Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
浙江大学医学院八年制教学
神经精神与运动1(模块2)
运动系统慢性疾病
肩关节周围炎、腱鞘炎
股骨头坏死
浙江大学医学院附属二院骨科
吴立东
运动系统慢性损伤
Bursitis
滑囊炎
滑囊炎是指滑囊的急性或慢性炎症。滑囊是结缔组织中的
囊状间隙,是由内皮细胞组成的封闭性囊,内壁为滑膜,
有少许滑液。少数与关节相通,位于关节附近的骨突与肌
腱或肌肉、皮肤之间。凡摩擦力或压力较大的地方,都可
有滑囊存在,其作用主要是有利于滑动,从而减轻或避免
关节附近的骨隆突和软组织间的摩擦和压迫
Bursae are sacs lined with a membrane similar to synovium; they
usually are located about joints or where skin, tendon, or muscle
moves over a bony prominence.
may or may not communicate with a joint.
Function: reduce friction, protect delicate structures from
pressure.
Bursae are similar to tendon sheaths and the synovial
membranes of joints and are subject to the same
disturbances: (1) acute or chronic trauma, (2) acute or
chronic pyogenic化脓性 infection, and (3) low-grade
inflammatory conditions such as gout, syphilis,
tuberculosis, or rheumatoid arthritis.
Two types of bursae: normally present (as over the
patella and olecranon) and adventitious ones (such as
develop over a bunion姆囊炎, an osteochondroma骨
软骨瘤, or kyphosis驼背 of the spine). Adventitious
bursae are produced by repeated trauma or constant
friction摩擦 or pressure.
急性滑囊炎:急性滑囊炎的治疗的特征是
疼痛,局限性压痛和活动受限。如为浅部
滑囊受累(髌前及鹰嘴),局部常红肿,化学
性(如结晶所致)或细菌性滑囊炎均有剧烈疼
痛,局部皮肤明显发红、温度升高,发作
可持续数日到数周,而且多次复发。异常
运动或用力过度之后能出现急性症状
Treatment---the cause of the bursitis
Systemic causes, such as gout痛风 or syphilis梅毒,
and local trauma or irritants should be
eliminated, and, when necessary, the patient's
occupation or posture should be changed. One
or more of the following local measures usually
are helpful: Rest, hot wet packs, elevation, and,
if necessary, immobilization of the affected part.
Surgical procedures useful in treating bursitis are
(1) aspiration and injection of an appropriate
drug, (2) incision and drainage when an acute
suppurative 化脓性bursitis fails to respond to
nonsurgical treatment, (3) excision of
chronically infected and thickened bursae, and (4)
removal of an underlying bony prominence.
Carpal Tunnel Syndrome
腕管综合症
(another name: tardy median palsy)
results from compression of the
median nerve within the carpal tunnel.
The syndrome consists predominantly
of tingling刺痛 and numbness
in the
innervated
typical median nerve distribution in the
radial three and one-half digits (thumb,
index, long, radial side of ring). Pain
occurs diffusely in the hand and
radiates up the forearm. Thenar手掌
atrophy usually is seen later in the
course of the nerve compression.
The syndrome frequently is associated with
nonspecific tenosynovial edema and rheumatoid
tenosynovitis, as are trigger finger and de
Quervain disease. Some studies reported biopsy
specimens of the flexor tendon synovium from
21 patients with “idiopathic特发性” carpal
tunnel syndrome. The findings were similar in all
and were typical of a connective tissue结缔组织
undergoing degeneration under repeated
mechanical stress.
Diagnosis
Paresthesia感觉异常 over the sensory distribution of
the median nerve is the most frequent symptom; it
occurs more often in women and frequently causes the
patient to awaken several hours after getting to sleep
with burning and numbness of the hand that is relieved
by exercise. The Tinel sign may be demonstrated in
most patients by percussing轻叩 the median nerve at
the wrist. Atrophy to some degree of the medianinnervated thenar muscles has been reported in about
half of the patients treated by operation.
Acute flexion of the wrist for 60 seconds in some but
not all patients or strenuous use of the hand increases
the paresthesia. Application of a blood pressure cuff
on the upper arm sufficient to produce venous
distention may initiate the symptoms. Some studies
evaluated the clinical usefulness of commonly
administered provocative tests, including wrist flexion,
nerve percussion, and the tourniquet test, in 67 hands
with electrical proof of carpal tunnel syndrome and in
50 control hands.
Diagnosis
The most sensitive test was the wrist flexion test,
whereas nerve percussion was the most specific and the
least sensitive. They also found that with the wrist in
neutral position, the mean pressure within the carpal
tunnel in patients with carpal tunnel syndrome was 32
mm Hg. This pressure increased to 99 mm Hg with 90
degrees of wrist flexion and to 110 mm Hg with the
wrist at 90 degrees of extension. The pressures in the
control subjects with the wrist in neutral position were
25 mm Hg, 31 mm Hg with the wrist in flexion, and 30
mm Hg with the wrist in extension.
Sensibility testing in peripheral nerve
compression syndromes was investigated, found
that threshold tests of sensibility correlated
accurately with symptoms of nerve compression
and electrodiagnostic studies.
Electrodiagnostic电生理 studies are reliable confirmatory tests.
Ultrasonography超声检查 has been used to show the
movement of the flexor tendons within the carpal tunnel, but it
does not clearly show soft tissue planes. Early reports of
magnetic resonance imaging (MRI) in carpal tunnel syndrome
are promising. A major advantage of MRI is its high soft tissue
contrast, which gives detailed images of both bones and soft
tissues. Care should be taken not to confuse this syndrome with
nerve compression caused by a cervical disc herniation, thoracic
outlet structures, and median nerve compression proximally in
the forearm and at the elbow.
Treatment
If mild symptoms have been present and there
is no thenar muscle atrophy, the injection of
hydrocortisone into the carpal tunnel may afford
relief. Great care should be taken not to inject
directly into the nerve. Injection also can be
used as a diagnostic tool in patients without
bony or tumorous blocking of the canal;
65% of these cases probably are caused by a nonspecific
synovial edema, and these seem to respond more
favorably to injection. Injection also helps to eliminate
the possibility of other syndromes, especially cervical
disc or thoracic outlet syndrome. Some patients prefer
to receive injections two or three times before a surgical
procedure is carried out. If the response is positive and
there is no muscle atrophy, conservative treatment with
splinting and injection is reasonable.
Treatment
If signs and symptoms are persistent and
progressive, especially if they include thenar
atrophy, division of the deep transverse carpal
ligament is indicated. The results of surgery are
good in most instances, and benefits seem to last
in most patients.
Although thenar atrophy may disappear, it
resolves slowly, if at all. As noted earlier, when
symptoms of median nerve compression
develop during treatment of an acute Colles
fracture, the constricting bandages and cast
should be loosened and the wrist should be
extended to neutral position. When median
nerve palsy develops after a Colles fracture and
has gone unrecognized for several weeks,
surgery is indicated without further delay.
Lateral epicondylitis
肱骨外上髁炎
Lateral epicondylitis (tennis elbow), a
familiar term used to described a myriad
of symptoms about the lateral aspect of
the elbow, occurs more frequently in
nonathletes than athletes, with a peak
incidence in the early fifth decade and a
nearly equal gender incidence.
Activities that require repetitive
supination and pronation of the forearm
with the elbow in near full extension.
Tenderness is present over the lateral epicondyle
approximately 5 mm distal and anterior to the
midpoint of the condyle. Pain usually is
exacerbated by resisted wrist dorsiflexion and
forearm supination, and there is pain when
grasping objects. Plain roentgenograms usually
are negative; occasionally calcific tendinitis may
be present. MRI demonstrates tendon
thickening with increased T1 and T2 signals but
generally is not indicated.
Regardless of the underlying cause,
nonoperative treatment is successful in 95% of
patients with tennis elbow. Initial nonoperative
treatment includes rest, ice, injections, and
physical therapy centered around treatment such
as ultrasound, electrical stimulation,
manipulation, soft tissue mobilization, friction
massage, stretching and strengthening exercises,
and counter-force bracing.
If prolonged (6 to 12 months), operative
treatment may be considered; it is effective in
90% of properly selected patients.
Adhesive Capsulitis
(frozen shoulder.)
肩周炎或称冻结肩
Frozen shoulders in patients who report no
inciting event and with no abnormality on
examination (other than loss of motion) or
plain roentgenograms were designated as
"primary," and those with precipitant
traumatic injuries as "secondary." This
division helps in planning treatment but
does not necessarily predict outcome.
No formal inclusion criteria. There are no
universally accepted criteria for the diagnosis of
frozen shoulder. internal rotation frequently is
lost initially, followed by loss of flexion and
external rotation.
The incidence of frozen shoulder in the general
population is approximately 2%. (an increased
incidence associated with, including diabetes
mellitus (up to 5 times more), cervical disc
disease, hyperthyroidism, intrathoracic disorders,
and trauma). People between the ages of 40 and
70 are more commonly affected. Common to
almost all patients is a period of immobility, the
etiologies of which are diverse
Primary Frozen Shoulder
Primary frozen shoulder is a vague entity that only
rarely recurs in the same shoulder. The clinical course
of primary (idiopathic) frozen shoulder consists of
three phases.
Phase I—Pain. Patients usually have a gradual onset of
diffuse shoulder pain, which is progressive over weeks
to months. The pain usually is worse at night and is
exacerbated by lying on the affected side. As the patient
uses the arm less, pain leading to stiffness ensues.
Primary Frozen Shoulder
Phase II—Stiffness. Patients seek pain relief by
restricting movement. This heralds the
beginning of the stiffness phase, which usually
lasts 4 to 12 months. Patients describe difficulty
with activities of daily living; men have trouble
getting to their wallets and women with
fastening brassieres. As stiffness progresses, a
dull ache is present nearly all the time (especially
at night), and this often is accompanied by sharp
pain during range of motion at or near the new
endpoints of motion.
Primary Frozen Shoulder
Phase III—Thawing. This phase lasts for weeks
or months, and as motion increases, pain
diminishes. Without treatment (other than
benign neglect) motion return is gradual in most
but may never objectively return to normal,
although most patients subjectively feel near
normal, perhaps as a result of compensation or
adjustment in ways of performing activities of
daily living.
Secondary Frozen Shoulder
Unlike patients with idiopathic frozen shoulder,
patients with secondary frozen shoulder can
recall a specific precipitating event, possibly
related to overuse or injury. The three phases of
classic frozen shoulder may not all be present
and may not follow the previously outlined
chronology; fortunately, treatment for the two
entities is similar.
Diagnosis
tests in patients with a frozen shoulder (including plain
film roentgenograms) usually are normal, except in
those with medical disorders such as diabetes or thyroid
disease. Bone scans have been reported to be positive in
some patients.
Arthrograms characteristically show a reduced joint
volume with irregular margins. Clinical improvement
has been reported after arthrography because of
brisement of adhesions from forcefully injecting fluid
into the joint. A volume of less than 10 ml and lack of
filling of the axillary fold currently are accepted
arthrographic findings indicative of a frozen shoulder.
Treatment
Traditionally, frozen shoulder has been considered a selflimiting condition, lasting 12 to 18 months.
Approximately 10% of patients have long-term problems.
Patients seeking care earlier usually recover more quickly.
Dominant shoulder involvement has been reported to be
predictive of a good result, whereas occupation and
treatment programs are not statistically significant.
Obviously, the best treatment of frozen shoulder is
prevention (secondary frozen shoulder), but early
intervention is of paramount importance; a good
understanding of the pathological process by the patient
and the physician also is important.
Treatment
Initial treatment is nonoperative, with emphasis
placed on control of pain and inflammation.
passive and active range-of-motion exercises.
Abduction should be avoided initially to prevent
impingement until joint motion becomes more
supple.
Treatment
Although a frozen shoulder usually is self-limiting and
resolves in 12 to 18 months, many patients do not wish
to wait that long for resolution of symptoms and
request active intervention long before 12 months. With
appropriate patient selection, significant improvement
can be obtained in approximately 70% of patients.
Closed manipulation under anesthesia
Open release of contractures
Treatment
Arthroscopic release is
an option when closed
manipulation fails or for
patients who have had
prolonged, recalcitrant
adhesive capsulitis.
Stenosing Tenosynovitis
狭窄性腱鞘炎
more often in the hand and wrist than
anywhere else in the body.
A peritendinitis may affect these tendons,
causing pain, swelling, and crepitus捻发音 .
When the long flexor tendons are involved,
trigger thumb, trigger finger, or snapping finger
occurs. The stenosis occurs at a point where the
direction of a tendon changes, for here a fibrous
sheath acts as a pulley滑轮 , and friction is
maximal. Although the tenosynovium lubricates
the sheath, friction can cause a reaction when
the repetition of a particular movement is
necessary, as in winding a fine coil of wire线圈
or stacking laundry.
DE QUERVAIN DISEASE
Stenosing tenosynovitis of the abductor pollicis longus
and extensor pollicis brevis tendons
When the extensor pollicis brevis and the abductor pollicis
longus tendons in the first dorsal compartment are affected, the
condition is named after the Swiss physician, De Quervain, who
described his experience in 1895.
Women are affected 10 times more frequently than men. The
cause is almost always related to overuse, either in the home or at
work, or is associated with rheumatoid arthritis. The presenting
symptoms usually are pain and tenderness at the radial styloid.
Sometimes a thickening of the fibrous sheath is palpable.
diagnosis
The Finkelstein test usually is positive:
"on grasping the patient's thumb and
quickly abducting the hand ulnarward,
the pain over the styloid tip is
excruciating." Although Finkelstein
states that this test is "probably the
most pathognomonic objective sign," it
is not diagnostic; the patient's history
and occupation, the roentgenograms,
and other physical findings must also be
considered.
Treatment
Conservative treatment, consisting of rest
on a splint and the injection of a steroid
preparation into the tendon sheath, is most
successful within the first 6 weeks after
onset.
When pain persists, surgery is the
treatment of choice (complete relief ).
TRIGGER FINGER AND THUMB
弹响指和弹响拇
Stenosing tenosynovitis, leading to inability to extend
the flexed digit ("triggering") usually is seen after 45
years of age.
Patients may note a lump块 or knot小结 in the palm.
The lump may be the thickened area in the first annular
part of the flexor sheath, or a nodule or fusiform纺锭
状 swelling of the flexor tendon just distal to it. The
nodule can be palpated by the examiner's fingertip and
will move with the tendon. The tendon nodule usually
is at the entry of the tendon into the proximal annulus
at the level of the metacarpophalangeal joint.
Treatment of trigger digits usually
is nonoperative in the
uncomplicated patient who
presents a short time after onset of
symptoms. Nonoperative methods
include stretching, night splinting,
and combinations of heat and ice.
Corticosteroid injection is effective
after one injection
Surgical release reliably relieves the
problem for most patients
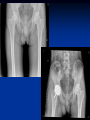
Osteonecrosis of Femoral head
股骨头无菌性坏死
Osteonecrosis of the femoral head is a
progressive disease that generally affects patients
in the third though fifth decades of life; if left
untreated, it leads to complete deterioration of
the hip joint. It is estimated that as many as
20,000 new cases of osteonecrosis are diagnosed
each year in the United States.
Diagnosis
Patients are typically asymptomatic early in the course
of osteonecrosis and eventually have groin pain on
ambulation. A thorough history and physical
examination should be done to discover potential risk
factors and determine the clinical status of the patient.
Plain roentgenograms should be obtained including
anteroposterior and lateral views. Roentgenographic
changes seen in osteonecrosis depend on the stage of
the disease. Plain films may appear normal in the early
stages, but changes are noted as the disease progresses,
such as increased density or lucency in the femoral head.
Advances in MRI have made
earlier diagnosis of
osteonecrosis of the femoral
head possible and allow
determination of the exact
stage and extent of the
pathological process without
use of invasive methods.
Treatment
Core decompression
Bone Grafting
Vascularized Fibular
Grafting
Osteotomies of
Proximal Femur
Resurfacing Hemiarthroplasty
Total Hip Arthroplasty and Bipolar
Hemiarthroplasty.
Improved results recently have been reported with
modern cementing techniques and press-fit cementless
total hip arthroplasty in patients with osteonecrosis.
With new bearing surfaces becoming available, such as
ceramic on ceramic, metal on metal, and highly crosslinked polyethylene, results may improve even more.
The results of primary total joint replacement for
osteonecrosis are now approaching those reported for
osteoarthritis in aged-matched patients.
Epiphysitis of tibial tuberosity
胫骨结节骨骺炎
(Osgood-Schlatter disease)
(Osteochondrol disease of the tibial
tubercle)
EPIPHYSITIS OF TIBIAL TUBEROSITY
(OSGOOD-SCHLATTER DISEASE)
The terms osteochondrosis and epiphysitis designate
disorders of actively growing epiphyses. The
disorder may be localized to a single epiphysis or
occasionally may involve two or more epiphyses
simultaneously or successively. The cause
generally is unknown, but evidence indicates a
lack of vascularity that may be the result of
trauma, infection, or congenital malformation.
Treatment
Surgery rarely is indicated for Osgood-Schlatter disease;
the disorder usually becomes asymptomatic without
treatment or with simple conservative measures such as
the restriction of activities or cast immobilization for 3
to 6 weeks. In a review of the natural history of
untreated Osgood-Schlatter disease in 69 knees in 50
patients, found that 76% of patients believed they had
no limitation of activity, although only 60 could kneel
without discomfort.
In a prospective study of 17 patients with OsgoodSchlatter disease and 12 adolescents without anterior
knee pain, Aparicio et al. noted a strong association
between Osgood-Schlatter disease and patella alta. The
increase in patellar height may require an increase in the
force by the quadriceps to achieve full extension, which
could be responsible for the apophyseal lesion.
However, it can be argued that the patella alta is the
result of chronic avulsion of the bony tuberosity.
Surgery may be considered if symptoms are
persistent and severely disabling.
Complications reported of Osgood-Schlatter
disease whether treated surgically or not,
including subluxations of the patella, patella alta,
nonunion of the bony fragment to the tibia, and
premature fusion of the anterior part of the
epiphysis with resulting genu recurvatum.
Insertion of Bone Pegs
Incise the periosteum longitudinally distal to the
tuberosity. With an electric saw cut two matchstick pegs
4 cm long from the tibia; make the base of each peg
larger than its tip. Then drill two holes through the
tibial tuberosity—one near but not in contact with the
proximal tibial physis and slanting proximally and
laterally and the other also distal to the physis and
slanting proximally and medially. Insert the pegs into
these holes and resect their projecting ends.
technique for insertion of bone pegs for
Osgood-Schlatter disease
AFTERTREATMENT.
A cast is applied
from groin to toes and is worn for 2 weeks.
A cylinder walking cast is then worn for 4
more weeks.
Excision of Ununited Tibial Tuberosity
TECHNIQUE: Make a longitudinal incision centered
over the tibial tuberosity. Expose the patellar tendon
and incise it longitudinally. Elevate the tendon laterally
and medially and excise any loose fragments of bone
and enough tibial cortex, cartilage, and cancellous bone
to remove any bony prominence completely. Do not
disturb the peripheral and distal margins of the
insertion of the patellar tendon. Close the wound.
AFTERTREATMENT. A cylinder walking cast is
applied and worn for 2 to 3 weeks. Exercises are then
begun.
excision of
ununited tibial
tuberosity. A,
Tibial tuberosity
has been exposed.
B, Bony
prominence has
been excised.
Legg-Calve-Perthes DISEASE
Perthes病
The cause
The clinical sign
Plain roentgenographic changes
Bone scintigraphy
MRI
Treatment
classified patients with this disease into groups
according to the amount of involvement of the
capital femoral epiphysis:
group I, partial head or less than half head
involvement;
groups II and III, more than half head
involvement and sequestrum formation;
group IV, involvement of the entire epiphysis.
(1)
(2)
(3)
(4)
(5)
They noted certain roentgenographic signs described as
"head at risk" correlated positively with poor results,
especially in patients in groups II, III, and IV.
These head-at-risk signs include
Lateral subluxation of the femoral head from the
acetabulum,
Speckled calcification lateral to the capital epiphysis,
Diffuse metaphyseal reaction (metaphyseal cysts),
A horizontal physis,
Gage sign, a radiolucent V-shaped defect in the lateral
epiphysis and adjacent metaphysis.
Containment by femoral varus derotational
osteotomy for older children in groups II, III,
and IV with head-at-risk signs.
Contraindications include an already malformed
femoral head and delay of treatment of more
than 8 months from onset of symptoms.
Surgery is not recommended for any group I
children or any child without the head-at-risk
signs.
Salter and Thompson advocated determining the extent
of involvement by describing the extent of a
subchondral fracture in the superolateral portion of the
femoral head. If the extent of the fracture (line) is less
than 50% of the superior dome of the femoral head,
the involvement is considered type A, and good results
can be expected. If the extent of the fracture is more
than 50% of the dome, the involvement is considered
type B, and fair or poor results can be expected.
According to Salter and Thompson, this subchondral
fracture and its entire extent can be observed
roentgenographically earlier and more readily than
trying to determine the Catterall classification.
Furthermore, according to these authors, if the femoral
head is graded as type B, then probably an operation
such as an innominate osteotomy should be carried out.
After statistical analysis of 116 hips affected with
Perthes disease, Mukherjee and Fabry concluded that
Salter and Thompson's classification is simple and
accurate and can be applied early in the course of the
disease to determine management.
Conclusions
1. Most patients can be treated by noncontainment
methods and obtain good results (84%).
2. Satisfactory clinical results frequently can be obtained
at long-term follow-up despite an unsatisfactory
roentgenographic appearance.
3. The Catterall classification is a valid indicator of
results but is not applicable as a therapeutic guide.
4. Head-at-risk signs added little to the Catterall
classification as a prognostic indicator or therapeutic
guide.
5. All of the fair and poor results were in patients
with Catterall III or IV involvement and onset of the
disease at age 6 or later.
Injury of Meniscus
半月板损伤
The menisci are crescents, roughly triangular
in cross section, that cover one half to two
thirds of the articular surface of the
corresponding tibial plateau
TEARS OF MENISCI
Traumatic lesions of the menisci are produced
most commonly by rotation as the flexed knee
moves toward an extended position. The medial
meniscus, being far less mobile on the tibia, can
become impaled between the condyles, and injury
can result. The most common location for injury is
the posterior horn of the meniscus, and
longitudinal tears are the most common type of
injury.
The length, depth, and position of the tear
depend on the position of the posterior horn in
relation to the femoral and tibial condyles at the
time of injury. Menisci with peripheral cystic
formation or menisci that have been rendered
less mobile from previous injury or disease may
sustain tears from less trauma.
Congenital anomalies of the menisci, especially
discoid lateral meniscus, may predispose to
either degeneration or traumatic laceration.
Likewise, areas of degeneration that develop as a
result of aging cannot withstand as much trauma
as healthy fibrocartilage. Abnormal mechanical
axes in a joint with incongruities or ligamentous
disruptions expose the menisci to abnormal
mechanics and thus can lead to a greater
incidence of injury.
Classification
Numerous classifications of tears of the menisci
have been proposed based on location or type
of tear, etiology, and other factors; most of the
commonly used classifications are based on the
type of tear found at surgery. (1) longitudinal
tears(bucket handle tears), (2)body tears,
(3)anterior horn tears, (4)1/3 anterior tears,
(5)1/3 posterior tears, and (6) horizontal tears
Four basic patterns of meniscal tears: I, longitudinal; II,
horizontal; III, oblique; and IV, radial
Horizontal tears B
Oblique tears C
Radial tears D
Cysts of the menisci are frequently associated
with tears and are 9 times more common on the
lateral than on the medial side. The most
common cause is trauma that produces
degeneration and secondary mucinous and cystic
changes in the periphery of the meniscus;
Discoid menisci are abnormal, and because of
hypermobility and the bulk of the tissue
between the articular surfaces, they are
vulnerable to compression and rotary stresses.
Degeneration within the discoid meniscus, as
well as tears, may develop. The diagnosis often is
not made until surgery, since the discoid
meniscus may not produce significant symptoms
until some derangement of the meniscus occurs.
Diagnosis
The diagnosis of internal derangement of the
knee caused by a meniscal tear can be difficult
even for an experienced orthopaedic surgeon.
Using a careful history and physical examination
and supplementing standard roentgenograms in
specific instances with special imaging
techniques and arthroscopy can keep errors in
diagnosing tears of the menisci to less than 5%.
When a meniscus has been injured, capsular and
ligamentous structures, as well as the articular surfaces,
often have been injured also.
Disorders that can produce symptoms similar to those
of a torn meniscus must be kept in mind, and to avoid
error, a detailed, careful, systemic history and physical
examination supplemented with appropriate imaging
studies and arthroscopy are indicated, especially if
symptoms and findings are not quite typical of a torn
meniscus.
A history of specific injury may not be obtained,
especially when tears of abnormal or degenerative
menisci have occurred. This scenario is noted most
often in a middle-aged person who sustains a weightbearing twist on the knee or who has pain after
squatting. Tears of normal menisci usually are
associated with more significant trauma or injury but
are produced by a similar mechanism, as the meniscus
is entrapped between the femoral and tibial condyles in
flexion, tearing as the knee is extended.
Patients with tears in degenerative menisci may
recall symptoms of mild catching, snapping, or
clicking, as well as occasional pain and mild
swelling in the joint. Once the tear in the
meniscus becomes of significant size, more
obvious symptoms of giving way and locking
may develop.
The syndromes caused by tears of the menisci
can be divided into two groups: those in which
there is locking and the diagnosis is clear and
those in which locking is absent and the
diagnosis is more difficult. The injured knee can
be locked and still extend to neutral position.
Locking usually occurs only with longitudinal
tears and is much more common with bucket
handle tears, usually of the medial meniscus.
Locking of the knee
May be caused by:
a bucket handle tear of a meniscus
an intraarticular tumor
an osteocartilaginous loose body
other conditions
Regardless of its cause, locking that is unrelieved
after aspiration of the hemarthrosis and a period
of conservative treatment may require surgical
treatment.
No locking
A patient typically gives a history of several episodes of
trouble referable to the knee, often resulting in effusion
and a brief period of disability but no definite locking.
A sensation of "giving way" or snaps, clicks, catches, or
jerks in the knee may be described, or the history may
be even more indefinite, with recurrent episodes of
pain and mild effusion in the knee and tenderness in
the anterior joint space after excessive activity.
When well understood, the following clues can
be important in the differential diagnosis in this
second group: a sensation of giving way,
effusion, atrophy of the quadriceps, tenderness
over the joint line (or the meniscus), and the
reproduction of a click by manipulative
maneuvers during the physical examination.
Diagnostic Tests
Clicks or snaps, either audible or detected by
palpation during flexion, extension, and rotary
motions of the joint, can be valuable for
diagnosis, and efforts should be made to
reproduce and accurately locate them. If these
noises are localized to the joint line, the
meniscus most likely contains a tear. Similar
noises originating from the patella, the
quadriceps mechanism, or the patellofemoral
groove must be differentiated.
Numerous manipulative tests have been
described, but the McMurray test and the Apley
grinding test probably are most commonly used.
All basically involve attempts to locate and
reproduce crepitation that results as the knee is
manipulated.
The McMurray test
With the patient supine and the knee acutely and
forcibly flexed, the examiner can check the medial
meniscus by palpating the posteromedial margin of the
joint with one hand while grasping the foot with the
other hand. Keeping the knee completely flexed, the leg
is externally rotated as far as possible and then the knee
is slowly extended. As the femur passes over a tear in
the meniscus, a click may be heard or felt. The lateral
meniscus is checked by palpating the posterolateral
margin of the joint, internally rotating the leg as far as
possible, and slowly extending the knee while listening
and feeling for a click.
A click produced by the McMurray test usually is
caused by a posterior peripheral tear of the meniscus
and occurs between complete flexion of the knee and
90 degrees. Popping, which occurs with greater degrees
of extension when definitely localized to the joint line,
suggests a tear of the middle and anterior portions of
the meniscus. Thus the position of the knee when the
click occurs may help locate the lesion. A positive
McMurray click localized to the joint line is additional
evidence that the meniscus is torn; a negative
McMurray test does not rule out a tear.
Grinding test
Described by Apley
With the patient prone, the knee is flexed to 90 degrees and
the anterior thigh is fixed against the examining table.
The foot and leg are then pulled upward to distract the
joint and rotated to place rotational strain on the
ligaments; when ligaments have been torn, this part of the
test usually is painful. Next, with the knee in the same
position, the foot and leg are pressed downward and
rotated as the joint is slowly flexed and extended; when a
meniscus has been torn, popping and pain localized to the
joint line may be noted. Although the McMurray, Apley,
and other tests cannot be considered diagnostic, they are
useful enough to be included in the routine examination
of the knee.
Imaging Studies
Roentgenograms. AP, lateral, and intercondylar
notch views with a tangential view of the
inferior surface of the patella should be routine.
Ordinary roentgenograms will not confirm the
diagnosis of a torn meniscus but are essential to
exclude osteocartilaginous loose bodies,
osteochondritis dissecans, and other internal
derangements that can mimic a torn meniscus.
Other Diagnostic Studies
such as ultrasonography, scintigraphy, computed
tomography (CT), and magnetic resonance imaging
(MRI), have been shown to improve diagnostic
accuracy in many knee disorders. Their principal
attractiveness over arthrography or arthroscopy is that
they are noninvasive procedures.
in a prospective study comparing the accuracy of MRI
with arthroscopic findings, reported 98% accuracy for
medial meniscal tears, 90% for lateral meniscal tears
ARTHROSCOPY
Proven meniscal tears usually are treated surgically, by
arthroscopy.
Arthroscopy has made the diagnosis of acute meniscal
injuries more precise, which aids in the treatment
planning. Incomplete tears or small peripheral tears are
difficult to confirm without arthroscopy.
Many incomplete tears will not progress to complete
tears if the knee is stable. Small stable peripheral tears
have been observed to heal after 3 to 6 weeks of
protection.
Chronic tears with a superimposed acute injury cannot
be expected to heal with nonoperative treatment. Thus
an acute meniscal injury in a patient with a history of
symptomatic episodes such as catching, locking, and
giving way probably does not qualify for nonoperative
management.
Nonoperative treatment is never appropriate in a
patient with a locked knee caused by a bucket handle
tear of the meniscus. Forceful manipulation of such
displaced tears is never justified, and most will not heal
without surgery even if reduced.
Meniscal tears that cause infrequent and minimal
symptoms can be treated with rehabilitation and
restricted activity. Tears associated with ligamentous
instabilities can be treated nonoperatively if the patient
defers ligament reconstruction or if reconstruction is
contraindicated.
Chronic tears even within the vascularized zone will not
heal without surgery. However, chronic tears have been
shown to heal when the synovial bed of the meniscus
has been freshened and the torn edges have been
apposed and sutured.
The most important aspect of nonoperative treatment,
once the acute pain and effusion have subsided, is
restoration of the power of the muscles about the
injured knee to a level comparable with that of the
opposite knee. As much motion of the joint as possible
should be encouraged. This can be accomplished
through a regular program of progressive exercises, not
only for the quadriceps and hamstrings but also for the
hip flexors and abductors.
OPERATIVE MANAGEMENT
The indications and surgical techniques for excision of
torn menisci have been controversial; noted orthopaedic
surgeons have advocated total excision of the torn
meniscus, whereas others have proposed subtotal
excision. Justification for total excision often was based
on short-term, functional recovery criteria. When longer
follow-up was studied, increasing degenerative changes
were noted, especially after total meniscectomy was
performed. Degenerative changes probably caused by
biomechanical changes were directly proportional to the
amount of meniscus excised. In vitro that removal of
even one third of the meniscus increased the joint
contact forces by up to 350%.
The greatest degenerative changes in animals occurred
after total rather than subtotal meniscectomy. These
changes also have been observed arthroscopically in
human knees. After subtotal excision of the meniscus,
less articular cartilage degeneration was found, and it
was localized principally to the area previously covered
by the meniscus. The amount of degenerative change in
the articular cartilage was directly proportional to the
amount of meniscus removed.
If a significant portion of the peripheral rim can be
retained by subtotal meniscal excision, the long-term
result is improved.
Complete removal of the meniscus is justified
only when it is irreparably torn, and the meniscal
rim should be preserved if at all possible. Total
meniscectomy is no longer considered the
treatment of choice in young athletes or other
people whose daily activities require vigorous
use of the knee.
Excision of only the torn portion of the meniscus,
either by open arthrotomy or by arthroscopic technique,
has sufficient support and clinical results to indicate its
routine use. Subtotal excision of a torn meniscus by
open arthrotomy can be a difficult procedure and can
be accomplished more easily by arthroscopic techniques.
Late Changes after Meniscectomy
(半月板切除术后的晚期病变)
The knee can function well without the meniscus,
sometimes for the rest of a patient's life, but late
degenerative changes within the joint sometimes occur,
and the loss of the meniscus undoubtedly plays some
part in producing these changes. In addition to the
condition of the meniscus, numerous other factors can
influence long-term function, such as joint alignment,
laxity of the capsular or ligamentous structures, and
incomplete rehabilitation of the musculature about the
knee.
谢谢大家!
Thank you very much for
your attention!