Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
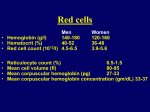
Anaemia gyermekkorban Molnár Dénes Gyermekklinika Cél • Anaemia okainak áttekintése • Anaemia diagnózisának felállításának megközelítése • Vashiányos anaemia diagnosisa és kezelése • Rövid tárgyalása a gyermekkori anaemiák egyéb okainak The Red Blood Cell • Life span: 120 days – 60-90 days in term & 35-50 days in preterm babies • Production – Regulated by epo (other hemopoietic factors. Colony- stimulating factors, interleukins, thrombopoietin are not mentioned here) • Produced by kidneys in response to low O2 – Epo stimulates marrow to make RBC precursors – Needs iron, B12, folate, and amino acid • Destruction – When old or damaged, taken up by spleen The RBC • Membrane • Enzymes • Hemoglobin – Heme (4 heme groups per Hb molecule) • Mediates binding of O2 by Hb – Globin • Protein that surrounds and protects heme molecule • 2 alpha and 2 beta genes (adult Hb) Fontosabb terminológia • Hb – Concentration of RBC Hb in whole blood • Ht (%) – Fractional volume of whole blood occupied by RBC • MCV – Mean value of volume of individual RBC • Microcytic, macrocytic, normocytic • MCHC – Calculated value (Hb/Ht) • Low MCHC indicates hypochromia Fontosabb terminológia • RDW (Red Cell Distribution Width) – Variability of RBC sizes; normal range 11-15 • Ferritin – Storage form of iron • 1 ng of ferritin: 10 mg of iron stores • Transferrin – Transports iron through plasma • Reticulocytes – Young RBC Anaemia okai • Decreased production • Increased destruction • Blood loss Csökkent vvt productio • Defective heme synthesis – Iron deficiency, anemia of chronic disease, lead poisoning • Defective globin synthesis – Alpha and beta thalassemia • Defective DNA synthesis – Nutrient deficiencies (B12, folate) • Impaired epo production – Renal disease Csökkent vvt productio • Marrow failure – Aplastic anemia • congenital Fanconi anemia is an autosomal recessive disorder affecting all bone marrow elements and associated with cardiac, renal, and limb malformations as well as dermal pigmentary changes.(congenital) • acquired – Red cell aplasia • Congenital (Diamond-Blackfan) • Acquired (Transient erythroblastopenia of childhood) • Marrow replacement – Malignancy, myelofibrosis Fokozódó destructio • Extracellular – Antibody mediated – Microangiopathic; HUS, DIC – Drugs, toxins – Hypersplenism Fokozódó destructio • Intracellular – RBC membrane defects • HS (hereditary spherocytosis, stomatocytosis [For as yet unknown reasons, the cells take on an abnormal shape, resembling a mouth or 'stoma‘]), HE (hereditary eliptocytosis) – Enzyme defects • PK (pyruvate kinase), G6PD – Hemglobinopathies • Sickle cell, thalassemia Vérvesztés • Acute hemorrhage • Chronic blood loss Anaemia • Definition – Hb concentration > 2 SD below mean for population • Normal values vary with age Életkori változások Age Newborn 2 wks 3 months 6m – 6 yrs 7-12 yrs Hb (g/l) 168 (137-210) 165 (130-200) 120 (95-145) 120 (105-140) 130 (110-160) Hct (%) 55 (45-65) 50 (42-66) 36 (31-41) 37 (33-42) 38 (34-40) MCV (fl) lowest 110 70-74 76-80 Reticuloc ytes (%) 5 1 1 1 1 Physiologiás anaemia • Drop in Hb around 3 months of age • Pathophysiology – At birth, O2 sat rises sharply • 65% in utero, nearly 100% when comes out – Decrease in epo production – Fetal RBC have shorter survival time (60 days) Anaemia diagnózisa • History • Physical exam • Investigations Anamnézis • Maternal history – Anemia during pregnancy – Pregnancy and delivery • Family history – – – – – Ethnicity Anemia Jaundice, gallstones, cholecystectomy Transfusion history Splenomegaly Anamnézis • Patient’s history – Jaundice at birth – Diet history – Medications – Recent infection – Chronic disease – Bruising, bleeding – Pica Fizikális vizsgálat General appearance – Pallor, jaundice, bruising • Head and neck – Pale mucous membranes and conjunctiva – Angular stomatitis – Adenopathy • Cardiac – Tachycardia, heart failure if severe – Heart murmur • Abdomen – Organomegaly Laborvizsgálatok • Most often incidental finding • CBC and smear – Hb, WBC, plt – MCV • Reticulocyte count • Depending on suspected process – Ferritin and iron studies, folate and B12, LDH, bili, Coombs, osmotic fragility, sickle screen, electrophoresis, bone marrow aspiration, renal function, liver function, etc Morphológiai osztályozás • Cell volume – Microcytic – Macrocytic – Normocytic Microcyter anaemia • Low MCV • Small cells • Etiologies – Iron-deficiency – Thalassemia – Chronic disease – Lead poisoning Macrocytic anemia • High MCV • Big cells • Etiologies – Folic acid and B12 deficiency – Hypothyroidism – Chronic liver disease – Aplastic anemias Normocyter Anaemia • Normal MCV • Production, destruction or loss • Must look at reticulocyte count – Young RBC – Determines adequacy of bone marrow response Normocyter anaemia • High retic count – Blood loss – Hemolysis • Low retic or normal count – – – – – Aplastic anemia Leukemia Chronic disease TEC Congenital hypoplastic syndromes Vashiányos anaemia • Epidemiology – Most common heme abnormality of childhood – Most common nutritional deficiency worldwide – 500 million to 2 billion people are irondeficient according to WHO • 80% of world’s population Vas metabolismus • Body iron content: 2 to 6 g (2 g in adult female, 6 g in adult male) – 1.5-2 g in Hb – 0.5-1 g bound to enzymes, transferrin (protein that carries iron), in storage form (hemosiderin and ferritin) – The rest in myoglobin – At birth, most term infants have 75 mg of elemental iron per kilogram of body weight, found primarily as hemoglobin (75%), but also as storage (15%) and tissue protein iron (10%). • Most iron is recycled • Gut absorption depends on: – Epo production – Body iron stores – Bioavailability of dietary iron Vas források • Bioavailability factors – Fish, poultry, meat • Iron 30% bioavailable – Vegetables • Iron 10% bioavailable • Absorbtion factors – Vitamin C increases absorbtion – Phytates (bran, oats, rye, fiber) and tea decrease absorbtion Vasszükséglet • The estimated iron requirement of the term infant is 1 mg/kg per day. • Because more than 80% of the iron is accreted during the third trimester of gestation, infants born before term must accrete more iron postnatally. Thus, the requirements for preterm infants range from 2 mg/kg per day (bwt. 1500 and 2500 g) to 4 mg/kg per day (bwt. < 1500 g). • Preterm infants who receive erythropoietin appear to need at least 6 mg/kg per day of iron. Vas felszívódás • Generally 10% of dietrary iron is absobed • Greater than 50% of iron from human milk is absorbed compared with typically less than 12% of iron from cow milk-derived formula Rizikócsoportok • Babies – Newborn body contains 75mg/kg – Infants triple blood volume in 1st year – Each kg gain requires increase of 35 to 45 mg body iron – Term babies usually iron replete for 5-6 months, then need iron-fortified foods • Iron recycled in first 2 to 3 months – Pre term at greater risk Rizikócsoportok • Toddlers – Too much cow’s milk!!! • • • • Maximum 16 oz/day Interferes with absorption from other food Colitis Decreased appetite for food • Teenagers – Increased requirement due to growth spurt – Menstrual loss Vashiány okai • Newborn factors – LBW, perinatal hemorrhage, prematurity • Dietary deficiencies – Insufficient intake, poor iron bioavailability • Early cow’s milk exposure – Excessive cow’s milk intake • Blood loss • Iron deficiency itself! – Blunting of intestinal villi leads to increased blood loss Lab eltérések • Bone marrow hemosiderin first disappears – Most reliable indicator of tissue stores • • • • • RDW earliest sign on blood work Ferritin Iron, TIBC Hb Smear – microcytosis and hypochromia • Retic normal or moderately increased – Insufficient response Vashiány hosszútávú következményei • Has been linked to ADHD and breath-holding spells – Although not well substantiated • Exercise intolerance – Study done in teenagers • Neurological impairment – More school difficulties, especially math and memory skills • Increases lead absorption – Leading to more cognitive abnormalities Szűrés • 9 mos of age if high risk – Recommanded by Canadian Task force • High risk – – – – Pre-term / LBW baby High prevalence in community Low SES Special health needs • Consider screening – Toddlers with poor diets – Teenagers Prevenció • Breast fed infant – > 2 servings of iron-fortified cereals at 6 months • Formula-fed infant – Iron-fortified formula • Pre-term breast fed infant – Iron 1 to 2 mg/kg at 1-2 mos, until 6-12 mos • No cow’s milk until 12 months • Limit cow’s milk intake in toddlers – < 500 cc from 1 to 5 yrs Kezelés • Diet modification – Decrease cow’s milk – Increase iron-rich foods • Iron therapy – 4 to 6 mg/kg of elemental iron • Increased absorption with Vit C Kezelés • Parenteral iron – 2-3% anaphylaxis – No advantage • PRBC transfusion – RARELY necessary – Only if hemodynamically unstable – 3 to 5 cc/kg at a time, watch for CHF Kezelésre adott válasz • 12-24 hours – Intracellular replaced – Subjective improvement – Increased appetite • 36-48 hours – Bone marrow response – Erythroid hyperplasia • 48 to 72 hours – Retics increased, peak at around 5 to 7 days Kezelésre adott válasz • 4 to 30 days – Increased Hemoglobin • 1 to 3 months – Repletion of iron stores • Treat for a total of at least 3 months Sikertelen kezelés • Poor compliance – 10% GI side effects – Poor taste • Ongoing blood loss • Wrong diagnosis Különböző anaemiák jellemzői Parameterek, Apl. Folate, B12 Fe def. indexek Anaemia def. MCV Hgb conc RBC Hgb conc Rets Se Bil Hemolysis Vérvesztés Mikor forduljunk gyermek hematológushoz? • • • • • • Neutropenia and /or thrombocytopenia Significant adenopathy/organomegaly Suspected hemolysis Hemodynamic compromise and/or HCT < 20% Suspected thalassemia major or sickle cell dis Failure to respond to therapeutic iron trial Hereditary spherocytosis • Prevalence: 1/5000 • Etiology: Autosomal dominant, 25% have no previous family history • Most common molecular defects: spectrin, ankyrin Clinical manifestations • Hyperbilirubinemia in the neonate • Some children stay symptomeless until adulthood, others have recurrent hemolytic crisis • After infancy the spleen is enlarged • Gallstone • Icterus Treatment • Transfusion • Splenectomy Diamond-Blackfan anemia • Diamond-Blackfan anemia (DBA), also known as Blackfan–Diamond anemia and Inherited erythroblastopenia, is a congenital erythroid aplasia that usually presents in infancy. DBA patients have low red blood cell counts (anemia). The rest of their blood cells (the platelets and the white blood cells) are normal. This is in contrast to Schwachman-Diamond syndrome, in which the bone marrow defect results primarily in neutropenia, and Fanconi anemia, where all cell lines are affected resulting in pancytopenia. Clinical picture • Diamond-Blackfan anemia is characterized by anemia (low red blood cell counts) with decreased erythroid in the bone marrow. This usually develops during the neonatal period. About 47% of affected individuals also have a variety of congenital abnormalities, including craniofacial malformations, thumb or upper limb abnormalities, cardiac defects, urogenital malformations, and cleft palate. Low birth weight and generalized growth delay are sometimes observed. DBA patients have a modest risk of developing leukemia and other malignancies Diagnosis • Typically, a diagnosis of DBA is made through a simple blood count and a bone marrow biopsy. • A diagnosis of DBA is made on the basis of anemia, low reticulocyte (immature red blood cells) counts, and diminished erythroid precursors in bone marrow. Features that support a diagnosis of DBA include the presence of congenital abnormalities, macrocytosis, elevated fetal hemoglobin, and elevated adenosine deaminase levels in red blood cells. • Most patients are diagnosed in the first two years of life. However, some mildly affected individuals only receive attention after a more severely affected family member is identified. • About 20-25% of DBA patients may be identified with a genetic test for mutations in the RPS19 gene.(19q13.2) Treatment • Corticosteroid • Transfusion • Bown marrow transplantation Transient erythroblastopenia of childhood (TEC) • Acquired erythroid bone marrow failure – Unknown etiology • • • • 18 mos to 2 yrs Often follows viral illness Child otherwise healthy Resolves spontaneously – Weeks to months TEC • Lab findings – Normocytic anemia (Hb 50-70, sometimes as low as 20) – Low retic count – No evidence of hemolysis – Other cell lines unaffected • Treatment – Supportive – Transfusion if symptomatic Hemoglobinopathies • Thalassemia – Decreased or absence of production of one or more globin chains • Alpha, beta, and variants • Sickle cell disease – Structural defect of beta-globin chain Thalassemia • Epidemiology – Prevalent in certain populations • Africa, Middle East, Asia, and Mediterranean population • Pathogenesis – Decreased or absent synthesis of one or more globin chains • Imbalance in number of chains – Precipitation of unstable Hb • Hemolysis occurs Alpha-Thalassemia • Common in Asian and black populations • Phenotype depends on number of deletions – 1-gene deletion • Silent carrier, no anemia – 2-gene deletion (trait) • Mild hypochromic, microcytic anemia – 3-gene deletion (Hemoglobin H) • Severe anemia • Hb Bart (gamma globin tetramers) – 4-gene deletion • Incompatible with life • Hb Bart Beta-thalassemia • Mediterranean or Southeast Asian origin • Phenotype depends on number and type of mutations – Minor • Microcytic anemia – Intermedia • Moderate to severe anemia – Major • Severe anemia, transfusion dependant Diagnosis • Family history, ethnic origin • CBC – Microcytic anemia • Normal or increased ferritin • Hb electrophoresis – Decreased HbA, increased HbF – Abnormal Hemoglobins • Gene studies Treatment • Alpha trait – None – Counseling • Severe anemia – Transfusion – Watch for iron overload – Chelation therapy – Splenectomy Sickle Cell Disease • Defect of beta-globin chain – Amino acid substitution (valine for glutamine) • Prevalent in certain populations – African, Caribbean, Middle Eastern, Indian, Mediterranean populations Hb susceptible to deoxygenation, acidosis, temperature, dehydration – RBC distorted into sickle shape – Results in tissue ischemia and infarction – Shortened RBC survival Sickle Cell Disease • Manifestations (only in disease, not if trait) – – – – – Bony crisis Chest crisis Strokes Splenic sequestration Aplastic anemia • Susceptibility to infections; autosplenectomize – Encapsulated organisms • Need penicillin prophylaxis Treatment • Pain control – NSAIDs, opiates • • • • • Hydration Antibiotics if febrile Transfusions Exchange transfusions Hydroxyurea