Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
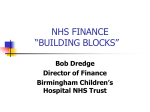
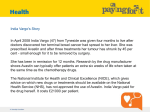
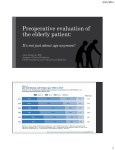
NDA and Age UK Improving Later Life 11 March 2013 London Older people are changing and they're here to stay. Some interesting challenges for healthcare! Finbarr Martin, Geriatrician Guys & St Thomas’ Hospital and Kings College London Current public and media focus Bad press and negative reports about • Variations in access– post code lottery • Dignity in care • Continuity of care in hospitals and primary care • Variation in performance of acute hospitals • Poor integration with community and primary care Older people are not all the same “usual” older people are heterogenous re – sensory impairments – physiological ‘abnormalities’ eg lung function – metabolic changes eg glucose impairment – psychosocial factors eg. cognition, engagement (Rowe and Kahn, Science, 1987) These variable developments are life long and multi-factorial And many are reversible/preventable this justifies a more optimistic and holistic approach to public health and clinical practice How and why individuals differ Genetics inc chance changes in development Maternal and early life factors Society and Lifestyle etc Events and illnesses and chance Frailty Specific diseases Spectrum of health and capacity And older people are changing ( rectangularisation to elongation of age distribution) Distribution of death England 1841 - 2006 100% Around 18% of all deaths were before 65 in 2006 –same proportion as in 1991 90% 1981 1991 80% 1941 70% 2001 60% 50% 1841 2006 40% 30% 20% 10% 0% 1 5 9 13 17 21 25 29 33 37 41 45 49 53 57 61 65 Source: mortality.org, originally ONS 69 73 77 81 85 89 93 97 101 105 109 5 As a result………… • Most older people now live long enough – To have several long-term conditions (+ multiple medications) • eg Respiratory, cardiac, diabetes – to develop sensory impairment, sarcopenia, inflammaging • Many also develop – dementia, osteoporosis, cataracts etc – homeostatic dysregulation • Resulting in frailty and “geriatric syndromes” What is frailty about? • • • • Widespread change just short of decompensation Much of this is NOT condition specific But variable between individuals - unpredictable Propensity to additional minor stressors mental and physical • Thus possibility of multisystem failure • And linkages between mechanisms of apparently different problems, – Eg delirium and sarcopenia – inflammaging and low IGF-1 Frailty “summarises” prediction of outcomes Rockwood and Mitniski A J Gerontol 2007 Getting healthcare fit for a modern population • People aged 65+ are ~ 17 % of the population • And use 65% of acute hospital bed-days • >50% of the patients having surgery, (>major) • Use nearly half the NHS total budget • Over half social services’ budgets • Over £3 billion for NHS continuing care So, are the older population a challenge to the NHS? OR, are older people core business?? People with long-term conditions have high health service use, 69% total health spend. People with limiting LTCs are the most intensive users of the most expensive services 100% % of services used 80% Limiting LTC 60% 40% 20% 0% Number of people GP consultations Practice Nurse appointments Outpatient and A&E attendances Type of service Source: 2005 General Household Survey. 10 No LTC Non-limiting LTC Limiting LTC 25 May, 2017 Inpatient bed days The official intention “A comprehensive service available to all based on need and irrespective of age, gender, ethnicity etc.....reflecting needs and preferences of patients families and carers” NHS Constitution 2008 “Discrimination has no place in a fair society which values all its members. ...services should be differentiated by age only when justifiable or beneficial” Equality Act 2010 Some of the challenges to make this reality • • • • • • Changing expectations Overcoming the social – clinical divide in care Elective and emergency surgery Management of long term conditions Reaching the most vulnerable people Recognising and respecting the end of life Right patient –wrong place? • Many staff regarded their hospital wards as the wrong place for older people • And too many senior politicians and policy experts seem to agree Tadd W et al. Dignity in Practice: An exploration of the care of older adults in acute NHS Trusts. NIHR Service Delivery and Organisation Programme; 2011. Right place - wrong skills • Clinical challenges of sudden change Subtle presentation of serious illness Functional decline is always “suspicious” • Co-morbidity is common • Loss of reserve is common – Physiological – Psychosocial Solution – embed the right skills as “routine” NCEPOD Report 2010 • >1000 deaths of surgical patients 80+ years • Report highlights suboptimal management of common post-operative complications • Gap between policies, guidelines and routine clinical practice. • Assessment and clinical skills were too narrow to anticipate and react to likely events • Interdisciplinary collaboration is essential National inter-disciplinary collaboration The Blue Book and the NHFD Local proactive joint care - example from GSTT: Proactive care of Older People having surgery -“POPS” Surgical Outpatients/PAC Pre-operative CGA Proactive referral of patients aged 65+ Consultant Screen to identify risk Clinical Nurse Specialist Including “medically unfit for surgery” Occupational therapist Physiotherapy Post Discharge Social worker Intermediate Care Patient education Links with primary care/ social care Specialist clinic follow up (falls etc) Preadmission Liaison Hospital Admission Surgical team Post-op consultant geriatrician and specialist nurse interventions Anaesthetists Therapy liaison Discharge planning GP and Community services Patient Long term conditions • Estimating potential benefit is complex – Attributing risk in context of co-morbidity – Effects on LE, independence and quality of life • Estimating risks and burdens is complex – Factoring in frailty • Enabling real co-decision making • Relatively evidence free End of life care - recognition Trajectories in the final 12 months of life What needs to be done? • Older people with problems are to be expected • Frailty and geriatric syndromes can be identified comprehensive geriatric assessment (CGA) • “Complications” can be predicted • Expert teams + up-skilling general services • The future is multidisciplinary in clinical practice and clinical governance • Better care is often cheaper care in the end, so NHS must get better to survive economically Can gerontology research help? • How to incorporate into clinical practice the individual adaptive strategies to deal with differences and difficulty • How to enable older people to navigate and make choices, even whilst receiving crisis stabilisation • How to provide care without creating ghettos • How to address the intergenerational difference between care receivers and givers …….As well as a host of bio-gerontology questions about ageing frailty and promoting recovery