Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
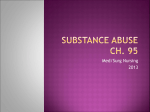
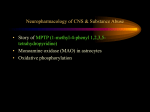
Click on the arrow to proceed to the next slide. Click on the to proceed to the next slide Click on the to go back to the previous slide Click on the to go to the “sections” slide You will be given opportunities throughout to test your knowledge Identify keys components to the pathophysiology of alcohol withdrawal and neurological involvement Identify the body’s responses to stress and how the HPA axis relates to aging Identify the signs, symptoms, and behaviors of alcohol withdrawal Apply learned concepts to a case study involving the care of the patient in alcohol withdrawal Identify how genetics and metabolism are related in alcohol abuse Identify inflammation and it’s role in comorbidities associated with alcohol abuse Sections Click on individual sections to jump to that section Case Study (1) Neurological Pathophysiology(2) Hypothalamic-pituitary-adrenal Axis(HPA Axis), “fight or flight”, & Generalized Stress Response(3) Signs & Symptoms of alcohol withdrawal(4) Symptom Management(5) Nursing Interventions(6) Genetics & Metabolism (7) Alcoholic Liver Disease & Inflammation (8) 31 year old male, admitted to your unit for alcohol detox, states he had his last drink over 24 hours ago, and exhibits the following signs and symptoms Complains of nausea but no vomiting Tremulousness States he has a tight “rubber band” feeling around his head Profuse sweating Click here to return to data Feels intense anxiety Denies hallucinations Denies agitation Knows the current place and time Click here to return to data We will come back to this case study later in the tutorial Neurons- nerve cells that communicate to each other using electrical and chemical signals (neurotransmitters) Synapse- giving and receiving ends where neurotransmitters are transported from one neuron to the next Presynaptic neurons release neurotransmitters to receptors on the postsynaptic neuron Lovinger, 2008 gamma-Aminobutyric acid (GABA) GABA Glutamate Glutamate Microsoft, 2007 Main inhibitory neurotransmitter in the human body Found in all areas of the brain Regulates neuronal excitability throughout the body Binds to GABA receptors in the presynaptic and postsynaptic phases of transmission Lovinger, 2008 Alcohol enhances GABA by increasing the inhibitory effects (sedative effect) Current drugs in the benzodiazepine and barbiturate families can replace alcohol in the brain for successful and non life threatening alcohol withdrawal treatment Benzodiazepines bind here NIAAA, 2009 Exhibits excitatory effects on the brain Like GABA, is found all over the brain Binds to NMDA receptors in the brain Acute alcohol exposure inhibits glutamate transmission, causing neuronal excitability (leading to seizures) Chronic alcohol exposure increases the number of NMDA receptors Lovinger, 2008 Increased numbers of NMDA receptors leads to withdrawal hyper excitability and alcohol induced neuronal damage when GABA cannot produce inhibitory effects Involved in cognitive functions such as learning and memory Drugs that act to reduce receptors involved with glutamate such as memantine and topiramate are either being studied or used for treatment GABA is an inhibitory neurotransmitter GABA and alcohol bind to the same receptors In alcohol withdrawal treatment, benzodiazepines bind to those same receptors, preventing neurological withdrawal symptoms Glutamate in an excitatory neurotransmitter Alcohol binds to certain receptors to produce sedating effects and long term use causes increased NMDA receptors In the absence of alcohol, NMDA and glutamate create excitability since GABA is not present to inhibit this (seizures) Neuroendocrine response to stress (Brain)(Hormones) Contributes to psychological and physiological responses to alcohol Ultimately stimulates glucocorticoid secretion Three way relationship exists between alcohol use, glucocorticoid secretion, and aging Hutchison & Spencer, 1999 Adrenal Gland Stressful situation (alcohol intoxication) Hypothalamus Pituitary Gland Hint: Roll mouse over body parts to reveal what they release. Adrenal Glands So now what? Cortisol released from the adrenal glands of the kidneys prevent further release of CRH and ACTH. Is this a negative or positive feedback loop? Think about it and save it for the end of the section. Hutchison & Spencer, 1999 & Microsoft 2007 Alcohol use stimulates the HPA Axis Length of stimulation depends on amounts of alcohol consumed or blood alcohol level (BAC) Hutchison & Spencer, 1999 & Microsoft 2007 Blood alcohol levels (BAC) and HPA Axis activation have a strong genetic component Strong evidence exists of a defective gene, not allowing the correct metabolism of alcohol People with this gene have significant high cortisol levels Hutchison & Spencer, 1999 Aging people are more at risk for HPA Axis overstimulation Why? Hutchison & Spencer, 1999 Recovery is slower The feedback loop takes longer to get the message back Getting rid of catecholamines takes longer Cortisol levels eventually will cause neuronal death Norepinephrine/ Noradrenaline Released Alpha 1 Diaphoretic Alpha 2 Dilated Pupils Increased Blood Pressure GI Tract off Lowers Insulin Beta 1 Increased HR Beta 2 Increased Respirations A patient in acute alcohol withdrawal is experiencing sweats (diaphoresis) and an increase in heart rate (tachycardia). What is causing this? Click on the correct answer Sympathetic Nervous System HPA Axis Delirium Accurate nursing assessment of patients with alcohol dependence can help to eliminate or minimize negative patient outcomes Recognizing/identifying signs/symptoms/behaviors of those at risk for alcohol withdrawal syndrome McKinley, 2005 Tremors Sweating Nausea Vomiting Autonomic Hyperactivity Agitation Anxiety Auditory disturbances Clouding of sensorium Visual/Tactile disturbances Neuropsychiatric Alterations McKinley, 2005 Signs/symptoms can appear within 24 hours of last drink Peak of s/s happen as early as 24 hours and stop around 48 hours Delirium tremens typically occur between 48-72 hours after last drink Delirium tremens is considered an emergency and can end in death McKinley, 2005 Excessive activation of NMDA increases the chance of seizures Long term exposure to alcohol depresses GABA, making brain more vulnerable to seizures For nurses, the implication would be to assess patient history of withdrawal/detox and treat more aggressively those who are most at risk Becker, 1998 48% of inpatient alcoholics who suffered seizures had gone through several detoxifications in their pasts In the same study, 12% of alcoholics who had seizures during detoxification had little to no history of detoxification Clinical Institute Withdrawal Assessment (CIWA) Selective Severity Assessment (SSA) CAGE questions Alcohol Withdrawal Syndrome Type Indicator Alcohol Use Disorders Identification Test CIWA is a 10 item rating scale that discriminates symptoms of gastric distress, perceptual distortions, cognitive impairment, anxiety, agitation, and headache Ragasis,2004 Nausea/Vomiting 0 No Nausea/Vomiting 1-3 Mild nausea 4-6 Intermittent Nausea with Dry Heaves 7-Constant Nausea, Dry Heaves, Vomiting Paroxysmal Sweats 0-No sweat visible 1-3 Barely Sweating 4-6 Beads of Sweat Obvious on Forehead 7- Drenching Sweats Click here to return to data Anxiety Tremors 0-No tremors 1-3 Not visible, but can be felt fingertip to fingertip 4- Moderate with arms extended 7-severe, even without arms extended “Do you feel nervous?” 0-No anxiety/at ease 1-3 Mildly anxious 4-6 Moderately anxious 7-Acute panic, anxiety Click here to return to data Agitation None 1-Very mild 2-Mild 3-Moderate 4-Moderately sever 5-Severe 6-Very severe 7-Extremely severe Headache/Fullness 0-Normal activity 1-3 Somewhat more than usual 4-6 Moderately fidgety/restless 7-Paces back and forth, thrashing about Click here to return to data Does the light appear to be too bright? Is the color different? Does it hurt your eyes? Are you seeing anything that is disturbing to you? Are you seeing things you know aren’t there? 0-None 4-Mild sensitivity to light to occasionally seeing things you can’t 7-Constant visual hallucinations Are you aware of sounds around you? Are they harsh? Do they frighten you? Are you hearing anything disturbing? Are you hearing things you know aren’t there? 0-None 2-Very mild harshness of ability to frighten 3-Moderate 4-Moderately severe hallucinations 5-Severe hallucinations 6-Extremely severe hallucinations 7-Continuous hallucinations Do you feel any itching, or pins and needles? Any numbness or burning? Do you feel bugs crawling on or under your skin? 0-None 1-Very mild itching 2-Mild itching 3- Moderate itching 4-Moderate hallucinations 5-Severe hallucinations 6-Extremely severe hallucinations 7-Continuous hallucinations “ What day is it? Where are you? Who am I?” 0-oriented 1-Cannot do serial additions or uncertain of dates 2-Disoriented to date but not by more than 2 days 3-Disoriented for date by more than 2 days 4-Disoriented to time/place Case Study Prepare to use your critical thinking skills and assess your patient in alcohol withdrawal! What is going on? Objective Data Subjective Data Patient is sweating profusely Exhibits moderate tremors when asked to extend arms Appears to be restless and jittery during assessment Click here to review the case study! Patient complains of intense headache, a “rubber band” is tight around his head Patient complains of intense anxiety Patient denies audio/visual/tactile hallucinations Patient is alert and oriented to self, place and time Patient complains of moderate nausea, no vomiting Click here to return to case study Subjective Data Objective Data Profuse sweating 4-7 Moderate tremors 4 Moderate agitation 4-6 Moderate headache 4-6 Intense anxiety 4-6 No hallucinations 0 Oriented 0 Mild nausea 1-3 Click on individual signs/symptoms to take you to the scores Score range is 21-32 Now what? Benzodiazepines are given, to meet receptors in the brain alcohol is no longer binding to, to prevent hyperexcitibility and seizures Intravenous fluids Anti inflammatory medications for the headache Thiamine (patients often malnourished) Multivitamin (patients often malnourished) Folic Acid (patients often malnourished) Therapeutic relations with patient (support) Always remember to continue to use the nursing process for outcomes and continued care! The processing of alcohol involves…. Gastrointestinal tract absorption 2. Alcohol distribution in the body 3. Liver metabolism Genetics and Environmental factors influence these processes 1. NIAAA, 2007 GI Surgeries Concentration of alcohol in beverage Rate of consumption Presence of food in the stomach Liver Enzymes (Needed for alcohol breakdown) Cytosolic alcohol dehydrogenase (ADH) Mitochondrial aldehyde dehydrogenase NIAAA, 2007 (ALDH2) The amount of alcohol metabolized in the body relies on: Liver Size & Body Mass Genetics have influences on ADH & ALDH and affect how people metabolize alcohol This can help to explain why certain groups of people have variances in levels of alcohol abuse NIAAA, 2007 Alcoholic Liver Disease (ALD) Alcoholic Cardiomyopathy Alcohol Related Dementia Peripheral Neuropathy Gastritis Pancreatitis Alcoholic Liver Disease (ALD) Fatty Liver Alcoholic Hepatitis Cirrhosis Long term alcohol abuse is leading cause of liver disease in the U.S. Alcohol, Research, & Health, 2000 What do you think? Click on a box to find out? No Yes Repeated Alcohol Abuse Endotoxins Produced Activate Immune System Roll mouse over underlined words for more information. Neuman, 2001 Cytokines Released Promote Scar Formation Stimulate More Cytokines Chronic inflammation from chronic alcohol exposure can cause hepatocyte apoptosis Increased numbers of cytokines continue to be activated Increased scarring occurs Cell injury increases Increase in cell death Compromised organ function Organ failure Alcoholic Liver Disease (ALD) Fatty Liver Alcoholic Hepatitis Depending on what is happening to the liver, interventions lie in decreasing the inflammation, resting the organ, preventing hepatic encephalopathy, preventing ascites, and abstaining from the stressor (alcohol) Cirrhosis One role of the nurse is to provide safe patient care that contributes to ideal patient outcomes. In caring for the patient in alcohol withdrawal these include: Keeping safety in mind (seizure pads) Eliminate extraneous stimuli (keep it quiet) Prevent falls (bed/chair alarms, rounding) Watching for s/s of bleeding (since the liver might be compromised) Critical thinking for s/s of other disease processes that might mimic AWS, as to avoid mistreating (medicating for AWS when patient might have a low blood sugar) Monitor all values related to liver function (coagulation, enzymes, etc.) Promote healing through nursing/medical interventions Be familiar with the pathophysiology of what is going on with the patient Look at the “whole” picture Advocate for the patient Animated images not otherwise specified, Microsoft Clip Art, (2009), obtained at http://office.microsoft.com/en-us/clipart/default.aspx Axen, D., Koranda, A., & McKay, A., (2004). Using a Symptom-Triggered Approach to Manage Patients in Acute Alcohol Withdrawal. Medsurg Nursing, February 2004, (13)1. Author unknown., Medical Consequences of Alcohol Abuse. (2000). Alcohol Research & Health., Vol. 24, No. 1. Becker, H.C., Kindling in Alcohol Withdrawal. (1998). Alcohol Health & Research World. Vol. 22, No. 1. Hutchison, K.E. & Spencer, R.L., Alcohol, Aging, and the Stress Response. (1999). Alcohol Research & Health. Vol. 23, No. 4. Lovinger, D.M., Communication Networks in the Brain: Neurons, Receptors, Neurotransmitters, and Alcohol.(2008). Alcohol Research & Health. Vol. 31 No. 3. Retrieved on the world wide web on March 31st, 2009 at http://pubs.niaaa.nih.gov/publications/arh313/196214.htm. McKinley, M.G., (2005). Alcohol Withdrawal Syndrome: Overlooked and Mismanaged? Critical Care Nurse. Vol. 25, No. 3. National Institute on Alcohol Abuse and Alcoholism., (2007). Alcohol Metabolism: An Update. Retrieved on the world wide web on April 16th, 2009 at http://pub.niaaa.nih.gov/publications/AA72/AA72.htm National Institute on Alcohol Abuse and Alcoholism, 2009, Permission obtained for use of pictures/graphics. Neuman, M. G., (2001). Cytokines-Central Factors in Alcohol Liver Disease. Retrieved on the world wide web on May 2nd, 2010 at http://pubs.niaaa.nih.gov/publications.arh274/307-316.htm. Ragaisis K.M., (2004). Alcohol Screening in the Acute Care Hospital. Journal of Addictions Nursing, 15: 171-175. Saitz, R., (1998). Introduction to Alcohol Withdrawal. Alcohol Health & Research World. Vol. 22, No. 1. As you have seen in previous slides, the sympathetic nervous (SNS) system, part of the GSR, is responsible for many signs and symptoms of alcohol withdrawal Click here to return to the tutorial Without inflammation , injuries would not be localized and the immune system would not be able to do its job, preventing healing and further infections. Click here to return to inflammation slide When the body has an “injury”, inflammation occurs, attempts to localize the injury, and calls the immune system to work as a team to heal the injury and prevent further spread or damage. Click here to return to inflammation slide