Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
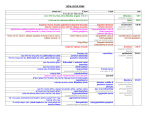
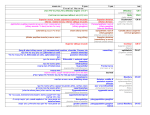
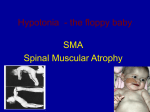
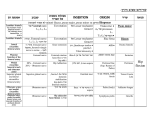
Emergencies in Palliative Care Objectives Manage palliative care emergencies Have a basic knowledge of appropriate treatments Know where to get help and advice Plan Ahead / Be prepared Understand importance of communication Know what supplies might be needed Advance care planning Palliative Care Emergencies Hypercalcaemia Superior Vena Cava Obstruction (SVCO) Spinal Cord Compression Haemorrhage / Bleeding Seizures / Fitting General Principles Anticipate Who is at risk? Plan Communication Preparation Avoid Correct the correctable Prophylaxis Factors to consider What is the emergency Can it be reversed General physical status of the patient Prognosis Burdens of treatment Patients and carers wishes מר לוי סובל מסרטן ראה . NSCC אתמול בגלל הדרדרות במצבו ,חולשה ניכרת קושי בעמידה ,החמרה בעצירות בצרבת ובכאב ,בדקת אותו וביקשת מהאחות לשלוח בדיקת דם .מה תבקש? אשתו מתקשרת אליך בשל החמרה במצבו :לא מסוגל לצאת מהמיטה ,נראה מעט מבולבל וגונח מכאב. Hypercalcaemia Who is at risk? 10-20% of all patients with malignant disease 50% of patients with myeloma 20% of breast and non small cell lung cancer patients Also commonly seen in oesophagus, thyroid, prostate, lymphoma, and renal cell carcinoma Hypercalcaemia Features Confusion Drowsiness Nausea and vomiting Constipation Polyuria and polydipsia Can mimic deterioration due to progressive malignancy Hypercalcaemia Diagnosis Check renal function and corrected calcium ( need to know albumin concentration) Corrected ca = measured Ca+(n ALBmALB)x0.8 Hypercalcemia Treatment Consider the goals Hydration and saline diuresis Bisphosphonates Steroids? FolIow 3-5 days prevention C. Woelk MD גב' זלץ בטיפולך בהוספיס בית בשל RCCמפושט. ידוע על מחלה גרורתית מפושטת לוריד החלול , בבלטות רטרופריטונאליות ובעמ"ש טורקלי ((D6- , 9באגן ובירך ימין. גב' זלץ קוראת לך בשל החמרה בכאב הגב ונימול הקורן ל 2הרגליים יותר לשמאל. לדבריה מתקשה ללכת לשירותים גם בעזרת ההליכון. Spinal Cord Compression (SCC) Occurs in advanced malignancy Main problem is lack of recognition Up to 5% of patients with cancer develop SCC There is a 30% 1 year survival Malignancies which commonly cause SCC include; prostate, breast, lung, myeloma, lymphoma and renal Spinal Cord Compression Compression of Vasculature Direct Compression Vertebral Mets Paraspinal mass Spinal Cord Compression (SCC) Most commonly affects thoracic level (70%) Signs and symptoms depend on the area of the cord affected Signs can be subtle to gross More than one level can be affected Compression below L2 affects the cauda equina Spinal Cord Compression Causes Vertebral metastases and collapse 85% Extravertebral tumour (extension into epidural space) Intramedullary tumour (from spinal cord) Intradural tumour (from meninges) Epidural metastases Spinal Cord Compression Features Pain (earliest symptom) Weakness Sensory changes and a sensory level tingling and numbness Sphincter dysfunction / perianal numbness Altered reflexes Can have resolution of the pain Examination Demarcated sensory loss Brisk or abscent reflexes Spinal Cord Compression Diagnosis Urgent MRI or CT Important early diagnosis! 70% have substantial weakness by the time of scanning 70% who can walk before treatment maintain mobility 35% of those with weakness regain function Only 5% completley paraplegic do so Management of SCC Oral dex 16mg (EMERG MNG IV 100MG ) Radiotherapy ( no spinal instability)20GR 5 # Surgery and radiotherapy ( spinal instability such as fracture Surgery alone relapse at previously irradiated site Chemotherapy Steroids alone Superior Vena Cava Syndrome The clinical manifestation of superior vena cava (SVC) obstruction, with severe reduction in venous return from the head, neck and upper extremities C. Woelk MD Superior Venacaval Syndrome . Superior Venacaval Syndrome Extrinsic tumour or Node Direct Invasion Intraluminal Thrombus Complication of Central Line Superior Vena Cava Syndrome Incidence and Etiology C. Woelk MD Usually associated with malignancies Often the initial presentation of cancer Bronchogenic carcinoma (80%) Lymphoma (15%) Metastatic disease (5%) Superior Vena Cava Syndrome Presentation Symptoms: Dyspnea Facial and neck swelling Fullness in head Cough Arm swelling Chest pain Dysphagia C. Woelk MD 63% 50% 50% 24% 18% 15% 9% Superior Vena Cava Syndrome Presentation Signs: Venous distention of neck Venous distention of chest wall Facial edema Cyanosis Edema of the arms Plethora of the face Vocal cord paralysis Horner’s syndrome 66% 54% 46% 20% 14% 10% 3% 3% Superior Vena Cava Syndrome Management Does not usually imply immediate threat to life, except when trachea or pericardium is compromised Important is to establish a diagnosis Emergency treatment indicated if: Compromised airway Decreased cardiac output Cerebral dysfunction C. Woelk MD Superior Vena Cava Syndrome Management C. Woelk MD Chemotherapy – SCLC, NHL Radiation - NSCLC Bed rest with head elevated Oxygen Diuretics Steroids- medium to high dose Severe hemorrhage Etiology Epistaxis GI bleeding: Hematemesis,Hematochezia,Melena Hemoptysis Hematuria Internal Bleeding Bleeding from fungating tumours Hemolysis C. Woelk MD Severe hemorrhage Important General Questions Is treatment of the underlying condition possible in the context of the bleeding? Is it possible to keep up with the loss of blood, and for how long? These may need to be addressed early, with the patient, family and caregivers. C. Woelk MD GI Bleeding Incidence and Etiology 80% of GI bleeding in cancer patients is from benign sources – good prognosis Massive hemorrhage is unusual ESOPHAGUS STOMACH SMALL INTESTINE COLORECTUM C. Woelk MD GI Bleeding Management Consider gastroscopy / colonoscopy / surgery if life expectancy reasonable. Avoid surgery if life expectancy < 2 months Stop potentially offending agents: e.g. NSAIDs Consider IV fluids, PPI C. Woelk MD GI Bleeding Management Massive Bleeding in the Terminal Phase: • • • C. Woelk MD Keep patient warm Consider sedation Green and black towels and sheets Hemoptysis Incidence and Etiology Present in 30-50% of primary lung neoplasms at the time of presentation 10 % of patients admitted to hospice Massive hemoptysis uncommon: Pulmonary embolism Bronchial bleeding due to tumour erosion Epistaxis C. Woelk MD Massive Hemoptysis Management Trendelenburg position Consider sedation Green and black towels C. Woelk MD Wound Bleeding Incidence and Etiology Bleeding is a common problem with malignant wounds May involve oozing from microvascular fragmentation to frank bleeding if vessels are involved C. Woelk MD Wound Bleeding Management For patients with malignant wounds, it will not be possible to heal the wound, unless one can treat the underlying cancer. Avoid adherent dressings. Keep the wound moist. Direct pressure, if actively bleeding Medicated dressing possibilities: Topical aminocaproic acid Topical dilute silver nitrate solutions C. Woelk MD Wound Bleeding Management If bleeding is possible, discuss this with the patient and family and staff If bleeding is catastrophic, dark towels may reduce anxiety of all involved If the patient is distressed, consider sedation C. Woelk MD Severe Hemorrhage Systemic Interventions C. Woelk MD D/C antiplatelet and anti-thrombotic agents Vitamin K Transfusion of blood or platelets Antifibrinolytic Medication Tranexamic acid Aminocaproic acid Desmopressin Octreotide (somatostatin analog) Severe Hemorrhage - Management Desmopressin (DDAVP) An analog of the posterior pituitary hormone: vasopressin Extensively used in Type 1 von Willebrand Disease 0.3-0.4 mcg/kg IV over 20 minutes OR 150300 mcg nasal inhalation Has been used successfully in acquired defects of platelet function – e.g. uremia, cirrhosis, ASA – and in variceal bleeding Avoid excessive fluid administration Severe Hemorrhage Management C. Woelk MD Remember the goals of care Keep patient, family, staff informed of progress and prognosis Seizures Incidence: 1% of patients with advanced cancer Seizures Etiology Most common: Primary or metastatic brain tumours CVA / Stroke Pre-existing seizure disorder Less common: Hypoxemia Metabolic: uremia, hypoglycemia, hyponatremia Sepsis Drug or alcohol withdrawal Seizures Education What to do if a seizure happens: Help avoid harm / trauma Do not restrain Do not attempt to insert anything orally Recovery position after the seizure Expect drowsiness for a while after Call for help if seizure lasts more than 5 minutes (it will feel like 30) Seizures Management C. Woelk MD Investigate as appropriate, based on patient’s status and course Generally felt unnecessary to give routine prophylaxis for seizures Grand Mal Seizures: Phenytoin is first drug of choice Focal Seizures: Carbamazepine is first drug of choice Other anticonvulsants may be needed Status epilepticus Management C. Woelk MD Protect airway Administer Oxygen Consider SC or IV Status epilepticus Medications IV available: Lorazepam 2-4 mg over 2-4 minutes Phenytoin load: 20 mg/kg at 25 mg/min Phenobarb 20 mg/kg at 100 mg/min IV unavailable Diazepam 10 mg solution PR C. Woelk MD May need to go as high as 30 mg/kg May be repeated q10minutes Midazolam SC infusion 1-3 mg / hour Consider steroids Multifocal Myoclonus C. Woelk MD Jerking, involuntary movements of arms and legs May start as subtle movements, and then become bothersome and disturbing Multifocal Myoclonus Etiology Very often associated with delirium and related to opioid toxicity May be a pre-terminal event Important to consider the differences C. Woelk MD Opioid Neurotoxicity C. Woelk MD Cognitive Dysfunction Myoclonus Hyperalgesia Allodynia Perceptual Disturbance Seizures Multifocal Myoclonus Management Stop the current opioid and rotate to a different one at 50-75% of the equivalent dose. Allow for adequate breakthrough doses Consider careful hydration Expect resistance from family / staff Interpreting the myoclonus and associated symptoms / signs as pain, and increasing the original opioid will eventually result in more myoclonus and delirium C. Woelk MD Summary Emergencies happen, even in dying individuals. Emergencies may be treated differently in the palliative population, with much more of an emphasis on symptom management than on attempts at reversing the disease process. Communication with the patient and family is extremely important for dealing with emergencies.