Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
DBS Team and Documentation
Punit Agrawal, DO
Movement Disorder Division
Department of Neurology
The Ohio State University
Team for Neuromodulation
Neurology/Pain/Anesthesia
Neurosurgery
Psychiatry/Psychology
Radiology
Physical Medicine and Rehabilitation
Beyond the physicians:
Physician assistants, Nurse practitioners, Allied Health
Ancillary staff including medical secretary/assistant,
office manager, and clinical coordinator
Research
Ethics
Roles of the Team
Referrals and scheduling
Evaluation for therapy
Team review of evaluations
Pre-surgical evaluation
Surgery
Post surgical care
Therapy Management
Research
Documentation
Proper documentation and record keeping is
important for several reasons including:
Allows for increased insurance approval for therapy
Records of neuromodulatory therapy results
Enhances communication with referring care provider
and other team members
Assists in proper reimbursement of services
When concerns of complications of devices or failure
of therapy, previous records are very helpful to
identifying potential problems.
Medical Records
These should include
Pre-therapy screening tests including imaging,
previous failed therapies, and evaluation
reports from various team members
Goals of therapy
Surgical Reports and subsequent studies
Psychosocial evaluations and concerns
Post-operative notes and evaluations
Records of therapy intervention with results
Initial Evaluations - Key Items to Include
Severe debilitating disease with indication for
therapy
Chronological history of disease
Previous failed therapies
Goals and expectations of therapy and
discussion of potential risks/complications
Things to Document with Each
Programming Visit
Disease Indication for Therapy
Therapy Target and Goals
Electrode/Device Models
Date of implant and battery changes
Device status (battery life, impedences, etc…)
Initial and Final Settings
Side effects or Complications
Patient/Family Education Provided
Date of Programming: ___________
Date of Therapy Initiation:___________
Date Electrode Placement: ___________
Date of IPG Placement:
______
PATIENT INFO
Site of implant:
IPG:
PW:
STN VIM
Right Left
Soletra
Kinetra
Freq:
Contact:
Amp (V)
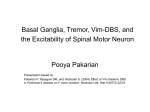
Sample of DBS
Therapy Monopolar
Review Worksheet
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
0
GPi
Other___________
Activa PC
1
Activa RC
2
Observations or Comments
3
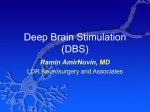
Sample Therapy Summary Sheet for DBS
Patient Name and Identifiers:
Date of implant:
Date of initial program:
Therapy Device:
Indication for therapy:
Site of implant: STN VIM
Right Left
GPi
Other___________
Initial programming summary:
Right
PW:
Freq:
Max Volt.
Left
PW:
Comment/Observation
Lead 0
1
2
3
Programming session summary:
Date
Anode Cathode
R
L
R
L
R
L
R
L
R
L
Max Volt.
Freq:
Comment/Observation
0
1
2
3
PW Freq
Amp Comments:
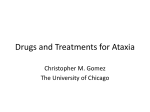
Sample Letter for Prior Authorization
Date
Patient Name:
Patient Date of Birth:
Insurance Identification No.:
Physician Name:
Tax Identification No.:
Projected Surgery Date:
Dear {payer name}:
The above named patient has been diagnosed with {diagnosis description}, diagnosis code { ICD-9
code) and is being recommended by the physician as a candidate for Deep Brain Stimulation Therapy. I
am requesting prior authorization on behalf of the patient for an Activa Deep Brain Stimulation System
permanent implant (Associated CPT Codes: 21499, 64999, 70450, 70551, 76376 or 76377, 61863, 61867 or
61867, 61885 or 61886, 95961 or 95962, 95970 or 95978). The procedure will be done at { facility name} in {
city, state}. I have attached supporting documentation for your review.
I request written confirmation that this therapy is a covered benefit based on medical necessity and that
associated professional fees for the surgery will be covered. The charge for the device is included with
the hospital fees.
Thank you for your prompt review of this information and for your coverage consideration. If you
have any questions, please contact me.
Sincerely,
Sample Letter for Medical Necessity
Sample Letter of Medical Necessity
DBS Tremor Control Therapy
Date:
Inside Address
Patient:
Policy Holder:
ID/Social Security #:
Dear __________:
This letter is to request a predetermination of coverage and/or prior authorization for the
implantation of a Medtronic Activa® Tremor Control System for the suppression of tremor
in patients with Essential Tremor or Parkinsonian tremor. The therapy involves the
unilateral implantation of an insulated wire lead in the ventral intermediate (VIM) nucleus
of the thalamus. The lead is connected to a pacemaker-like neurostimulator that provides
stimulation of the targeted area in the brain. The totally implantable Activa Tremor
Control System includes a quadripolar DBS™ lead for deep brain stimulation, an
extension, and the Soletra® implantable neurostimulator. The patient may also receive the
Access Review™ Patient Therapy Controller.
Activa Tremor Control Therapy has been available for commercial use in Europe, Canada
and Australia since February 1995. It was approved by the FDA for commercial release in
the United States in July 1997. Medicare has national coverage on Deep Brain Stimulation
for Essential Tremor and Parkinson Disease. Effective April 1st, 2003, Medicare will cover
unilateral or bilateral thalamic VIM DBS for the treatment of essential tremor (ET) and/or
Parkinsonian tremor and unilateral or bilateral STN or GPi DBS for the treatment of
Parkinson’s disease. Medicare’s coverage conditions may be found at:
www.cms.hhs.gov/manuals/pm_trans/AB03023.pdf. Enclosed you will find further
information about this therapy and summaries of clinical studies.
Based on my review, I believe that my patient, ________________, is an excellent candidate
for this therapy.
Document Chronological History
(Document the patient’s history of interventional efforts noting therapies/procedures and
medications that have previously been attempted. Note the outcome of each. A timeline may
be useful.)
Recommend Medtronic Activa Tremor Control Therapy
(State how this therapy is an appropriate intervention at this point in the patient’s care. Note
therapeutic goals, anticipated outcome, risks of performing the procedure, risks of not
performing the procedure, and possible complications.)
Describe the Implant Procedure
(Describe the surgery itself, listing procedure codes (CPT) anticipated. Note the follow-up care
associated with the therapy. This could be an attachment rather than in the body of the letter
itself.)
Because ___________ fits the patient selection criteria and has not responded to other
measures, I recommend test stimulation for Activa Therapy. The decision to implant the
Activa System will be based on the patient’s intra-operative response to the test stimulation
as indicated by tremor suppression and improvement in neurological testing.
I request confirmation that this therapy is a covered benefit based on medical necessity, and
that associated professional fees for the surgery and follow-up will be covered. I request
authorization for all costs associated with this procedure including physician professional
fees and hospital fees. The charge for the device is included with the hospital fees. The
implant procedure has been scheduled at [name of facility] on [date].
Thank you for your review of this information and for your coverage consideration. If you
have any questions, please contact me.
Sincerely,
_______________, M.D.
[Personalize the letter for the particular patient using the information outline which
follows. You may require one or more paragraphs for each of the headings listed.]
Address each of the following points:
Document Current Findings/Status
(Describe the patient’s current status including diagnosis, complaints, and level of impairment.
Detail functional impairments and state how quality of life, activities of daily living, caretaker
(if applicable), employment, etc. are affected.)
(This document is a template only. Medtronic staff members would never complete such a form for their customers)
Additional Key Elements to
Successful Prior Authorization for
Therapy and Reimbursement
Identify a staff member within the practice
to coordinate all prior authorization and
pre-certification processes with payers and
hospitals.
Involve the patient and/or family in the prior
authorization process as appropriate.
Follow the payer’s conditions for coverage.
Prepare a clear and concise letter of medical
necessity.
Educate the payer regarding the therapy, as
needed.