Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
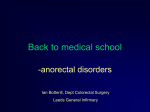
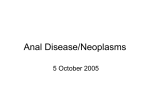
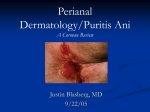
Anal Fissure and Fistula By Mike Parenteau Anal Fissure an unnatural crack or tear in the anus, usually extending from the anal opening and located posteriorly in the midline. This location is probably because of the relatively unsupported nature of the rectal wall in that location. Etioloogy / Pathophysiology Most anal fissures are caused by stretching of the anal mucosa beyond its capability. Various causes of this fissure include: Straining to defecate, especially if the stool is hard and dry Severe and chronic constipation Severe and chronic diarrhea Etioloogy / Pathophysiology Crohn's disease and Ulcerative colitis Anal sex or dildo use Anal stretching Insertion of foreign objects into the anus Tight sphincter muscles Excessive anal probing Clinical Mainfestations The symptoms of anal fissure include: Pain during, and even hours after, defecation Visible tear in the anus Blood on the stool or on toilet paper or toilet bowl Constipation Burning, possibly painful, itch Medical Management Most anal fissures are shallow or superficial (less than a quarter of inch or 0.64 cm deep). These fissures self-heal within a couple of weeks. While waiting for the fissure to heal, topical or suppository containing antiinflammatory agents and local anesthetic can be used. Furthermore, treatment used for hemorrhoid such as eating a high-fiber diet, using stool softener, taking pain killer and having a sitting bath Medical Management Painful deep fissures, on the other hand cut through the sphincter muscle thus making it prone to spasm, which exacerbates the fissure and aborts the healing process. Medications such as nitroglycerine and nifedipine ointments can relax the sphincter muscle Medical Management Surgical intervention may be required for persisting deep anal fissures unresponsive to the above conservative measures. Procedures include: Internal lateral sphincterotomy or excising a portion of the sphincter Anal dilation or stretching of the anal canal is no longer recommended because of the unacceptably high incidence of fecal incontinence Anal Fistula Abnormal opening on the cutaneous surface near the anus. Abnormal connection between the epithelialised surface of the anal canal and (usually) the perianal skin Usually this is from a local crypt abscess and also is common in Crohns. Symptoms Anal fistulae can present with many different symptoms: Pain Discharge - either bloody or purulent Pruritus ani - itching Systemic symptoms if abscess becomes infected Objective The opening of the fistula onto the skin may be seen The area may be painful on examination There may be redness An area of induration may be felt thickening due to chronic infection A discharge may be seen Medical Management Doing nothing - a drainage seton can be left in place long-term to prevent problems. This is the safest option although it does not definitively cure the fistula. Conversion to a cutting seton - this involves a similar process to a draining seton but the suture is tied tightly. This gradually cuts through the muscle and skin involved, leaving behind a small area of scarring. This cures the fistula in most cases, but can cause incontinence in a small number of cases, mainly of flatus (wind). Medical Management involves an operation to cut the fistula open and let it heal naturally. This cures the fistula but leaves behind a scar, and can cause problems with incontinence. This option is not suitable for complex fistulae, or those that cross the entire anal sphincter. Fibrin glue injection is a method explored in recent years, with variable success. It involves injecting the fistula with a biodegradable glue which should, in theory, close the fistula from the inside out, and let it heal naturally. This method is perhaps best tried before all others since, if successful, it avoids the risk of incontinence, and creates minimal stress for the patient. Medical Management Fistula plug is an "advanced" version of the fibrin glue method. It involves "plugging" the fistula with a "plug" made of porcine small intestine submucosa (sterile, biodegradable), fixing the plug from the inside of the anus with suture, and, again, letting the fistula heal "naturally" from the inside out. According to some sources, the success rate with this method is as high as 80%. Medical Management Endorectal advancement flap is a procedure in which the internal opening of the fistula is identified and a flap of mucosal tissue is cut around the opening. The flap is lifted to expose the fistula, which is then cleaned and the internal opening is sewn shut. After cutting the end of the flap on which the internal opening was, the flap is pulled down over the sewn internal opening and sutured in place. The external opening is cleaned and sutured. Success rates are variable and high recurrence rates are directly related to previous attempts to correct the fistula. Plug