Sometimes
the pain is located in the right subcostal
area , and under the breasts.
Cholestatic syndrome.
Manifested persistent or intermittent
ochrodermia, skin itching, dark urine,
feces lightening.
Vehetodystonic syndrome.
Psycho-emotional instability, insomnia,
headache, cardialgia, fluctuations in
blood pressure, sweating.
Febrile syndrome.
Unexplained fever, prolonged or
recurrent, most often seen in
chronic active hepatitis, in the
active stage of liver cirrhosis. The
reason could be severe overgrowth
of endogenous intoxication,
periodic bacteremia.
In 2/3 patients with cirrhosis due to
fever associated infectious lesions pneumonia, ascites - peritonitis.
Articular syndrome.
Joint pain, prolonged or
intermittent, without
deformation accompanying
reactive hepatitis and
cirrhosis of the liver.
Hemorrhagic syndrome.
Bleeding from the nose and gums,
subcutaneous hemorrhage, menorrhagia,
bloody vomiting, tarric excrements.
Edematous-ascitic syndrome.
Fluid retention, increasing the size of
the abdomen, swelling of the legs.
Entsefalopatyc syndrome.
Memory loss, drowsiness,
dyzoriyentation in time and space,
inappropriate behavior.
Classification
I.
Etiology:
viral
alcoholic
autoimmune
toxic
drug (toxic-allergic)
nonspecific reactive
Secondary biliary
hepatitis with hepatic
cholestasis outside
II. The morphological
changes:
1. Persystic
2. Lobular
3. Activities:
a) with moderate
activity;
b) a high degree of
activity.
4. Cholestatic
Classification
III. The clinical course:
Phase of aggravation
Phase of remission
IV. For the functional
state of the liver:
compensated
decompensated
Physical examination:
-Skin - greyish-pale, can be local or diffuse
hyperpigmentation (melasma).
-Jaundice - develops when hyperbilirubinemia above 30
mmol / l, expressed in bilirubin more than 120 mmol / l.
-Originally jaundice appears on the palate and sclera,
sometimes there is only partial ochrodermia nasolabial
triangle, forehead, palms. Itching and traces solutions,
caused an increase in the skin of bile acids.
-Teleangiectasia, or star-shaped angiomas on the neck,
face, shoulders, back , racemes. Their expression is
reduced in the fall of blood pressure, bleeding. Xanthoma
- internally yellow skin plaques that form in severe
hyperlipidemia.
Hemorrhage into the skin - pinpoint
hemorrhages develop in protracted course of
hepatitis.
For chronic liver disease characterized by
painless superficial hemorrhages in the skin
and mucous membranes, bleeding from the
gums, nose, uterine bleeding.
Palmar eritema (liver palms) - symmetric
splotchy red palms and soles. Spots become
pale with pressing and again blush at the
termination of pressure.
"Crimson, the cardinal's tongue" - and no
sinergy of papillae of the tongue to the degree
of "patent" surface. Atrophy of the shoulder
musculature due to violation of protein
metabolismand hormonal imbalance.
There is thickening of the distal
phalanges of the fingers of the type
"drumsticks“
Gynecomastia - female type hair on the
body develops as a result of increased
estrogen levels.
Possible loss of pubic hair, axillary
areas, testicular atrophy. Syndrome
most often occurs in alcoholic hepatitis.
Leg swelling, lymphadenopathy - arises
in severe hypoalbuminemia.
Enlargement of the liver - a
characteristic sign of its parenchyma.
Reducing the size of the liver is rare, in
the later stages of cirrhosis of the liver
is a bad prognostic sign. On palpation
the liver during severe pathological
process activity observed liver
tenderness. Liver tissue is sealed, the
edge can be condensed, the pointed,
hilly.
Splenomegaly is not typical for most
cases of hepatitis
Diagnostic tests.
-Zag en. blood - anemia, leykopeniya. Acute alcoholic
hepatitis occurs with leukocytosis, a sharp increase in
ESR, stab shift.
-Tjtal urine test - a possible micro hematuria, mild
proteinuria
-biochem. of blood - an increase of ALT and AST,
hlutamat dehidrohenaze, lactate dehydrogenase, iron,
vitamin B12, an alkaline phosphatase linked (direct)
bilirubin, total bilirubin, cholesterol, reduced albumin,
protein, prothrombin complex.
-Sonography of liver: increased in size, increased density
heterogeneity of ehostruktures.
-Radionuclide study of liver. Used radiopharmaceutical
Bengal pink for study of liver function.
- Morphological study of the liver - punctures on biopsy.
Treatment
depends on the etiology, process activity severity.
A during acute process.
Bedrest
Diet 5
Drugs that improve metabolism in liver cells - ATP, Vit. B
group, Glutamic acid.
Hepatoprotectors: Essenciale forte, Gepabene, Sealy
boron, Vitohepat.
Glucocorticoids: Prednisolone, Methyl Prednisolone (at
high process activity).
Amino quinoline drugs: Delahil, Plakvenil,
immunosuppressive drugs: Azathioprine, Cyclosporine.
when viral hepatitis B, C, D - interferons α, β, γ.
Detoxification Therapy - Gemodez, Glucose, Sodium
Thiosulfate, enzyme preparations.
Adsorbents bile acids - Bilihnin, Cholestyramine,
Activated carbon with vitamins A, D, E, K, Enterodez,
Ursofalk.
Oxygen therapy, herbal medicine Bile - Yarrow,
Immortelle, Hypericum, Rose, Dandelion roots.
Cirrhosis
This is a progressive, diffuse, polyetiological
disease characterized by a significant
decrease in the mass of functioning
hepatocytes, fibrosis with impaired hepatic
lobule structure and vasculature liver.
Etiology
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
Alcoholic
Virus (HBV, HVC, HBV + HDV)
Primary biliary cirrhosis
Secondary biliary cirrhosis
Violation of venous outflow from the liver
Metabolic
Toxic
Nutritional
Cryptogenic
Parasitic diseases
Shunt surgery for intestinal
Diagnosis. Main symptoms
and syndromes:
Astenovegetative, edematous syndrome,
endotoxemia, hyperbilirubinemia, diarrhea,
intrahepatic cholestasis, portokavalnoho bypass,
hepatomegaly, splenomegaly, mesenchymalinflammatory, cytolytic, bleeding, hepatocellular
failure, portal hypertension, malabsorption,
anemia, hormonal imbalance.
Physical data
Resized and seal liver
Palpable spleen determined
Spider veins on the upper trunk and
face
Palmar erythema
Gynecomastia and testicular atrophy
Veins on the anterior abdominal wall
Ascites
jaundice
Laboratory parameters
Hematologic: concentration of Hb, # of
leukocytes and platelets, Coagulation, blood
type, Rh factor, prothrombin index.
Biochemical: bilirubin, albumin, globulin,
chloride, urea, creatinine, K, Na, copper, iron,
Ig in the serum activity of ALT, AST, alkaline
phosphatase.
Immunological indices serum
HBsAg, anti-HVC, antibodies to smooth
muscle, to soluble liver antigen, α-feto-protein.
Instrumental research
Esophagogastroduodenoscopy
Doppler-ultrasound liver
Computed tomography of the liver
Krizshkirna needle biopsy
Radioisotope scanning of the liver
Fluoroscopy esophagus and stomach
Treatment of cirrhosis
Regieme - depending on the stage of
cirrhosis.
Diet № 5 in portal hypertension - bezso
Levu, in hepatic coma - Protein-free.
Detoxification therapy: Neogemodez,
Glucose.
Anti-inflammatory therapy: steroids,
antibiotics, immunosuppressants,
hepatoprotectors, adsorbents bile acids,
drugs that improve metabolism in
hepatocytes, pancreatic enzymes
"The main symptoms and syndromes in
diseases of the hepato-biliary system.
Methods of clinical, laboratory and
instrumental examination. '
Chronic non-calculous (bilestone free)
cholecystitis (sholecystitis chronica) - a chronic
inflammatory disease.
Polyetiological gall bladder, which is
combined with motor-tonic disorders
(dyskinesia), biliary tract and changes in
physico-chemical properties and biochemical
composition of bile (dysholia).
Etiology.
1.
2.
3.
4.
5.
Bacterial infections
Parasitic infestation
Duodenobiliar reflux
Allergies
Chronic inflammatory disease of the
digestive system.
6. Acute cholecystitis.
Predisposing factors
1. Stagnation of bile.
2. Reflex effects from abdominal organs
during development in their overall
process.
3. Intestinal dysbiosis.
4. Metabolic disorders contributing to
changes in physico-chemical properties
and composition of bile (obesity, diabetes,
gout).
5. Hereditary with respect to XX.
The main pathogenic
factors:
1.
2.
3.
4.
5.
Neurodegenerative changes ZHM wall.
Neuroendocrine disorders.
Stagnation and dysholiya bile.
Violation of the wall ZHM.
Factors:
Allergic reactions and
Immunoinflammatory.
Classification of chronic
cholecystitis
1.
2.
3.
4.
Etiology: kolibatcilic, enterokokcial, strepto-, stafilo-,
pneumococcal, Salmonella, typhoid, dysentery,
brutselozal, paratyphoid and others.
The degree of severity: mild, moderate, severe.
The nature of the course: recurring, monotonous,
intermittent.
During phases: pointed, decreasing exacerbation,
stable remission, unstable remission.
In the presence of complications, uncomplicated,
complicated periholecistitis.
Clinical
Subjective symptoms:
-Pain at HBH localized in the area of right
hypochondrium, sometimes in the epigastrium,
radiating to the right shoulder blade, sometimes - in
the collarbone.
-Dyspeptic symptoms:
nausea, vomiting, a feeling of bitterness in the mouth,
belching bitter. Due to the development of secondary
gastritis, pancreatitis, enteritis appear heartburn,
belching rotten, flatulence, loss of appetite, diarrhea.
Itchy skin.
-Fever.
-Psycho-emotional disorders:
depression, weakness, fatigue, irritability, emotional
lability.
Physical examination .
Review.
Most patients say overweight.
In some patients there subictericity of scleras and skin.
Palpation marked tenderness in the region of the gallbladder.
May show some positive signs:
Symptom Zakharyin - pain when pressing the point ZHM.
S-m of Vasilenko - when tapped at the point ZHM at the
height of inspiration there is a sharp pain.
S-m of Obraztsov-Murphy - after clicking on the area offered
ZHM patient to breathe, while the patient "intercepts" breath
of pain in the ZHM.
S-m of Ker - pain on vdosi during palpation right
hypochondrium.
S-m of Ortner - pain when tapped his hand on the edge of
right costal arch.
S-m of Myusi cardiology - pain at the point of the phrenic
nerve (frenikus-symptom).
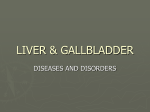
Pain point at disease gall
bladder:
1 - cystic point
2 - epigastric area
3 - choledochitis-pancreatic area
4 - zone in the area of proc. acromion
5 - point n. phrenici
6 - spade point
7 - point at the end of the 12th rib
8 - point about 8 - 11 thoracic vertebrae
9 - point to the right of 12 thoracic vertebrae
Laboratory and instrumental methods
1.
2.
3.
4.
Total blood: moderate leukocytosis, left shift with increasing stab leukocytes,
ESR acceleration.
Biochemical analysis of blood: an exacerbation of increased content of
sialic acids seromucoid, fibrin, alpha 2-globulin, possibly gamma globulin.
Imunolohiche blood research: reduced number of B and T lymphocytes
and IgA.
Fractional duodenal intubation:
Changes of duodenal intubation (portions "B"), typical of chronic cholecystitis:
- The presence of large numbers of leukocytes, especially their clusters.
- Detection by visual inspection bile pronounced turbidity, flakes of mucus.
- Established in bile of a large number of cells columnar epithelium.
- The appearance of cholesterol crystals and calcium bilirubinate.
- Reduction of relative density and pH of gallbladder bile.
- Changes in biochemical composition of bile (increased # of mucins
substances reduced content of bile acids, cholate-cholesterol ratio, lipid
complex)
- Bacteriological study: the number of bacteria than 100,000 in 1 ml of bile.
5. ultrasound:
Echo signs of Mts. cholecystitis
ZHM wall thickening greater than 2 mm;
sealing wall, especially with thickening;
unevenness and deformation path
bladder, increase or decrease the size,
adhesions;
reduction or absence of motion ZHM
breathing;
nonhomogenouse content of "gall
precipitate."
Ultrasound of the liver and gall bladder
6. Ro-study ZHM:
Cholecystography:
Signs HNH
- Impaired concentration ability and motor function
ZHM (sharp slowdown emptying ZHM);
- ZHM deformity (inequality contours due
pereholecystitis).
7. Computed tomography ZHM.
8. Radioisotope studies of biliary tract:
Symptoms: - persistent infringement speed filling
and emptying ZHM;
increase or decrease its size;
seal lying ZHM.
9. Thermography: observed local temperature increase
of 0,3 -2 ° C, zone ZHM looks bright.
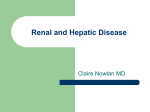
Cholelithiasis (CT scan)
1 - chronic cholecystitis (thickening of the walls of the gall bladder),
2 - calcium-containing stones in area neck of the gallbladder
Treatment
1.
2.
3.
4.
5.
6.
In acute patient lax recommend bed rest for 7-10 days, 1-2
days a warm drink.
Diet № 5, frequent meals (5-6 times / day)) in small portions.
Purchasing pain
m anticholinergics: Atropine Sulfate, Methacin, Platifillin
Gidrotartrata, Gastrotsepin;
antispasmodics: Papaverine, Nospanum;
Analgesics: Proteins, Baralgin, Droperiodol.
Antibiotic therapy in acute.
Appointed when thinking about the nature of the bacterial
disease have clinical and laboratory data confirming the
activity of the inflammatory process in ZHM (Erythromycin,
Ampicillin, Oxacillin, Lincomycin, Furazolizon, Penicillin,
Tetracycline, Blacks, Taryvid, Cephalosporin antibiotics).
Detoxification therapy in very severe exacerbation of
symptoms of intoxication: broths hips, alkaline mineral water /
drip - gemodez, polidez, 5% glucose isotonic district.
7. Bile means.
Rational choice bile depends on the phase of chronic
cholecystitis and concomitant type dyskinesia.
1) drugs that stimulate the formation of liver bile - Bile
true (choleretic):
preparations containing bile acids (Hologon, Deholin,
Alahol, Festal, Holenzim, Liobil);
synthetic choleretic (Nikodin, Tsykvalon, Oksafenamid);
vegetable (Immortelle, Corn Silk, Flamini, Peppermint,
Holosas, Parsley);
hidroholiretyky (water type "NAFTA");
2) drugs that stimulate bile (holekinetiki): Xylitol,
Sorbitol, MgSO4, Tansy.
8. Normalization function of the autonomic NS:
sedativ, minor tranquilizers.
9. Immunomodulatory therapy: Timalin, Taktyvhin, Sodium Nukleinat, Adaptogens
(Ginseng, Pantocrinum, Siberian ginseng).
10. Physiotherapy treatment.
11. When stihanii acute phenomena inductothermy, UHF, microwave, SMT, UST,
electrophoresis of novocaine, MgSO4,
applications paraffin wax, ORT,
balneotherapy.
12. Treatment of mineral water.
13. Spa treatment in remission (Truskavets
Gusyatin, Satan, Essentuki, Borjomi).
Chronic calculous cholecystitis
(sholecystitis chronica calculosa, cholelithiasis)
- a disease characterized by the formation of
stones in the gallbladder, at least - in the bile
ducts.
In the development of gallstones are important
metabolic disorders, infection and bile stasis.
There are three stages of gallstone disease.
The first stage (physical and chemical).
The second stage (latent) is characterized by
changes in lithogenic bile to form gallstones.
The third stage of cholelithiasis - clinical
(calculous cholecystitis).
Clinical
Subjective symptoms:
The most characteristic feature of the disease is a
liver or biliary colic. Intense pain localized in the right
upper quadrant and epigastric, radiating to the back,
chest thing, right shoulder, shoulder, arm. Join
nausea, repeated vomiting, which does not facilitate
pain, bloating, delayed stool. With prolonged fit of
itching appears.
Physical examination.
On examination can detect jaundice (the second day),
xanthoma. There bloating, muscle tension and local
tenderness in the right upper quadrant. Positive gallmihurni symptoms and areas of hyperesthesia (lower
angle shoulder, shoulder area, paravertebral right
from VIII to IX thoracic vertebra).
Xanthelasma of the upper eyelid
Laboratory and instrumental methods
In the biochemical analysis of blood observed increase in
cholesterol levels, increasing the activity of alkaline
phosphatase.
Ultrasound. The smallest size of stones that can diagnose = 1-2
mm. Often unable to determine sediment (sand) in ZHM.
Cholecystography. Stones in the bile ducts and ZHM seen as a
zone of enlightenment.
Treatment.
First stage: diet number 5, eat lots of vegetables, fruits,
regularly engage in physical activity, obesity be prevented.
Second stage: to dissolve cholesterol (x-RAY negative)
gallstones prescribe (Henohol, Henofalk) and
urodyzoksyholevoyi (Ursofalk, Urso - 100) acids.
In the third stage of the disease, during an attack of bilious
colic, the patient admitted to the surgical department. Assign
antispasmodics, analgesics, if necessary - to operate.
Cholangitis (angiocholitis - cholaengitis) inflammation of the bile ducts. There are acute and chronic
cholangitis. Chronic cholangitis may be latent, recurrent
and prolonged septic component of the course.
Clinical
The feeling of heaviness or dull pain in the right upper
quadrant, which occurs in violation diet bumpy ride,
physical work. The pain spread to the right shoulder and
shoulder.
Diarrheal syndrome: a bitter taste in the mouth, aversion
to fatty foods, nausea when inhaled the smell of this dish.
Itching of the skin that can occur to limit the area.
Astenodepresyvnyy syndrome: weakness.
Long periods of unwarranted subfebrile with periodic fever.
When viewed subikteryc mucous. They exhibit a larger
soft, tender liver.
Laboratory and instrumental
methods
Complete blood count: leukocytosis, left shift, accelerated
ESR, anemia.
Biochemical analysis of blood: increased bilirubin, alpha 2 and
γ-globulin, transaminases, alkaline phosphatase, γhlyutamiltranspeptydazy, sialic acid, fibrin.
Urine lab. the possible emergence of protein cylinders bilirubin.
Fractional duodenal intubation. Portion B - a large number of
shallow cylindrical epithelium. Portion C - bacterial flora,
leukocytes, increase in sialic acid, fibrin, enzymes.
Ultrasound - expanding intrahepatic bile ducts, liver
enlargement.
Intra / a cholangiography or endoscopic retrograde pankreatoholangiohraphy exhibit advanced bile duct.
Treatment
Diet number 5a;
antibacterial;
bile med-s.
if necessary - surgery.
Hepatorenal syndrome. About hepatorenal syndrome talking
when along with marked and anatomically proven liver and
biliary tract revealed signs of kidney damage. It is most
commonly observed in liver cirrhosis.
Cholestatic syndrome. (Cholestasis syndrome). It is
characterized by dark, like brown skin, intense itching, which
precedes the appearance of jaundice. On the palms in the
corners of the eyes, the outer surface of the elbows, knees flat
formation appear yellow due to hypercholesterolemia xanthelasma. In some cases there may be fever, chills. In blood
levels of conjugated bilirubin, cholesterol, β-lipoprotein,
hemahlyutamintransferazy. Urine is dark in color, like color of
beer, feces may be bright.
The syndrome of hepatic failure (insuffitientia hepatitis) - is a
violation of the liver, accompanied by severe disorders of
homeostasis and violation of the internal organs, especially the
central nervous system.
Diarrheal syndrome is characterized by nausea, spitting,
heartburn, vomiting, appetite disturbance.
Pain in the right upper quadrant.
Chronic autoimmune hepatitis
More common in girls and young women aged 10-30 years, at
least women in menopause. According to the literature, the
ratio of women and men in this disease 3-1.
Beginning disease can manifest weakness, anorexia, dark
urine, jaundice prior. Chance of a extrahepatic manifestations:
fever, joint damage that gives rise to the diagnosis of rheumatic
fever, lupus.
In later stages: fever to subfebrile digits combined with
arthralgia. The process involved large joints of the upper and
lower extremities, occasionally spine.
Configuration joints varies mainly due peryartykulyar
inflammation and tendon-muscle syndrome.
Chronic autoimmune hepatitis is a systemic disease with
lesions of the skin, mucous membranes and internal organs. It
is characterized by the presence of pleuritis, myocarditis,
pericarditis, ulcerative colitis, glomerulonephritis.
Described Cushing's syndrome, diabetes, generalized
lymphadenopathy, hemolytic anemia
The disease has a continuous flow. In the study
revealed an increase in blood levels of bilirubin,
aminotransferases.
Hypergammaglobulinemia occurs so often that one of
the names of this form of the disease is "progressive
hyperhammaglobulinemic hepatitis." Typical
hypoalbuminemia, significant deviations thymol and a
sharp slowdown allocation of bromsulfaleyin. Possible
signs of hypersplenismus (platelets and leukopenia).
Often there are positive LE-cell phenomenon,
antinuclear factor, complement fixation, high (1:160,
1:320 and higher) titer of antibodies to tissue smooth
muscle (the latter is a pathognomonic sign of liver
damage).
Pain in the right upper quadrant, constantly aching, often
intense, sharply intensified after exercise. This pain associated
with inflammatory infiltration in the connective tissue in the liver
capsule. In some patients the equivalent is the feeling of
heaviness and fullness in the right upper quadrant.
Diarrheal syndrome appears distorted taste of food, constant
nausea, which increases after meals and medication depends
on the violation of decontaminating the liver and reactive
pancreatitis.
Syndrome "small" liver failure, which manifested drowsiness,
severe bleeding, transient jaundice and ascites occurs in
patients with severe necrotic changes in hepatocytes.
For cholestasis syndrome characterized by itching, increased
bilirubin, cholesterol, alkaline phosphatase, gammahlutamiltransferazy serum
Hepatomegaly is found in all cases HVH. In acute liver disease
stands at 5-7 cm from the edge of the arc, it is moderately
dense, tapered edge, palpation is painful. Remission
accompanied by a marked decrease in liver. The spleen is
enlarged slightly.
Blood analysis revealed during acute
hypergammaglobulinemia, hypoalbuminemia,
increased thymol and activity of aminotransferases
(ALT, AST more). Increasing total protein and bilirubin
in serum. In remission, these figures are improving,
but do not reach the standards.
Ultrasound shows moderate hepatomegaly with a
rounded bottom edge of both particles liver. Prolonged
disease decreases sound conductivity and elasticity of
the liver. Some diagnostic value has nuclear scans.
Chronic hepatitis B (chronic viral hepatitis B) in 10-20% of
cases are due to acute process. Major antigenic and serological
markers of viral replication - HBV DNA, DNA polymerase, HbeAg, anti-Ig NBc class M. They are found in patients with chronic
disease and they are an indicator of activity of the process. The
presence of NVs-Ag in serum is a sign of viral persistence.
Chronic hepatitis C (HVHS) occupies a special place among
HVH because 20-50% of cases transformed into cirrhosis. HCV
virus is heterogeneous, is not less than 6 of its types, which
differ both in the degree of pathogenicity, and the sensitivity to
interferon. Feature of HCV is that its replication can occur not
only in the liver tissue, but also in mononuclear cells. This
explains poliorhannist damage in HCV. The basis of
extrahepatic manifestations (idiopathic thrombocytopenia,
aplastic anemia, uveitis, lesions of the thyroid gland, systemic
vasculitis, etc.). Lie as a direct effect of the virus, and
autoimmune reactions.
Chronic hepatitis D (XVHD) runs as a mixed infection
because replication of the virus (NDV) is required
HbsAg hepatitis B virus (HBV).
Chronic drug-induced hepatitis (HMH) - drug liver
damage - is an urgent problem due to the increasing
number of different medications, uncontrolled use,
widespread polypharmacy. HMH is up to 5% of all
chronic heptytiv.
Damaging factors can be realized in the form of
autoimmune and toxic reactions. Hepatotoxic agents
can cause necrosis already in high doses and their
toxicity increases with dose (chloroform, muscarinic et
al.). Effects of other drugs due to idiosyncrasy and is
independent of dose (chlorpromazine, ftorotan,
isoniazid, erythromycin, tetracycline, anabolic steroids,
oral contraceptives, and others.) May manifest
metabolic or immunological disorders.
Chronic cryptogenic (idiopathic) hepatitis. This group includes
chronic hepatitis without identified etiology, which may be due
to insufficient sensitivity of existing serological tests, especially
to certain subtypes faith hepatitis B, C or D, their mutations and
other causes. In addition, it is expected that other types of
hepatitis viruses are not identified so far.
In establishing the diagnosis of chronic hepatitis B should
reflect the etiology, pathogenesis, level of activity and stage of
disease. The degree of activity (weight process) for chronic
hepatitis determined by enzyme laboratory tests and
morphological study of liver biopsy. From laboratory signs is to
identify the most informative alanine aminotransferase (ALT) increasing its level of 3-5 reflects the minimum of 5-10 times moderate, more than 10 times - a high degree of activity.
In the morphological study using semi-quantitative analysis of
the index of histological activity (ISSAR) - "index Knodel".
Step hCG reflects prebih disease and is characterized by the
degree of liver fibrosis until the development of cirrhotic
changes. There fibrosis: portal, periportal,
peryhepatotselyulyarnyy.
Weather. In chronic hepatitis mostly favorable, especially after
the elimination of etiological factors.
Prevention of chronic hepatitis includes early diagnosis,
adequate treatment of acute viral hepatitis, clinical supervision
for him, to prevent exposure to various industrial, medical and
consumer intoxication others.
Treatment of chronic viral hepatitis. Should exclude all
hepatotoxic effects (contact with hepatotropic poisons the
workplace, alcohol). Obmezhuyetsya heavy physical work. Not
intended medication slowly neutralized liver (tranquilizers,
sedatives, analgesics) are contraindicated physiotherapy on the
plot liver balneotherapy. In acute disease surgery performed
only for health indications.
Recommended diet number 5. Food consumed 4-5
times a day in small portions.
Drug therapy involves the use of immunostimulants
(levalizol, timalin, T-activin) and antiviral drugs
(interferon ademin-arabinoside). The main treatment
for patients with chronic viral hepatitis is interferon
(IF). It inhibits virus replication and stimulates the
production of endogenous ineterferonu. Treatments IF
long enough: at least 4-6 months with HVH type B (510 million IU 3 times a week subcutaneously or
intramuscularly), up to 18 months at HVH type C (3
million IU 3 times per week), and 12 months at HVH
type D (10 million IU 3 times a week). Possible
combinations of IF with antioxidants dezoksyholevoyu
acid and drugs from the group hepatoprotetoriv
(essentiale, vitamins B, C, etc.).. In chronic
autoimmune hepatitis commonly used steroids in
combination with immunosuppressive drugs.
cirrhosis
Cirrhosis (sirrhosis hepatis) - Polyetiological chronic
progressive disease with severe symptoms in varying
degrees of functional liver failure and portal
hypertension, the main feature of which is the
significant growth of connective tissue.
The morphological structure distinguish large-, MKD,
mixed and biliary (primary and secondary) liver.
Mixed (macro-mikronodulyarnu) form is diagnosed
when a number of small and large sites about
equally.
Large-(makronodulyarnyy, postnekrotychnyy) cirrhosis is
characterized by the formation of nodes of various sizes over
3mm in diameter. Some units reach 5 cm size liver may be
normal, increased and decreased sharply.
The initial clinical manifestations of large-cirrhosis is often
dyspeptic syndrome (loss of appetite, flatulence), asthenia
(decreased performance, irritability, hipohondriya), pain or a
feeling of heaviness in the upper abdomen. On examination
revealed liver enlargement with thickening and deformation of
the surface, the liver edge sharpened. Initially, there is a
uniform increase in both particle unsharp liver. Subsequently
often dominates the increase of the left lobe. Portal
hypertension in the initial stage shows moderate splenomegaly.
In the expanded stage of the disease early and persistent
symptoms, regardless of etiological and morphological types is
a pain in the right upper quadrant and hepatolienal syndrome.
This can be detected signs hipersplenizmu (leukopenia,
thrombocytopenia, anemia).
diarrheal syndrome
skin changes
Fever lasted
Hemorrhagic syndrome
The syndrome of gastrointestinal tract
Hepatopankreatic syndrome
intestinal lesion
Syndrome of endocrine disorders
Toxic encephalopathy syndrome
Syndrome of cardiovascular changes
Clinically distinguish light, medium and severe
hepatocellular failure:
light - general weakness, degradation, loss of appetite,
nausea;
medium - jaundice, drowsiness, decreased mental
abilities, "liver palms" appearance of vascular "stars"
on the body, hemorrhagic syndrome (bleeding from
the nose, with esophageal varices, hemorrhoids veins,
hemorrhage);
severe - impaired consciousness until its complete loss,
muscle twitching, they cramp, periodic excitation.
Reflexes fade, lowers blood pressure, increases
respiration rate, and so on.
MKD (mikronodulyar, portal) cirrhosis - units of the same size,
with a diameter of 1-3 mm. Liver of normal size or enlarged.
This form of cirrhosis is often observed in alcoholism, bile duct
obstruction, breach of venous outflow, hemochromatosis.
The initial stage (diarrheal) vascular and parenchymal
compensation. The clinic is dominated dyspeptic,
astenovegetative syndromes. Standing is a sign of a moderate
increase in the liver.
Extensive stage (ascites) accompanied by manifestations of
primary parenchymal and portal decompensation. In the initial
stage of clinical signs attached portal hypertension (Fig. 3),
hemorrhagic syndrome, endocrine disorders, jaundice, "hepatic
features", weight loss and atrophy of skeletal muscles. During
acute increases body temperature. The liver is enlarged, firm,
often rough, rounded edge. Increased spleen. In general blood
test show signs of moderate anemia, leukopenia,
thrombocytopenia, and increased ESR.
Phase of severe parenchymal and portal failure (kahektychna).
Pronounced symptoms of the second stage. Typical is with
cholestatic jaundice component severe hemorrhagic syndrome
(nosebleeds, distributed or pislyain'yektsiyni spontaneous
ecchymosis), hepatic encephalopathy. Severe signs of portal
hypertension: ascites, dilatation of abdominal wall ("Head of
Medusa") (Fig. 5), right pleural effusion, umbilical hernia,
bleeding from hemorrhoidal veins of esophageal varices and
gastric. Can a progressive decrease in the size of liver. In
general blood test show signs hypersplenizmus, accelerated
ESR.
In biochemical analysis of blood - reducing total protein, albumin,
cholesterol, prothrombin, increased ALT, bilirubin, indicators of
thymol. In the analysis of urine - proteinuria, microhematuria,
cylindruria. Ultrasound examination of the liver reveals
hepatosplenomegaly, diffuse lesions, ascites, sudden
expansion of portal vein, absence of respiratory fluctuations
lumen of portal vein. In Radionuclide imaging the liver are
hepatomegaly, diffuse lesions, diffuse weakening hatching,
uneven intensity figure.
Biliary cirrhosis
is divided into primary and secondary. The basis
of primary biliary cirrhosis is an autoimmune
disease that begins as a chronic
nonsuppurative destructive cholangitis. Long
time no severe symptoms. More common in
women over 35 years. The most common and
most constant symptom is itchy skin.
Inconsistent initially it for years ahead of
jaundice, which gives rise to long-term
treatment of "skin disease". Subsequently itch
becomes a constant, increasing after a warm
bath at night. There is a dark brown
pigmentation of the skin in the area of the
blades, jaundice cholestatic type xanthelasma.
Rarely is expressed mild hepatomegaly.
Extensive stage disease is characterized by the
increase of jaundice, fever to febrile digits
depletion until cachexia due to malabsorption in
the intestines. Often there is redness of her
hands, sometimes with a yellowish tinge ("liver
palms"). In some cases, changing as nails
watch glass. Thickening of distal phalanges
("drumsticks")
In end-stage (terminal) itchy skin decreases.
Pigmented skin thickens, coarsens, it can
manifest as swelling in scleroderma. A violation
occurs secretion of bile malabsorption of fatsoluble vitamins, osteoporosis.
MKD (mikronodulyar, portal) cirrhosis - units of the
same size, with a diameter of 1-3 mm. Liver of normal size or
enlarged. This form of cirrhosis is often observed in alcoholism,
bile duct obstruction, breach of venous outflow,
hemochromatosis.
The initial stage (diarrheal) vascular and parenchymal
compensation. The clinic is dominated dyspeptic,
astenovegetativnogo syndromes. Standing is a sign of a
moderate increase in the liver.
Extensive stage (ascites) accompanied by manifestations of
primary parenchymal and portal decompensation. In the initial
stage of clinical signs attached portal hypertension (Fig. 3),
hemorrhagic syndrome, endocrine disorders, jaundice, "hepatic
features", weight loss and atrophy of skeletal muscles. During
acute increases body temperature. The liver is enlarged, firm,
often rough, rounded edge. Increased spleen. In general blood
test show signs of moderate anemia, leukopenia,
thrombocytopenia, and increased ESR.
Blood analysis increases the activity of enzymes of
cholestasis: alkaline phosphatase,
leytsynaminopeptydazy, gamma
hlyutamiltranspeptydazy.
Increased bilirubin slow and occurs in the later stages.
Increasing the concentration of bile acids and copper
content in serum and iron levels decreased.
Typical is hyperlipidemia with increasing concentrations
of cholesterol, beta-lipoproteins, phospholipids.
The level of circulating immune complexes, exhibit
kriohlobuliny, antimitochondrial antibodies.
Ultrasound detects unchanged bile duct, liver biopsy in
the study are nonsuppurative destructive cholangitis
intrahepatic in the early stages of the disease, then biliary cirrhosis.
Secondary biliary cirrhosis is caused by prolonged
violation vidtikannya bile at large intrahepatic ducts, due to
strictures, stones, primary metastatic tumors. Clinic determined
the primary disease. It is dominated by such signs as jaundice,
diffuse hyperpigmentation of the skin, its dryness, thickening
and itching. Sometimes the forefront aholiya, steatorrhea.
Almost always there is pain. Characterized by hyperthermia,
sweating. More pronounced than in primary biliary cirrhosis,
avitaminosis fat-soluble vitamins A, C, and D. The blood found
neutrophilic leukocytosis, accelerated erythrocyte
sedimentation rate.
Treatment for cirrhosis of the liver
Assign diet number 5 (with Pevsner). If the patient
shows signs of hepatocellular failure, then limit the
protein, with edema - salt.
Drug therapy includes drip of 5% Glucose solution,
Dextran, Alvezin, Reohlyumanu with detoxification
effect, improves microcirculation. In addition, the tools
that affect the liver cell membrane (Essenciale,
Lipostabil, Kars, Hoftiol, Riboksin). In portal
hypertension, ascites using Potassium-sparing
diuretics (Veroshpiron, Triamterene), which can be
combined with Saluretics (Furosemide, Urehit,
Oksodomin), beta-blockers. The use of diuretics
requires periodic prescribing potassium (Asparcam,
Panangin). Assign vitamins A, D, E, C, B vitamins to
reduce itching - Cholestyramine, Carbon and Silicon
sorbents.
When symptoms of encephalopathy apply glutamic
acid, Ornitsetyn, Hoftiol, Purslane, Antibacterials,
Plazmaforez, Hemosorbtion. When ascites
intravenously administered native plasma albumin,
which increase the osmotic pressure of the plasma,
improve metabolism in liver cells.
During resistant ascites, which defies adequate
therapy accession hepatorenal syndrome threats
abdominal bleeding apply parantsentez (removed no
more than three liters of fluid).
Unfavorable prognosis. The average life span of
patients with cirrhosis 4-6 years. It remains the longest
performance with biliary cirrhosis, less - in portal and
postnekrotyc cirrhosis.
Prevention. First elimination or limitation of etiological
factors, timely diagnosis and treatment of chronic
hepatitis and liver.
Thanks for your
attention!