Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
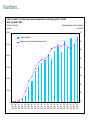
Incident Reporting in Healthcare and the Associated Human Factors Issues Sarah Scobie Head of Analysis and Feedback Melinda Lyons Human Factors Lead Presentation today • The National Reporting and Learning Service • Healthcare’s achievements in incident reporting • The Human Factors issues in incident reporting in healthcare Purpose of the Reporting and Learning System Learning for safety improvement Hazard and risk identification New and emerging hazards Highlighting unsolved problems Supporting reporting organisations with local reporting Locally, each NHS organisation using data for patient safety and risk management Reporting and Learning Cycle •Know what the problems are •Understand which are most important and why they happen •Inform solutions and recommendations to prevent future harm •Assess the difference How does it collect incidents • Voluntary, confidential national system • Commenced Nov 2003 – over 4 million reports so far • Covers all health sectors • Every severe and death incident individually reviewed for national learning • Undergoing continuous improvement Local Risk Manageme nt System Service eForm Open Access eForms WWW NHS Net 99% incidents Encrypted traffic Reporting and Learning System Secure Database Data cleansing Cleansed Database Analysis and feedback Numbers… Chart 1: Number of incidents reported and organisations reporting by quarter, October 2003 - December 2008 Number of incidents reported Average proportion of trusts reporting per month 300,000 80% Incidents submitted Average proportion of trusts reporting per month 70% 250,000 60% 200,000 50% 150,000 40% 30% 100,000 20% 50,000 10% 0 0% Oct - Jan - Apr - Jul - Oct - Jan - Apr - Jul - Oct - Jan - Apr - Jul - Oct - Jan - Apr - Jul - Oct - Jan - Apr - Jul - Oct Dec Mar Jun Sep Dec Mar Jun Sep Dec Mar Jun Sep Dec Mar Jun Sep Dec Mar Jun Sep Dec 2003 2004 2004 2004 2004 2005 2005 2005 2005 2006 2006 2006 2006 2007 2007 2007 2007 2008 2008 2008 2008 April 07 To March 08 April 07 to March 08 April 07 To March 08 … and text “Cardiac arrest. Patient had mouth full of stomach contents… Both portable suctions not working. Aspiration.” •Provides essential information for learning from individual incidents •Provides case studies to illustrate points which front-line clinicians relate to •Brings incidents and learning alive 1500 Systematic review of NRLS death & severe incidents Systematic review of STEIS reports Ad hoc incident / issue reports e.g. coroners, clinicians 50 Incidents & issues considered by the Weekly Response Group 20 Issues followed up with mini-scope e.g. NRLS search, basic literature search 4 Fullscope 1 RLS based products ... Products & activities Ongoing projects for clinical teams National Institute for Clinical Excellence (NICE) Resuscitation Council National Confidential Enquiry into Patient Outcome and Death (NCEPOD) * correct site burr holes in emergency neurosurgery * delayed diagnosis of head injury in patients affected by alcohol * sudden collapse in orthopaedic surgery related to cement and fat embolism * omission of urgent antibiotics in sepsis and neutropaenia * resuscitation in mental health settings, including management of choking and illicit opiate use * diagnostic delay where minor head injuries lead to significant harm in anticoagulated patients * nasogastric feeding safety in patients with anorexia nervosa * incorrect insertion of central lines * collapse in hospital grounds and the responsibilities of hospital and ambulance service staff * transport for patients in urgent need of transfer between hospitals * correct lens insertion in cataract surgery * patients with arterial disease whose circulation is compromised by anti-embolism stockings * access to emergency gastroscopy out-of-hours * readmission after day surgery * non-invasive ventilation outside high dependency environments * portable syringe drivers in terminal care * female catheters causing urethral trauma if inserted in males * Awareness due to lack of non-return valve on giving set (TIVA) * administration errors when medication supplied in compliance aids * safe storage of emergency medications in staff response vehicles * HIV screening and treatment in maternity care * management of oxygen therapy * over-provision of intravenous fluids * wrong side burr holes / craniotomy * Rapid Response Report Royal College of Ophthalmologists Medicines & Healthcare products Regulatory Agency (MHRA) Royal College of Anaesthetists Chest drains • Trigger incident – patient died from perforated liver after drain inserted Feb 08 • RLS database : 12 reported patient deaths + 15 serious harm Jan 05 - March 08 • + 9 serious incidents from MHRA re problems with equipment • Go back to trusts for more information – RCAs • Key learning – junior doctors without supervision, poor positioning (without ultrasound), unfamiliar with equipment Actions • Report May 2008 developed with input of chest physician/British Thoracic Society • Clear actions including use of ultrasound (NICE 2006) • Longer term action includes work by MHRA (concern re length of dilators) and revised clinical guidelines from British Thoracic Society • Evaluation in 2009 but informal feedback suggests widespread support eg purchase of portable ultrasounds Challenges Under-reporting Closing the loop Analytic methods Priority setting Actionable learning What are the biggest challenges? • “Extracting the important data - what are the real issues that impact on safety, how can we analyse in a meaningful manner, other than simple 'number' crunching.” • “Relies on events being reported; easy to miss recovered incidents as staff see it as part of their skill to do so - may consider don't have time to then report, especially if no harm to the patient.” • “Conflicting demands on existing resources, in respect of support staff, reporters etc” Direction • Embedding and engaging • Trial of specialty reporting • Data mining And not to forget those human factors…. • Human Factors in the analysis • • • • Awareness of Human Error Awareness of Equipment design Awareness of Workload Supporting clinical decisions and education about biases And not to forget those human factors…. • Human Factors in the solutions • • • • Equipment and Environment Design Training and Education Protocols and Checklists Supporting a “just culture” And not to forget those human factors…. • Education of the value of human factors (it’s not just teamwork!) • The role in implementation and stakeholder engagement • Recognition of human errors – even in the most well-meaning of patient safety efforts… • Validation of changes / decisions – did they really make it more safe? www.npsa.nhs.uk [email protected] [email protected]