Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
General, Basic, Advanced &
Paramedic Review
Overview
Methodology of Instruction
Stipulations
2015 Changes
The 2015 Protocol
Questions & Answers
2
Methodology of Instruction
= Emergency Medical Responder Skills & Procedures
= Emergency Medical Technician Skills & Procedures
= Advanced Emergency Medical Tech. Skills & Procedures
= Paramedic Skills & Procedures
Italics = Physician’s Orders
Pink Text or Boxes Refer to Pediatric Orders
*** This is not a complete review of the protocol. Due to time
limitations, the most important information will be covered.***
4
Methodology of Instruction
A higher level of certification can perform all of the
procedures that a lower lever of certification is allowed to
perform.
The protocol has been written to promote “critical thinking”
5
Stipulations
Protocol is for use by individuals operating under the GMVEMSC
Drug Box Exchange and properly certified by the State of Ohio
Nothing by be done without pre-approval of the Medical Director for
the local agency
Recipe-style adherence to specific protocols may not be in the
patient’s best interest.
No protocol can substitute for the EMS professional’s judgment.
Never should treatment options exceed those authorized without
direct consultation with Medical Control
7
2015 Changes
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
♦
Changed all references to Intermediate to AEMT
♦
Recommends manual B/P in patients with s/s of shock
♦
Removed most of the contraindications to drug administration within
the protocol
♦
Drug Bags may only be exchanged within the same department
♦
Added Ambulance Restocking policy
♦
Added Protocol Testing Compliance
♦
Made slight changes to the Hospital Capabilities & Phone number lists
♦
Added additional requirements to the Drug Bag Program
9
2015 Changes
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
♦
SMR applies to all age patients (if <3 y/o with a GCS <15, then
immobilize)
♦
SMR for patients > 70 y/o should include a C-collar
♦
Deleted all references to remove or manage an insulin pump
♦
Recommends transporting all CVA patients flat
♦
Added additional APGAR at 10 minutes
♦
Mention cold water submersion for cooling heat stroke patients
♦
Added EMT & EMR administered Narcan, only EMT may repeat
10
2015 Changes
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
♦
Added 1 mcg/kg IN admin. to Pediatric Fentanyl (max 100 mcg)
♦
Pediatric Midazolam changed to 0.2 mg (max. 4 mg) for IN/IM
♦
Under Chemical Restraint, removed MCP orders for initial dose
for Midazolam
♦
Added 1 mcg/kg IN admin. to Pediatric Fentanyl (max 100 mcg)
♦
Added crush protocol
♦
Removed “last resort” verbage to IM Midazolam
♦
Asthmatic condition added to indication for CPAP
11
2015 Changes
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
♦
Renal patients with wide complex bradycardia may
need hyperkalemia therapy
♦
Pediatric Midazolam changed to 0.1 mg (max. 2 mg)
♦
Added pediatric dose of Hydroxocobalamine
♦
Replaced Dopamine with Norepinephrine throughout
the protocol
12
Communicating with the Hospitals
Reasons to call hospital
Prepare the receiving facility for the arrival
To obtain orders
To obtain advice
When calling:
Paint a clear picture
If trauma, include MIVT, ETA, GCS and findings
If consultation is required, ask for Medical Control
Call after transmission of any EKG, Paramedics do not have to
transmit (should only do so for advice)
When calling for an alert, say “We recommend a __________
Alert”
14
Communicating with the Hospitals
Hospitals that request notification on every patient:
15
Children’s Medical Center (CMC)
Maternity at Good Samaritan
Maternity at Miami Valley Hospital
Springfield Regional Medical Center
Soin Medical Center
VA Medical Center
Wayne Hospital
McCullough-Hyde Hospital
WPAFB Medical Center
Non-Initiation of Care
♦
Resuscitation won’t be initiated in the following circumstances:
Deep, penetrating, cranial injuries
Massive truncal wounds
DNR Order - present and valid
Frozen body
Rigor mortis, tissue decomposition, or dependent post-mortem lividity
Triage demands
Pediatric patients may meet criteria
If care began and it is readily apparent to EMS that the patient
met non-initiation of care criteria, resuscitation efforts may
cease.
Continued…
16
Non-Initiation of Care
Resuscitation will not be initiated in the following
circumstances:
Blunt trauma found in cardiac arrest unless one of the
following conditions are present:
Patient can be delivered to an emergency department in 5
minutes
If the arrest is caused by a medical condition
Focused blunt trauma to the chest (Commotio Cordis)
Continued…
17
Non-Initiation of Care
Resuscitation will not be initiated in the following
circumstances:
Penetrating trauma found in cardiac arrest when the patient
cannot be delivered to an emergency department within 15
minutes.
Resuscitation will be initiated on victims of penetrating
trauma who arrest after they are in EMS care
Once en route, continue care even if the above time limits
cannot be met.
18
Do-Not-Resuscitate
Continued…
19
Do-Not-Resuscitate
DNR-Comfort Care (CC)
Permits any medical treatment to diminish pain or
discomfort that is not used to postpone the patient’s death
The following treatments are permitted:
Suctioning
Oxygen
Splinting/Immobilization
Control bleeding
Pain control
Continued…
20
Do-Not-Resuscitate
DNR-Comfort Care (CC)
Permits any medical treatment to diminish pain or discomfort
that is not used to postpone the patient’s death
The following treatments are not permitted:
Chest compressions
Airway adjuncts (including CPAP)
Resuscitative drugs
Defibrillation/cardioversion/monitoring
Respiratory assistance (oxygen, suctioning are
permitted)
Continued…
21
Do-Not-Resuscitate
DNR-Comfort Care Arrest (CCA)
Permits any medical treatment until the patient goes into
cardiac or respiratory arrest
Any appropriate standing orders treatment until cardiac or
respiratory arrest/agonal breathing occurs.
Continued…
22
Do-Not-Resuscitate
DNR-Comfort Care Arrest (CCA)
Note: When a Durable Power of Attorney for Healthcare
(DPA-HC) is present and the “Living Will and Qualifying
Condition” box is checked, the DPA-HC cannot override the
patient’s DNR status.
A patient may change their DNR status at anytime verbally,
in writing or action.
23
= EMR
Field Termination
= EMT
= AEMT
= Paramedic
Italics = MCP
When a patient has failed to respond to ALS, it may be decided to
terminate the effort
The following criteria must be met:
Patient 18 years or older
Patient in asystole or PEA
If PEA rate above 40, then consider resuscitation
Not be in arrest due to hypothermia
Patient has an advanced airway
Patient has vascular access
Contact medical control directly to receive consent for termination
Field Termination doesn’t apply to Pediatrics
24
Continued…
= EMR
Field Termination
= EMT
= AEMT
= Paramedic
Italics = MCP
Field Termination with no ALS Equipment
If no ALS equipment is available at the scene, and transport
time to a medical facility will exceed 20 minutes, consider field
termination
Must be 18 years or older
Must not be in arrest due to hypothermia
Contact MCP directly to receive consent for termination
Continued…
25
Field Termination
This section does not apply to Emergency Medical
Responders
The intent of this section is to avoid the risks of emergency
transport of patients who are almost certainly non-viable.
Ensure that the EMS Coordinator of the hospital that
authorized the Field Termination receives a copy of the run
sheet for his/her records.
26
= EMR
Initial Care
= EMT
= AEMT
= Paramedic
Italics = MCP
Follow basic life support algorithms as indicated based on current
AHA guidelines
Obtain chief complaint (OPQRST), SAMPLE history, and vital
signs per patient condition
Monitoring devices pulse oximeter, etc. as appropriate
Patient with IV pump experiencing an allergic reaction:
discontinue only after receiving approval from MCP otherwise,
maintain pump
Bring meds or list with dose and frequency
Continued…
27
= EMR
Initial Care
Cardiac monitor
IV of Normal Saline (NS) or a Saline Lock (SL)
IVs:
Shock:
= EMT
= AEMT
= Paramedic
Italics = MCP
Run wide-open.
Decrease fluid rate if SBP >100.
IV NS, 20 ml/kg
Medical Emergencies, Head Trauma, Cardiac Problems (with stable BP):
Use TKO rate
Slow IV Meds means over 2 minutes
Any IV Med can be given IO
Adult IO devices
28
Continued…
Initial Care
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
IO Devices
Use when patient is hemodynamically unstable or
unresponsive
When less invasive methods aren’t available. (IM or IN)
Lidocaine 1.5 mg/kg, IVP up to 100 mg via the IO
2% Lidocaine – 0.5 mg/kg IO
Utilize Central venous catheters, dialysis catheters, fistulas,
or grafts if in cardiac arrest, profoundly unstable or rapidly
deteriorating
29
Spinal Immobilization
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Blunt trauma
All patients with clinical indications of a spinal injury and/or with
altered levels of consciousness must be immobilized with both a
C-Collar and a spinal immobilization device
Other alert trauma patients can have a C-Collar placed and
moved in-line as a unit to the cot. Including:
30
Neck pain or spinal tenderness
Pain on motion of the neck
Age > 70
High risk mechanism (high speed MVC, fall > 10 ft, axial loading injury)
Patients who are ambulatory may ambulate to the cot
Spinal Immobilization
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Penetrating trauma
Patients with penetrating trauma to the torso or neck with focal
neurological signs or paralysis should be immobilized in a c-collar and
with a spinal immobilization device.
Patients without focal neurological signs or paralysis need NOT be
immobilized.
Delays in transport for immobilization are to be minimized
This protocol applies to all patients
Those patients < 3 y/o with a GCS of < 15 should be fully immobilized
31
Spinal Immobilization
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Airway Management
Patients who are immobilized and require airway and / or ventilatory
intervention (including intubation) may have the collar removed, with inline stabilization performed during the intervention.
The collar should then be reapplied.
Patients who do not tolerate immobilization should have it adjusted
to the point of removal if necessary
32
Pain Control
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Prehospital pain management is important. It reduces time to pain
relief, avoids exacerbation of pain during movement and transport,
is compassionate, and is good medical care
Use ice packs, position of comfort, and splinting to reduce pain as
indicated
This protocol is for management of acute moderate to severe pain,
it is NOT for treatment of exacerbations of chronic pain
Call for orders for narcotics for pain from a chronic condition
Document pain at initial contact, during treatment and after
intervention
MCP approval required before administration of Fentanyl in
pediatric patients with abdominal pain
33
Pain Control
If patient is alert, Fentanyl 50 mcg slow IVP
May repeat Fentanyl 50 mcg slow IVP after 5 min.
Maintain SBP >100
If no IV, give Fentanyl 50 mcg IM or Fentanyl 100 mcg IN
Repeat dose of Fentanyl 50 mcg IM (repeat after 30 min.)
IN Fentanyl may be repeated (if a second drug box is available)
NO FENTANYL TO ANYONE < 2 YEARS OF AGE
Consider Fentanyl 1 mcg/kg, slow IV (max dose 50 mcg)
May repeat Fentanyl 1 mcg/kg (max 50 mcg), slow IVP after 5 minutes
Maintain appropriate normal SBP
If no IV, give Fentanyl 1 mcg/kg IM (max dose 50 mcg).
Repeat dose of Fentanyl 1 mcg/kg IM (max dose 50 mcg, repeat after 30 min.)
Or if no IV, give Fentanyl 1/mcg/kg IN (max dose 100 mcg)
34
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Airway Maintenance
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
O2 PRN. Use the following rates as guidelines:
2 LPM by NC for patient with COPD
4 - 6 LPM by NC for other patients
12 - 15 LPM by NRB for severe trauma patients, distressed cardiac
patients, patients with respiratory distress, or patients who appear to
need high flow O2
Ventilate patients who are symptomatic with an insufficient
respiratory rate/depth
If indicated and approved, utilize a “Rescue Airway”
35
Airway Maintenance
Intubate for respiratory arrest with appropriate airway device
Decompress tension pneumothorax
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
If awake consider:
Lidocaine Jelly to the ET tube
Lidocaine, 100 mg IN {half dose per nostril} or nebulized
Lidocaine, 1.5 mg/kg IN or neb. with 8-10 LPM O2 ,max dose 100 mg
If resisting and SBP >100, consider Midazolam, 2 mg slow IVP
Midazolam, 0.1 mg/kg slow IVP (max dose 2 mg)
36
= EMR
Airway Maintenance
= EMT
= AEMT
= Paramedic
Italics = MCP
Sedate to Intubate
Lidocaine 100 mg, IVP in suspected CVA, intracranial hemorrhage,
head injury, or signs of increased intracranial pressure
Etomidate 0.3 mg/kg, IVP (average initial dose is 15-25 mg).
Repeat initial dose within 2 minutes.
Or Ketamine 100 mg IV. May repeat within 5 min.
Or Ketamine 500 mg IM (2 doses of 250 mg), may repeat in 5 min.
After the jaw relaxes (30-60 seconds), intubate
After Intubation, if the patient is still resisting, and SBP is >100,
administer Midazolam 2 mg IVP over 2 min
Continued…
37
Confirmation Devices
38
Colormetric ETCO2 Detector
Limitations
The patient must have adequate perfusion.
May be useful for patients in cardiac arrest if color change is
present.
Secretions, emesis, etc., can ruin the device.
Large amounts of carbonated beverage give a false positive.
Use the device for no more than two hours.
Continued…
39
Colormetric ETCO2 Detector
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Medication Issues:
If you administer medications via ETT, remove the EtCO2
detector for several ventilations, until no medication returns
through the tube during exhalation.
Medications splashing up the tube can alter color change.
Intravenous sodium bicarbonate will produce more carbon
dioxide resulting in enhanced color.
40
Capnography
Measures the amount of carbon dioxide in the exhaled ventilations of
patients.
Can be used with patients who are not intubated.
In-line EtCO2 monitors can be used on patient with or without adequate
perfusion.
Electronic monitors are more sensitive therefore changes can be seen
in real time.
Is considered the “Gold Standard” and should be used every time if
you have the equipment
41
Esophageal Detector Device
Limitations:
A large amount of gastric air and late term pregnancy can give a
false positive finding
A cold device may give a false negative result.
Can only be used on ETT
Cannot be used continuously.
May only be used on patients who are > 5 y/o and weigh at least 20
kg/44 pounds.
42
= EMR
IO Insertion
= EMT
= AEMT
= Paramedic
Italics = MCP
♦
Use of IO devices is limited to patients who are unresponsive or
hemodynamically unstable; and then, only when less invasive
means are ineffective or not available
♦
For an adult in cardiac arrest, the preferable order of vascular
access:
♦
♦
♦
♦
♦
External Jugular IV
Antecubital IV
Proximal Humeral IO
Last resort, Proximal Tibial IO
Pediatrics, < 8 y/o use Tibial IO
43
Adults
Pediatric
Arrest:
Humerus
Tibia
Non-arrest:
Tibia
Tibia
IO Insertion
44
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
IO Insertion
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
IO Insertion at Proximal Tibia Site
Identify the tibial tuberosity
Prep the skin and insert needle according to manufacturer’s directions.
Use 10-15O caudal angulation to further decrease risk of hitting growth
plate.
Needle will stand up on its own with proper placement.
Attach syringe and aspirate bone marrow (to further confirm
placement).
Connect the IV line. If flow is good and extravasation is not evident
secure needle with gauze pads and tape.
A pressure bag may facilitate infusion.
Lidocaine 1.5 mg/kg up to 100 mg via IO for pain associated with IO
Lidocaine 2% 0.5 mg/kg (max 100 mg) via IO for pain
45
= EMR
IO Insertion
= EMT
= AEMT
= Paramedic
Italics = MCP
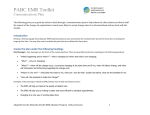
Acromion
Coracoid Process
Greater Tuberosity
46
IO Insertion
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
IO Insertion at Humeral Head site
Position patient so shoulder is adducted (moved toward the middle of
the body) and the greater tuberosity is most prominent by lying patient
supine, arm at their side with palm on their navel.
Prep the skin and insert needle according to manufacturer’s directions.
Insert the needle at 90-degree angle directly into the greater tuberosity.
Needle will stand up on its own with proper placement.
Attach syringe and aspirate bone marrow (to further confirm
placement).
Connect the IV line. If flow is good and extravasation is not evident
secure needle with gauze pads and tape.
A pressure bag may facilitate infusion.
47
Alternative Venous Access
Central Venous Catheter
48
Internal Dialysis Fistula
Central Venous Catheters
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Central catheter: Catheter placed through chest wall.
Distal portion of catheter is external with access ports.
Subcutaneously Implanted Port: Device surgically placed under the
skin on the chest. No external access. Do not use!
PICC Line: Catheter placed in arm. Distal portion of catheter is
external with access port.
Do not force fluids or drugs through the device
D10 by PICC is preferable to IM Glucagon.
Paramedics are only permitted to access central catheters and PICC
lines, not subcutaneously implanted ports.
49
Central Venous Catheters
Direct access can result in the following complications:
Air Embolism:
Clamp before attaching the syringes
Clamp before removing the syringes.
Heparin Bolus: Remove 5 cc of blood before using
Catheter Damage: Use a 10 cc syringe or bigger
After draw, bolus 10 cc NaCl in pulsating manner
Do not use catheter if no blood return.
50
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Internal Dialysis Fistula
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Artificial passage between an artery and a
vein used to gain access to the bloodstream for
hemodialysis.
Usually located in the inner aspect of the patient's forearm
resulting in a bulge under the skin that should be visible or
easily palpated.
In cardiac arrest or the profoundly unstable/rapidly
deteriorating patient, a dialysis fistula, may be accessed to
administer IV fluids or medication.
51
Internal Dialysis Fistula
Accessing the Fistula
Utilize an aseptic technique
Be careful not to puncture the back wall of the vessel.
Use pressure bag for infusion.
Blood may still backup in the IV tubing.
Increased risk of hemorrhage because of regular use of
anticoagulants during hemodialysis.
Control bleeding with direct pressure.
52
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Cardiac Arrest: Treatable Causes
Treatable causes include:
Hypoxia
Hypovolemia
Hypo/Hyperkalemia
Hypoglycemia
Hydrogen Ion (acidosis)
Hypothermia
53
Trauma
Thombosis
Toxins
Tamponade, (Cardiac)
Thrombosis, (Coronary & Pulmonary)
Tension Pneumothorax
CA: Renal Dialysis
Calcium Chloride 10% (1,000 mg)
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Calcium Chloride 10% 0.2 ml/kg (20 mg/kg) (max 500) slow
IVP
Flush IV line thoroughly between Calcium and
Sodium Bicarb.
Sodium Bicarbonate, 100 mEq IVP
Sodium Bicarbonate, 1 mEq/kg slow IVP
54
= EMR
CA: Smoke Inhalation or Cyanide
♦
= EMT
= AEMT
= Paramedic
Italics = MCP
For smoke inhalation or cyanide poisoning
♦ Administer Hydroxocobalamin, 5 gm slow IV, over 15 min.
♦ DO NOT ADMINISTER both Hydroxocobalamin and other cyanide antidotes to
the same patient.
♦ Pedi dose is 70 mg/kg IV, max dose 5000 mg
♦ May repeat Pedi dose 35 mg/kg IV, max dose 2500 mg
♦ Sodium Thiosulfate 12.5 gm (50 ml) slow IVP
♦ >25 kg - 12.5 gm (50 ml) slow IVP
♦ <25 kg – 1.65 ml/kg (412.5 mg/kg) (50 ml) slow IVP
♦
Antidotes are no longer in Drug Bags. They are in multiple
caches in the region.
♦ Contact 937-333-USAR (8727)
♦ Call if: Reported victim trapped, known cyanide event, or Mayday scenario
♦
No MCP orders needed if patient in Cardiac Arrest
55
CA: V-fib/Pulseless V-tach
If unwitnessed arrest, CPR for 2 minutes,then AED
If witnessed arrest, AED immediately
Continue CPR and AED
Consider treatable causes
First Defib @ 360 J (or biphasic equivalent)
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
If witnessed, if not then 2 min CPR first
Defibrillate 2 j/kg(or biphasic equivalent)
Continued…
56
CA: V-fib/Pulseless V-tach
♦
Uninterrupted, Continuous CPR throughout the Code
♦
Second Defib @ 360 J (or biphasic equivalent)
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
♦ Defibrillate 4 j/kg(or biphasic equivalent)
♦
Epinephrine 1 mg, IV/IO repeat every 3-5 minutes
♦ If no IV Epi 2mg ETT q 3-5 minutes (11 ml total)
♦ Epi 0.01 mg/kg, IV/IO or Epi 0.1 mg/kg, ETT
♦
Third Defib @ 360 J (or biphasic equivalent)
♦ Defibrillate 6 j/kg(or biphasic equivalent)
Continued…
57
CA: V-fib/Pulseless V-tach
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Amiodarone 300 mg, IV/IO or Lidocaine, 1.5 mg/kg ETT
Amiodarone 5 mg/kg (Max. 300 mg), IV/IO or Lidocaine, 1.5 mg/kg ETT
Fourth Defib @ 360 J (or biphasic equivalent)
Defibrillate 8 j/kg(or biphasic equivalent)
Repeat Amiodarone 150 mg or Lidocaine 0.75 mg/kg ETT
Repeat Amiodarone 5 mg/kg (Max. 150 mg), IV/IO or Lidocaine, 0.75
mg/kg ETT (Max. 100 mg)
Fifth Defib @ 360 J (or biphasic equivalent)
Defibrillate 10 j/kg(or biphasic equivalent)
Continued…
58
CA: V-fib/Pulseless V-tach
♦
Continue CPR and repeat treatment as indicated
♦
12-lead EKG if return of spontaneous circulation
♦ If AMI, transport to Interventional Cath Center
♦
If no anti-arrhythmic has been given:
♦ Amiodarone, 150 mg IV over 10 minutes
59
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
= EMR
CA: Asystole/PEA
= EMT
= AEMT
= Paramedic
Italics = MCP
♦
If unwitnessed arrest, CPR for 2 minutes, then AED
♦
If witnessed arrest, AED immediately
♦
Continue CPR and AED
♦
Uninterrupted, Continuous CPR throughout the Code
♦
Consider treatable causes
Continued…
60
CA: Asystole/PEA
Epinephrine 1 mg, IV/IO repeat every 3-5 minutes
If no IV Epi 2mg ETT q 3-5 minutes (11 ml total)
Epi 0.01 mg/kg, IV/IO or Epi 0.1 mg/kg, ETT
Consider Atropine 1mg, IV/IO for Asystole or slow PEA
Repeat every 3-5 minutes up to 3 doses
12-lead EKG if return of spontaneous circulation
If AMI, transport to Interventional Cath Center
Consider Field Termination
61
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Therapeutic Hypothermia
Should be initiated during the CPR process
Trauma is a contraindication
Do not start if pt. is hypothermic (<34 C or 93.2 F)
Do not start if pt. is conscious
Place ice packs in axilla, groin (bilaterally) and neck
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Change ice packs every 15 min
Complete a neuro exam including GCS and Pupils
62
Continued…
Therapeutic Hypothermia
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Chilled IV bolus to a max. of 2 L rapidly
Administer medications in a normothermic IV
Notify Hospital so they are ready to continue cooling
If SBP remains < 100, Norepinephrine drip at 30 gtts/min titrate to BP
4 mg added to 250 ml bag, 60 gtt tubing
Max dose 44 gtt/min
Treat shivering
Midazolam 5 mg slow IVP
Etomidate 0.3 mg/kg (20 mg max)
63
Therapeutic Hypothermia
♦
CLINICAL PEARLS
♦ Protocol begins with a patient in Cardiac Arrest
♦ Inclusion Criteria
♦ Arrest not related to Trauma or hemorrhage
♦ Age 16 or older
♦ Advanced airway in place with EtCO2 > 20
♦ Do not hyperventilate, patients may develop metabolic alkalosis
♦ If no advanced airway, cooling only with MCP orders
♦ GSC less than 8 (no purposeful response to pain)
♦ For patients < 16 y/o, contact MCP
64
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
= EMR
Chest Pain
= EMT
= AEMT
= Paramedic
Italics = MCP
ASA, 324 mg to patient with symptoms of ACS, >25 y/o
Patient MUST CHEW the Aspirin
Do not administer if pregnant patient is in 3rd Trimester
Basics need MCP permission to access drug bag
Administer Nitro tabs 0.4 mg SL every 5 minutes x 3
If SBP >100, and the patient is > 25 years old
Vital signs between doses
EMTs need MCP permission to access drug bag or give more than one
dose of patient’s NTG
Do not administer if Patient admits to the use of Viagra, Cialis, Levitra,
Revatio or similar drugs in the last 24 hrs.
Establish IV access prior to admin if patient has never had Nitro
Continued…
65
= EMR
Chest Pain
= EMT
= AEMT
= Paramedic
Italics = MCP
12 Lead EKG, (EMT & AEMT must transmit to MCP)
Transmit with at least two patient identifiers
For EMT & AEMT, MCP will make transport decision
Include patient’s cardiologist by name in verbal assessment
Consider Fentanyl, 50 mcg slow IVP
Do not wait for 3 Nitro admin for pain management
Repeat Fentanyl, 50 mcg slow IVP after 5 min.
If no IV Fentanyl, 50 mcg IM
Repeat Fentanyl, 50 mcg IM no sooner than 30 minutes if transport
time is > 30 minutes.
Continued…
66
= EMR
Chest Pain
= EMT
= AEMT
= Paramedic
Italics = MCP
IV NS, up to 500 ml may be administered with SBP
<100 without pulmonary edema.
With evidence of RVI, contact MCP for fluid bolus
If evidence of AMI, transport to interventional facility
Repeat 12 Lead EKGs throughout transport
Continued…
67
Acute Myocardial Infarction
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Inferior Wall MI (II, III, aVF)
Capture Lead V4R
Treat hypotension with a fluid challenge
Administer NTG or Fentanyl with caution.
If 2 type II or 3 block, prepare to pace immediately
Consider Atropine, 0.5 mg IVP (max 3 mg)
Set pacer @ 70 bpm, 20 mA increase till capture
Consider Midazolam 2 mg slow IVP
If SBP remains < 100, Norepinephrine drip at 30 gtts/min titrate to
BP (max 44 gtts/min)
Continued…
68
Acute Myocardial Infarction
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Anterior Wall MI (V1-V4)
ST elevation in 2 or more leads at high risk for death
High risk for CHF or Cardiogenic shock
o
May develop BBB, PVC or 3 Block
If SBP remains < 100, Norepinephrine drip at 30 gtts/min
titrate to BP (max 44 gtts/min)
Lateral Wall MI (I, aVL, V5, V6)
May have some LV dysfunction, but not as severe as Anterior
May also develop AV Nodal Block
69
Interventional Facilities
♦
♦
♦
♦
♦
♦
♦
♦
Atrium Medical Center
Kettering Medical Center
Good Samaritan Hospital
Miami Valley Hospital
Grandview Hospital
Springfield Regional Medical Center
Southview
Reid Memorial Hospital
70
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Cardiac Dysrhythmias
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Bradycardia
Wide-complex bradycardia in a renal patient may need 1 amp Calcium
Chloride for hyperkalemia
For adequate perfusion, observe and monitor.
Consider 12 Lead EKG & Transmit
Transport unless ALS is < 5 min. away
For poor perfusion,
Consider Atropine, 0.5 mg IVP up to 3 mg
Set at 70 BPM, 20 mA and increase until mechanical capture
Consider Midazolam, 2 mg IVP
71
Cardiac Dysrhythmias
Bradycardia
For adequate perfusion, observe, monitor vital signs, and
apply oxygen if needed.
For poor perfusion:
Perform CPR if HR < 60/min
Epi (1:10,000) 0.01 mg/kg, IV/IO or
Epi (1:1,1000) 0.1 mg/kg, ETT every 5 minutes
72
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Cardiac Dysrhythmias
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Bradycardia
If AV Block
Consider Atropine 0.02 mg/kg
Minimum dose 0.1 mg
Maximum dose 0.5 mg
May repeat dose (total max. dose – 1.0 mg)
Consider pacing at 80 bpm
Pedi pads for patients <15 kg
Consider Midazolam, 0.15 mg/kg (Max. 4 mg) IVP over 1-2 minutes
Start at 5 mA and increase to 200 mA
73
Cardiac Dysrhythmias
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Tachycardia
For adequate perfusion, observe and monitor.
Consider 12 Lead EKG & Transmit
Transport unless ALS is < 5 min. away
Continued…
74
Cardiac Dysrhythmias
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Stable Tachycardia
Narrow Complex – Regular
Vagal maneuvers
Adenosine, 6 mg rapid IVP
If patient advises it takes 12 mg of Adenosine, then administer Adenosine, 12 mg
rapid IVP
May repeat Adenosine, 12 mg rapid IVP x 2
Continued…
75
= EMR
Cardiac Dysrhythmias
= EMT
= AEMT
= Paramedic
Italics = MCP
Stable Tachycardia
Wide Complex – Regular
Amiodarone, 150 mg IV over 10 minutes
Infuse in a 250 Nacl bag
18 g Needle
Use 60 gtt tubing wide open
Wide Complex – Irregular
Consider Amiodarone, 150 mg IV over 10 minutes
Continued…
76
Cardiac Dysrhythmias
Unstable Tachycardia
Cardioversion 100 J, 200 J, 300 J, 360J
Or biphasic equivalent
Consider Midazolam, 2 mg IVP
77
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Cardiac Dysrhythmias
Stable or Unstable Tachycardia
Vagal Maneuvers (blow through straw or O2 tubing)
Unstable Tachycardia
Adenosine, 0.1 mg/kg rapid IVP (Max. 6 mg)
Repeat Adenosine, 0.2 mg/kg rapid IVP (Max. 12 mg) x2
Cardioversion 1 j/kg followed by 2 j/kg
Consider Midazolam, 0.15 mg/kg (Max. 4 mg) slow IVP
78
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Non-Traumatic Shock
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Without Pulmonary Edema
No JVD, edema, or rales noted
NS, 500 ml IV bolus, repeat if needed
NS, 20 ml/kg IV bolus titrated to perfusion, repeat if needed
For persistent shock, additional vascular access.
If SBP remains < 100, Norepinephrine drip at 30 gtts/min titrate to BP
(max 44 gtts/min)
Continued…
79
Non-Traumatic Shock
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
With Pulmonary Edema
JVD, edema, or rales present
Consider NS, 250 ml IV bolus
Treat arrhythmias as indicated.
If SBP remains < 100, Norepinephrine drip at 30 gtts/min titrate to
BP (max 44 gtts/min)
80
Non-Traumatic Shock
Exsanguinating Hemorrhage
Vascular access(es) NS to maintain SBP ~100 en route to ED
Do not get SBP too high
NS, 20 ml/kg IV bolus titrated to perfusion, may repeat x2
81
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
= EMR
Stroke
= EMT
= AEMT
= Paramedic
Italics = MCP
Complete GMVEMSC Prehospital Suspected CVA/TIA
Checklist.
If signs of cerebral herniation
Ventilate at a rate of 20 respirations per minute
Ventilate at a rate of 10 faster than normal
If available, ventilate at EtCO2 readings of 30 mmHg
Complete Cincinnati Prehospital Stroke Scale.
Facial Droop (patient shows teeth or smiles).
Arm Drift (patient closes eyes and holds both arms straight out)
Abnormal Speech (have patient say a phrase)
Continued…
82
= EMR
Stroke
= EMT
= AEMT
= Paramedic
Italics = MCP
If glucose <60, or there is strong suspicion of hypoglycemia
despite glucometer readings
D10, IV 250 ml at wide open rate
D10, 5 ml/kg IVP, maximum single dose of 250 ml
D10 may be repeated in 10 min. if BSL <60
If unable to establish vascular access, Glucagon, 1 mg IM
Strongly consider transport to a Stroke Center
If symptoms occurred >4 hours and <8 hours from last time they
were known to be free of stroke symptoms
If patient wakes with symptoms
Continued…
83
Stroke
Contact MCP with a Stroke Alert and for advice regarding
destination if greater than 8 hrs since last seen normal
Transport the pt. with the bed flat to increase cerebral
perfusion.
Transport historian with patient for pt. history and for
permissions
Complete the “EMS CHECKLIST: SUSPECTED
Stroke/CVA/TIA” for every stroke/TIA patient.
84
Stroke
Interventionl Facilities:
Miami Valley Hospital
Kettering Medical Center
Symptoms mimicking stroke
85
Seizures
Subdural hematoma
Brain tumor
Syncope
Toxic or metabolic disorders (i.e., hypoglycemia)
Trauma
General Considerations
Scene size-up, with rapid assessment and recognition of
major trauma/multiple system trauma and effective
evaluation of the mechanism of injury are essential to the
subsequent treatment.
Hypothermia is a significant and frequent problem in shock
for major trauma patients. Maintain patient’s body
temperature.
When patient is transported by helicopter, the EMS run
sheet should be faxed to the receiving trauma center.
86
Trauma
♦
General Considerations
♦ The only procedures that should take precedence to
transport of major trauma patients are:
♦ Airway management
♦ Stabilization of neck/back or obvious femur and pelvic fractures
on a backboard
♦ Exsanguinating hemorrhage control
♦ Extrication
♦ Notification of the receiving facility is essential
♦ Give Mechanism of Injury, Injuries, Vital signs, Treatment
(MIVT), GCS with components, and ETA.
87
Head Injury
♦
Evaluate patient condition:
♦ Level of Consciousness
♦ Pupillary size and reaction
♦ Glasgow Coma Scale
♦
Ventilate at 20 BPM (10 BPM faster than normal) when the
signs of cerebral herniation are present:
♦ Blown or unequal pupil(s)
♦ Bradycardia
♦ Posturing
♦ Decreased mental status
♦
Ventilate to maintain EtCO2 readings of 30 mmHg
88
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
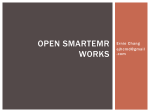
Glasgow Coma Score
< 2 Years Old
Eyes
Verbal
Motor
89
Adult & Peds >2 y/o
Spontaneously
4
Spontaneously
4
To Voice
3
To Voice
3
To Pain
2
To Pain
2
No Response
1
No Response
1
Coos, Babbles
5
Oriented
5
Irritable Cry, Consolable
4
Confused
4
Cries to Pain
3
Inappropriate Words
3
Moans to Pain
2
Grunts, Garbled Speech
2
No Response
1
No Response
1
Normal Movements
6
Normal Movements
6
Withdraws to Touch
5
Localizes Pain
5
Withdraws to Pain
4
Withdraws to Pain
4
Flexion (Decorticate)
3
Flexion (Decorticate)
3
Extension (Decerebrate)
2
Extension (Decerebrate)
2
No Response
1
No Response
1
= EMR
Extremity Fracture, Dislocations, Sprains
= EMT
= AEMT
= Paramedic
Italics = MCP
Assess pulse, motor and sensation before/after
splinting and during transport.
For open fractures, control bleeding with direct pressure and
cover with dry, sterile dressing.
Apply appropriate splinting device.
To reduce swelling, elevate extremity and apply ice
Consider Pain Control Protocol
90
Continued…
Crush Syndrome Trauma
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
History – Entrapped or under extreme load for >60 min
1 liter NaCl bolus IV. Then 500 ml/hour IV
NaCl, 20 ml/kg IV
Follow pain management protocol
If hypotensive and the patient has been entrapped > 1 hr:
Give additional NaCl, 1 Liter IV.
Give additional NaCl, 20 ml/kg IV
12 lead EKG
91
Crush Syndrome Trauma
= EMT
= AEMT
= Paramedic
Italics = MCP
Normal ECG/hemodynamically stable, immediately prior
to extrication:
Sodium Bicarb 100 mEq IV
Sodium Bicarb 1mEq/kg IV
= EMR
Abnormal ECG/hemodynamically unstable:
If after release, there are EKG changes consider Calcium
Chloride
Peaked T waves with a QRS > 0.12 seconds.
QT ≥0.46 seconds.
Loss of P-wave.
Sodium Bicarb 100 mEq IV
Sodium Bicarb 1mEq/kg IV
92
Crush Syndrome Trauma
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Consider Midazolam 2 mg IV
0.1 mg/kg IV, max dose of 2 mg
Special considerations:
Potential for multiple system trauma
Potential for hypo/hyperthermia.
Hyperkalemia from crushed syndrome can produce ECG
changes, and may also cause a bizarre wide complex
rhythm.
93
= EMR
Hypothermia
= EMT
= AEMT
= Paramedic
Italics = MCP
Move patient to warm environment
Remove all wet clothing
Dry the patient
Cover with blankets.
Avoid any rough movement that may cause cardiac dysrhythmias.
It may be beneficial to immobilize the patient on the backboard.
Assess neurological status.
94
Continued…
= EMR
Hypothermia
= EMT
= AEMT
= Paramedic
Italics = MCP
It may be necessary to assess pulse and respirations
for up to 30-45 seconds to confirm arrest.
Consider possibility of other medical conditions (i.e. overdose,
hypoglycemia, CVA)
Transport to a trauma center.
Use the least invasive means possible to secure airway. Intubate if
necessary, as gently as possible.
Complete the following steps during transport:
Establish vascular access and consider warmed fluids
Treat bradycardia only if it is profound
Do not initiate CPR if there is a pulse, no matter how slow
95
Continued…
Hypothermia
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
If patient arrests:
CPR continuously
If severe hypothermia (<86F (30C)) is strongly suspected, limit
defibrillation attempts to 1 and withhold medications/defibrillations
except on orders from Medical Control
If body temperature is >86F (30C), follow normal arrest protocols
Intubate and oxygenate the patient with warmed and humidified
100% O2
Continue resuscitative efforts while in transit, even if there is no
response
96
Frostbite
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Protect injured area(s)
Remove clothing and jewelry from injured parts.
Do not attempt to thaw injured part with local heat.
Maintain core temperature.
Severe frostbite injuries should be transported to a burn center.
Consider vascular access with {warmed} fluids
Consider Pain Control Protocol
97
Continued…
Burns/Smoke Inhalation
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Keep patient warm.
Superficial and partial thickness burns <10% may have wet
dressings applied.
Cover burn areas with clean, dry sheets or dressings after
cooling burns <10% first
Remove clothing and jewelry from injured parts
CO Oximeter (if available)
5-12 PaCO in a non-smoker needs monitoring
Over 12 PaCO is significant
98
Continued…
= EMR
Burns/Smoke Inhalation
= EMT
= AEMT
= Paramedic
Italics = MCP
Do not remove items which have adhered to the skin
Radiation burns:
Treat as thermal burns
Except when burn is contaminated with radioactive source
Then treat as Hazmat situation
Consider contacting Haz-Mat team for assistance in
contamination cases
Continued…
99
Burns/Smoke Inhalation
Inhalation Burns:
Provide O2 {humidified with Saline}
If no humidifier is available, administer a Saline Nebulizer, 3 ml.
Repeat PRN
Provide early endotracheal intubation as indicated
Sodium Thiosulfate, 12.5 gm (50 ml) if Cyanide is possible
>25 kg - 12.5 gm (50 ml) slow IVP
<25 kg – 1.65 ml/kg (412.5 mg/kg) (50 ml) slow IVP
Or Hydroxocobalamin (Cyanokit), 5grams, via slow IV infusion
Pedi dose is 70 mg/kg IV, max dose 5000 mg
May repeat Pedi dose 35 mg/kg IV, max dose 2500 mg
100
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Burns/Smoke Inhalation
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Antidotes are no longer in Drug Bags. They are in multiple caches
in the region.
Contact 937-333-USAR (8727)
Call if: Reported victim trapped, known cyanide event, or Mayday scenario
No MCP orders needed if patient in Cardiac Arrest
Hydroxocabalamin considerations
Do not administer both Cyanokit and other antidotes
Administer in separate IV line when possible
Control seizure activity with Diazepam or Midazolam
Continued…
101
Burns/Smoke Inhalation
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Consider Hyperbaric Treatment for the following:
Underlying cardiovascular problems
Symptoms such as chest pain or shortness of breath
> 60 years of age
Obvious neurological symptoms, such as any interval of
unconsciousness, loss of time, inability to perform simple motor
tasks, or loss of memory
Smoke inhalation victims
Pregnancy
102
Carbon Monoxide Poisoning
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Provide high flow O2 to all suspected CO poisonings
SpO2 readings will be falsely high
CO Oximeter (if available)
5-12 PaCO in a non-smoker needs monitoring
Over 12 PaCO is significant
103
Carbon Monoxide Poisoning
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Consider Hyperbaric Treatment for the following:
Underlying cardiovascular problems
Symptoms such as chest pain or shortness of breath
> 60 years of age
Obvious neurological symptoms, such as any interval of
unconsciousness, loss of time, inability to perform simple
motor tasks, or loss of memory
Smoke inhalation victims
Pregnancy
104
= EMR
Heat Exposure
= EMT
= AEMT
= Paramedic
Italics = MCP
Move patient to a cool environment.
Strip the patient of clothing, cool the patient, and apply water to the skin.
Apply cold packs to underarms and groin area.
If neither vomiting nor extremely nauseous provide oral fluids.
Hyperthermia patients should be transported to a trauma center.
If hypotensive or mental status changes are present administer NS, 500
ml bolus. May repeat x1
NS 20 ml/kg IV
Continued…
105
Heat Exposure
Geriatric, pediatric, diabetic and spinal injury patients are
most likely to suffer heat-related illnesses.
The following medications increase risks; cardiac,
diuretics, cold medications and psychiatric.
Be prepared for seizures.
Consider other medical conditions (i.e. overdose,
hypoglycemia, CVA).
Transport to a Trauma Center
106
= EMR
Eye Injuries
If possible, contact lenses should be removed.
Chemical Burns:
= EMT
= AEMT
= Paramedic
Italics = MCP
Irrigate immediately with NS or water for a minimum of 20
minutes
Determine chemical involved. Bring MSDS, if available
Continued…
107
Eye Injuries
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Major Eye Trauma:
Cover injured eye.
Do not use a pressure or absorbent dressing on or near any
eye that may have ruptured, or have any penetrating
trauma
Cover both eyes to limit movement
Transport with head elevated at least 30%
Continued…
108
Eye Injuries
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Prior to irrigation with NS or for significant eye pain:
Tetracaine - 2 drops in affected eye(s).
Do not irrigate or use Tetracaine if penetrating trauma
Morgan Lens or nasal cannula and IV tubing for irrigation
Irrigate for at least 30 mins or until Med Control is contacted
109
Pulmonary Edema
CPAP or Bi-PAP (should be primary therapy)
Consider need for possible early ET Tube
If patient has SBP >100:
Nitroglycerin 0.4 mg SL up to X 3 every 5 minutes.
Maintain SBP >100.
110
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Asthma/Emphysema/COPD
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Assist with Albuterol MDI
Consider Albuterol 2.5 mg and Ipratropium 0.5 mg, nebulized with
O2 @ 8-12 LPM.
May repeat Albuterol 2.5 mg nebulized X 2.
After intubation, avoid Auto-PEEP by ventilating at:
8-10 bpm
10-15 bpm
If patient arrests, strongly consider bilateral needle decompression for
relief of tension pneumothorax.
Continued…
111
Asthma/Emphysema/COPD
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
For asthmatics in severe distress:
If >30 kg:
Adult EpiPen and EpiPen Jr. or
Epinephrine (1:1,000) 0.5 mg IM
May repeat Epinephrine (1:1,000) 0.5 mg/kg IM
If <30 kg:
EpiPen Jr. or Epinephrine (1:1,000) 0.01 mg/kg IM (max 0.5 mg)
May repeat Epinephrine (1:1,000) 0.01 mg/kg IM (max 0.5 mg)
COPD:
CPAP or Bi-PAP
112
Continued…
= EMR
Allergic Reaction/Anaphylaxis
If severe allergic reaction, assist patient in with Epi-Pen
if patient has his/her medication.
If patient doesn’t have their Epi-pen, access drug bag after MCP
If >30 kg: Adult EpiPen and EpiPen Jr.
= EMT
= AEMT
= Paramedic
Italics = MCP
or Epinephrine (1:1,000) 0.5 mg IM
May repeat Epinephrine (1:1,000) 0.5 mg IM
If <30 kg: EpiPen Jr.
or Epinephrine (1:1,000) 0.01 mg/kg IM (max 0.5 mg)
May repeat Epinephrine (1:1,000) 0.01 mg/kg IM (max 0.5 mg)
If patient develops wheezing, assist them with taking their prescribed
Albuterol metered dose inhaler
The EMT may NOT administer Albuterol to a patient that is not currently
prescribed Albuterol
Continued…
113
= EMR
Allergic Reaction/Anaphylaxis
= EMT
= AEMT
= Paramedic
Italics = MCP
If patient deteriorating or unresponsive, consider early intubation, possibly
with smaller than normal ET tube.
If patient is apneic, intubate
In conscious patient requiring ETT, consider:
Lidocaine Jelly to the ET tube
Lidocaine, 100 mg IN (1/2 dose per nostril) or via Nebulizer
Lidocaine 1.5 mg/kg IN or Nebulizer (max. dose 100 mg)
If patient is wheezing: Albuterol, 2.5 mg and Ipratropium, 0.5 mg in
nebulizer with O2 flowing at 8-12 LPM, may repeat Albuterol x2
Continued…
114
= EMR
Allergic Reaction/Anaphylaxis
= EMT
= AEMT
= Paramedic
Italics = MCP
If patient is intubated, Albuterol, 2.5 mg by nebulizer into the
endotracheal tube. If Ipratropium not given before intubation, add to
first Albuterol.
If hypotensive, NS, bolus to maintain SBP >100
If hypotensive, NS IV 20 ml/kg to maintain adequate perfusion
Diphenhydramine 50 mg, IM/IV
Diphenhydramine 1 mg/kg IM/IV (max dose 50 mg)
If patient remains hypotensive after a fluid bolus, Epinephrine
(1:10,000) 0.5 mg, slow IV.
For patients unresponsive to Epinephrine, Glucagon 1 mg, IV/IM.
115
Altered LOC
If glucose <60, or suspicion of hypoglycemia
Oral Glucose
D10, 250 ml IV at a wide open rate
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
D10, 5 ml/kg IVP maximum single dose of 250 ml
Repeat D10 250 ml. if blood sugar remains under 60
Document amount of D10 in milliliters
If no vascular access, Glucagon, 1 mg IM.
Maintain normothermia
Continued…
116
= EMR
Altered LOC
= EMT
= AEMT
= Paramedic
Italics = MCP
Naloxone, 2 mg IN or slow IVP or or up to 4 mg IM (Titrate to effect)
<20 kg - 0.1 mg/kg slow IN/IV/IM/IO/ETT (Max. 2 mg) 1 mg IN (may
repeat once)
>20 kg - 2 mg slow IN/IV/IM/IO/ETT (may repeat once)
Slow IV is the preferred method, but may be given IN first
If IN, if resp. don’t improve after 3 min., administer IV dose
Titrate to effect or adequate respirations
After Naloxone administration, transport is encouraged
Continued…
117
Altered LOC
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
CLINICAL PEARLS
Patients 18 y/o may be permitted to refuse if:
Repeat physical exam and V/S, patient must be A&O X 3
Warn the patient that there is a significant risk of going back into
hypoglycemia, especially if on oral hypoglycemics
Advise the patient to eat something substantial immediately
Advise the patient to contact their family physician as soon as
possible to minimize future episodes
Advise the patient to stay with someone
Follow normal patient refusal procedures
Continue D10 infusion (minimum of 250 ml) during the refusal
process
Ensure that the EMS Coordinator of the hospital that replaces
your Drug Bag and Supplies receives a copy of the run sheet
for his/her records.
118
Seizures
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
BVM and nasopharyngeal airway during seizure as needed.
Maintain normothermia.
If glucose <60, or there is strong suspicion of hypoglycemia despite
glucometer readings:
119
Administer Oral Glucose (if able to swallow)
D10, 250 ml IV wide open
D10, 5 ml/kg IVP maximum single dose of 250 ml
D10 may be repeated in 10 minutes with BGL <60
If no vascular access, Glucagon, 1 mg IM
In a diabetic patient with an insulin pump and a glucose <60, disconnect
patient from the pump or “suspend” the device if you are familiar with its
operation.
Continued…
= EMR
Seizures
= EMT
= AEMT
= Paramedic
Italics = MCP
If seizing, Diazepam, 5 mg slow IV/IO or
Midazolam, 10 mg, IN (5 mg in each nostril)
Midazolam may also be given 2 mg slow IV/IO or
Midazolam may also be given 4 mg IM
IM Midazolam is a no longer last resort
Repeat Diazepam, 5 mg slow IV/IO or Midazolam, 5 mg, IN, or
Midazolam 2 mg IV/IO , or Midazolam 4 mg IM
If no vascular access or MAD, Diazepam, 10 mg PR
Continued…
120
= EMR
Seizures
= EMT
= AEMT
= Paramedic
Italics = MCP
If seizing, Diazepam, 0.2 mg/kg slow IV (Max dose 5 mg) or
Midazolam, 0.2 mg/kg, IN (Max dose 4 mg)
Midazolam, 0.1 mg/kg slow IVP (Max dose 2 mg)
Midazolam, 0.2 mg/kg IM (Max dose 4 mg)
Repeat Diazepam, 0.2 mg/kg slow IV or
Repeat with half dose of administered Midazolam
Do NOT repeat if Midazolam was administered IM
If no vascular access or MAD, Diazepam, 0.5 mg/kg PR.
(Max. dose 10 mg)
Continued…
121
Seizures
When obtaining history be sure to include the
following:
Description of seizures, areas of body involved, and
duration
Other known medical history; i.e. head injury, diabetes,
drugs, alcohol, stroke, heart disease.
122
= EMR
Extrapyramidal (Dystonic) Reactions
Patient will be on a drug therapy of a
Phenothiazine (Phenergan, Thorazine, etc.)
Butyrophenone (Haldol, Droperidol, etc.)
Signs/Symptoms
Acute muscular spasms
Motor restlessness
Mental status unaffected
Vitals normal
Initiate IV of Normal Saline
123
= EMT
= AEMT
= Paramedic
Italics = MCP
Continued…
= EMR
Extrapyramidal (Dystonic) Reactions
If glucose is <60, or suspicion of hypoglycemia
D10, 250 ml IV wide open
D10, 5 ml/kg IVP maximum single dose of 250 ml
D10 may be repeated in 10 minutes with BGL <60
If no vascular access, Glucagon, 1 mg IM
Consider Diphenhydramine 50 mg IV or IM
Diphenhydramine 1 mg/kg IV or IM (Max dose 50 mg)
124
= EMT
= AEMT
= Paramedic
Italics = MCP
= EMR
Overdose
= EMT
= AEMT
= Paramedic
Italics = MCP
Contact MCP for suspected poisonings, Poison Control is for Public
Manage Airway
Gather appropriate history
Thorough search for source substance
Glucometer
Ingested Poison
Transport container and / or remaining medication to the hospital
with the patient.
Continued…
125
Narcotic Overdose
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Consider patient restraint before Naloxone
If patient has a pulse, Naloxone before ETT
Naloxone, 2 mg IN or slow IVP or or up to 4 mg IM (Titrate to effect)
<20 kg - 0.1 mg/kg slow IN/IV/IM/IO/ETT (Max. 2 mg), 1 mg IN (may repeat once)
>20 kg - 2 mg slow IN/IV/IM/IO/ETT (may repeat once)
Slow IV is the preferred method, but may be given IN first
If IN, if resp. don’t improve after 3 min., administer IV dose
All levels except EMR may repeat Narcan dosing
126
Crack/Cocaine Overdose
Nitroglycerine 0.4 mg SL, if SBP >100
Diazepam, 5 mg slow IV/IO, if SBP >100 or
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Midazolam, 10 mg, IN (5 mg in each nostril)
Midazolam may also be given 2 mg slow IV or
Midazolam may also be given 4 mg IM
IM Midazolam is a last resort
Repeat Diazepam, 5 mg slow IV/IO or Midazolam, 5 mg,
IN, or Midazolam 2 mg IV/IO , or Midazolam 4 mg IM
Continued…
127
= EMR
Tricyclic Overdose
= EMT
= AEMT
= Paramedic
Italics = MCP
Sodium Bicarbonate, 1 mEq/kg, IV.
Repeat Sodium Bicarbonate 0.5 mEq/kg, IV for
persistent QRS prolongation.
Note: Overdose with tricyclic antidepressant
medications may be evidenced by bradycardia,
tachycardia, hypotension and prolongation of the
QRS complex. Risk of rapid deterioration or sudden
onset V. Fib is high.
Continued…
128
= EMR
Blocker Overdose
= EMT
= AEMT
= Paramedic
Italics = MCP
Calcium Channel Blocker Overdose
Calcium Chloride, 1 gm IV
Calcium Chloride, 0.2 ml/kg (20mg/kg) slow IVP
Max. dose 500 mg
Glucagon, 1 mg IM or IV
Beta Blocker Overdose
Glucagon 1 mg, IM or IV.
Continued…
129
Abdominal Pain
Ondansetron (Zofran), 4 mg IV for nausea or vomiting
If no IV, 4 mg dissolving tablet PO may be administered
Or administer the IV dose PO
AEMT will administer 4 mg Zofran PO
Ondansetron (Zofran), 0.1 mg IV (Max dose 4 mg)
AEMT will administer 4 mg PO if patient is > 12 y/o and > 40 kg
For pain relief, consider Pain Control Protocol
AEMT requires MCP for pediatric pain relief
130
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
= EMR
Newborn Care & Resuscitation
= EMT
= AEMT
= Paramedic
Italics = MCP
General Considerations
Directly after delivery, dry, warm, maintain airway.
Place in the sniffing position (1” towel under shoulders).
Suction infant until all secretions are clear of airway.
If meconium-stained and vigorous, with strong respirations, good muscle
tone, and heart rate greater than 100 BPM, suction the mouth and nose in
the same way as for infants with clear fluid.
If meconium-stained and depressed, with poor respiratory effort, decreased
muscle tone, or heart rate less than 100 BPM,
Suction the trachea before taking other resuscitative steps.
Lower airway suction is achieved by intubating the infant and suctioning
directly through the ET Tube, re-intubated with a new tube each time
Continued…
131
= EMR
Newborn Care & Resuscitation
= EMT
= AEMT
= Paramedic
Italics = MCP
General Considerations
Mechanical suction may be used on infants, but only if the suction
pressure does not exceed 100 mmHg or 136 cm H2O. Bulb
suctioning is preferred.
If drying and suctioning has not provided enough tactile stimulation,
try flicking the infant’s feet and/or rubbing the infant’s back. If this
stimulation does not improve the infant’s breathing, then BVM may
be necessary.
Avoid direct application of cool oxygen to infant’s facial area as may
cause respiratory depression
Use length/weight based resuscitation tape
Continued…
132
= EMR
Newborn Care & Resuscitation
Assess the airway/breathing while drying and position
head down.
If HR <100, ventilation is necessary to increase HR
= EMT
= AEMT
= Paramedic
Italics = MCP
Ventilate at 40-60/min
Ventilation is also indicated for apnea and persistent central
cyanosis.
Despite adequate ventilation, if HR <60 begin CPR
Compress at 120/bpm. (ratio of 3:1)
Epinephrine 1:10,000, 0.01 mg/kg IV/IO
or 1:1,000 0.1 mg/kg ETT.
If no response, repeat Epinephrine 1:10,000 every 3-5 min.
Continued…
133
= EMR
Newborn Care & Resuscitation
= EMT
= AEMT
= Paramedic
Italics = MCP
If hypovolemic, NS, 10 ml/kg over 5-10 minutes.
Consider Naloxone, 0.1 mg/kg, IV/IO/IM every 3 minutes
until respirations improve.
Dextrose 2 ml/kg D10 if BS <40 mg/dl.
134
= EMR
Psychiatric Emergencies
= EMT
= AEMT
= Paramedic
Italics = MCP
Consider staging until police have assured
scene safety
Have patient searched for weapons
Obtain previous mental health history:
Suicidal or violent history
Previous psychiatric hospitalization, when and where
Location that patient receives mental health care
Medications
Recreational drugs/alcohol – amount, names
Continued…
135
Psychiatric Emergencies
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Do not judge, just treat.
Transport all patients who are not making rational
decisions and who are a threat to themselves or others for
medical evaluation
Threat of suicide, overdose of medication, drugs or alcohol
and/or threats to the health and well being of others are not
considered rational.
136
= EMR
Combative Patients
= EMT
= AEMT
= Paramedic
Italics = MCP
Determine patient incompetence
Consider medical causes for patient’s condition
Explain the need for restraint to the patient
Recheck a restrained patient’s ability to breathe often
Have the ability to remove/cut restraints if the patient
vomits or develops respiratory distress
Continued…
137
= EMR
Combative Patients
= EMT
= AEMT
= Paramedic
Italics = MCP
Document the restraints used and justification for the restraints thoroughly
Do not transport restrained patients in a prone position with the hands
and feet behind the back or sandwiched between backboards or other
items.
Consider Ketamine 500 mg IM (repeat in 10 min.)
2 separate doses of 250 mg in large muscles (anterolateral thigh)
Or 100 mg slow IVP (repeat in 5 min.)
Consider Midazolam, 10 mg IN (5 mg in each nostril) (repeat in 5 min.)
or Midazolam 2 mg IV (repeat in 5 min.)
or Midazolam 4 mg IM (repeat in 10 min.)
All sedatives may be repeated for combative patients
Continued…
138
Combative Patients
= EMR
= EMT
= AEMT
= Paramedic
Italics = MCP
Pediatric Sedation
Consider Ketamine 1 mg/kg slow IV (Max dose 100 mg)
Ketamine 5 mg/kg IM (Max dose 500 mg)
Patient must be 8 y/o or greater
Consider Midazolam, 0.2 mg/kg IN/IM (Max dose 4 mg)
or Midazolam 0.1 mg/kg slow IV (Max dose 2 mg)
Call MCP for all repeat sedative doses
139
Summary
Methodology of Instruction
Stipulations
2015 Changes
The 2015 Protocol
Questions & Answers
140