Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
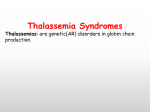
Comprehensive Patient Blood Management Avoiding Allogeneic Transfusion: A Case Study in Patient Blood Management Irwin Gross, M.D. May, 2012 Disclosures Irwin Gross, MD • Medical Advisory Board, Strategic Healthcare Group Learning Objectives • Name the three pillars of patient blood management • Name three adverse outcomes associated with transfusion • List four tools that can be used in patient blood management to limit the risk of transfusion • Describe the role of parenteral iron in treating anemia • Name two types of perioperative autologous blood collection • List two relative contraindications to cell salvage What is Patient Blood Management: The Three Pillars Optimize erythropoieis Minimize bleeding & blood loss © Axel Hofmann/Shannon Farmer – SHEF Meeting Perth August 2010 Harness & optimize physiologic tolerance of anemia Anemia independently associated with increased: • morbidity 5-75% incidence in patients presenting • hospital length of stay for elective surgery • likelihood of transfusion Shander 2004 Anemia • mortality Spahn DR. Anesthesiology 2010; 113(2) 1-14 Beattie WS, et al Anesthesiology 2009; 110(3) 574-81 Dunne JR, et al J Surg Res 2002; 102: 237-44 Shander A. Am J Med 2004; 116(7A) 58S-69S Bleeding associated with increased • Morbidity • ICU and hospital length of stay • Mortality Procedural • Elective surgery ~0.1% bood loss & Bleeding • Subgroups: • Vascularbleeding 5–8% • Up to 20% with severe bleeding • Major organ damage 30–40% Causes • On average 75 – 90% local surgical interruption or vessel interruption • 10–25% acquired or congenital coagulopathy Shander A. Surgery 2007 RBC transfusion independently associated in a dose-dependent relationship with increased: •Morbidity •ICU and hospital length of stay •Mortality Transfusion Beattie WA, et al Anesthesiology 2009 Murphy GJ, et al Circulation 2007 Salim A, et al J Am Coll Surg 2008 Bernard AC, et al J Am Coll Surg 2008 Hearnshaw SA, et al Aliment Pharmacol Ther 2010 Blair SD, et al Br J Surg 1986 Impact of Transfusion on Patient Outcomes Author (year) Koch et al (2005) Murphy et al (2007) Surgenor et al (2009) Pedersen et al (2009) Nikolsky et al (2009) van Straten et al (2010) D’Ayala et al (2010) O’Keeffe et al (2010) Veenith et al (2010) Population Cardiac surgery n Impact of Blood Transfusion 11,963 - Higher postop mortality rate - Higher postop morbidity rate (RF, prolonged ventilatory support, serious infection, cardiac complications, & neurologic events) Cardiac surgery 8,598 - Higher mortality rate - More ischemic complications - More infectious complications Cardiac surgery 3,254 - Decreased survival after cardiac surgery Total hip 4,508 - Higher mortality rate replacement - More pneumonia PCI after MI 2,060 - Higher 30-day and 1-year mortality rate Cardiac surgery 10,435 - Worse early survival Lower extremity 300 - More postop adverse events amputation - Longer ICU/hospital stay Lower extremity 8,799 - Higher mortality rate revascularization - More pulmonary complications - More infectious complications Elderly undergoing 874 - Higher mortality rate cardiac surgery - Longer ICU/hospital stay Physiologic Impact of Red Cell Transfusion Author (year) Population Babineau et Postoperative al (1992) Silverman et Septic shock 21–88 yrs al (1992) Marik et al Septic adults (1993) Lorente et al Septic adults (1993) Gramm et al Septic shock 46 ± 3 yrs (1996) Casutt et al Postoperative 32–81 yrs (1999) Fernandes et Septic shock 18–80 yrs al (2001) Walsh et al Euvolemic anemic critically ill (2004) patients Suttner et al Volume-res mechanically (2004) ventilated patients Mazza et al SIRS/Sepsis (2005) n Blood Transfused ↑Hb ↑DO2 ↑VO2 ↓Lactate 31 328 ± 9 mL Yes Yes No No 21 2 units Yes Yes No No 23 3 units Yes Yes No No 16 2 units Yes Yes No ? 19 2 units Yes No No ? 67 368 ± 10 mL Yes Yes No ? 10 1 units Yes No No No 22 2 units Yes ? ? No 51 1 or 2 units vs. 100% FIO2 1–3 units Yes Yes No ? Yes ? ? No 29 What are “Transfusion Alternatives”? • • • • • Optimize hemodynamics and oxygenation Physiologic tolerance of anemia Use of erythropoietic stimulating agents Use of intravenous iron Minimizing blood loss – Manage coagulopathy – Anti-fibrinolytics – Perioperative cell collection and reinfusion Our Patient • A 68 year old retired immunology professor requires revision of a prior right hip arthroplasty due to aseptic loosening with severe instability and functional limitation • Past medical history is significant for rheumatoid arthritis and Type 1 vWD • Patient underwent a recent hemicolectomy for T1N0M0 (Stage 1) colon cancer at another hospital without a blood management program Our Patient • The patient is referred to an orthopedic surgeon • A total hip arthroplasty is planned • The patient, having read the article summarized on the next slide, requests that transfusion of allogeneic blood be avoided unless surgical bleeding is life threatening Influence of Transfusion on Colorectal Cancer Recurrence • Cochrane meta-analysis involving 12,127 patients • Evaluated role of transfusion in colorectal cancer recurrence • Overall OR for recurrence was 1.41 (95% CI 1.20-1.67) in transfused patients Amato, A, et al. Cochrane Database System Rev 2006;(1): CD005033 Reasons to Avoid Transfusion • Transfusion is associated with: – – – – Increased perioperative infections Increased length of stay Increased short term mortality Transfusion reactions, some life threatening – Increased incidence of cancer recurrence and decreased disease-free and long term survival Pre-operative Screening for Anemia • The patient should be screened for anemia -he is undergoing surgery with significant blood loss – CBC – If CBC shows anemia (< 13 g/dL) then additional lab tests required • Iron, iron binding capacity, ferritin, Vitamin B12, creatinine, reticulocyte count • Folate if MCV > 100 fl Scheduling • The ideal window to evaluate a patient for pre-operative anemia is 21-30 days before surgery – Medicare will not pay for lab studies > 30 days • If commercial insurance or known history of anemia or co-morbidity associated with anemia, screen sooner (more time to treat anemia is better) – Treatment of chronic anemia with iron, EPO or both requires (at least) 3-4 weeks – The clinical condition may require the case to be scheduled sooner (unstable cardiac disease; cancer diagnosis) Scheduling • If procedure is truly elective, and anemia cannot be managed in the available time, surgery should be deferred • Occasional patients will need referral to specialist: hematologist, gastroenterologist, etc. Our Patient • Surgery is scheduled to take place in 24 days. Lab results are as follows: – – – – – – Iron: Total iron binding: % Saturation: Ferritin Hemoglobin Reticulocyte count 20 ug/dL (28-170) 250 ug/dL (261-478) 8% (15-45) 600 ng/mL (45-500) 10.1 g/dL (14-17) 25 Th/uL (22-98) Our Patient • Diagnoses – Iron deficiency anemia (blood loss from recent chronic lower GI blood loss and colon surgery treated with enteral iron sulfate) • Enteric iron is ineffective when there is inflammation, e.g. rheumatoid arthritis – Anemia of Inflammation (functional iron deficiency – patient has rheumatoid arthritis) • Recommended Rx – Intravenous iron – Consider erythropoietin Anemia Management: Intravenous Iron / EPO • “Standard” regimen for perioperative anemia; hemoglobin between 10-13 g/dL; non-vascular, non-cardiac surgery – 40,000 units of erythropoietin on days 21, 14, and 7 pre-op, and on day of surgery • Patient must have transferrin saturation > 20% and ferritin > 100 ng/ml to be reimbursed by Medicare – 200 mg I.V. iron sucrose with each EPO dose – 1 mg folate, p.o., daily – 500 mg Vitamin C, twice daily Should We Use EPO and Iron or Iron Alone? • Reasons to use EPO: – Patient has only 24 days till surgery with Hgb of 10.1 g/dl – EPO improves rate of response to iron – Rheumatoid arthritis may result in decreased endogenous EPO production • Reasons not to use EPO – Increased VTE risk – Some data suggests shortened survival and time to recurrence in some malignancies with EPO – But, transfusion is associated with shortened survival and time to recurrence in malignancy and increased perisurgical mortality JAMA. 2008;299 (8): 914-924 Anesthesiology. 2009 Mar; 1 10(3):547-81 Our Patient • After discussion of the risks and benefits of EPO (informed consent), the patient consents to the use of EPO – Orders are written for three doses of EPO between now and surgery, by subcutaneous injection (600 units/kg) – A fourth dose of EPO will be given on post-op day one if hemoglobin is less than 8.0 g/dL – Goal: lowest dose to avoid transfusion Iron Administration • Intravenous iron should always be given during a course of treatment with EPO unless iron saturation is > 35% or ferritin > 1,000 ng/ml • Three “classes” of IV iron available in U.S. – – – – Minimal cross reactivity re: reactions Iron sucrose and iron gluconate Ferumoxytol (paramagnetic nanoparticle) Iron dextrans • Fewer ADE’s with low molecular weight iron dextran than high molecular weight iron dextran) David H et al Oncologist 12:231-242, 2007 J Am Soc Nephrol 18: 975-984, 2007 Iron Sucrose vs. Iron Dextran vs. Ferumoxytol • Iron sucrose – Most appropriate for serial encounters or total dose of 300 mg or less – Comes in 100 mg vials – Maximum dose we use is 300 mg in 100 ml saline over 60 minutes – Lowest rate of serious adverse drug reactions – Characteristics and use of iron gluconate are similar Iron Sucrose vs. Iron Dextran vs. Ferumoxytol • Low molecular weight iron dextran – Best option for total dose iron replacement (TDI) – Use when single encounter and iron required exceeds 300 - 500 mg – Requires administration of test dose – Remaining dose given over 1 – 2.5 hours, up to 1,500 mg – Low incidence of A.D.E.’s (3.3 / million doses) – I recommend against high molecular weight iron dextran Iron Sucrose vs. Iron Dextran vs. Ferumoxytol • Ferumoxytol – Can administer 510 mg of iron in 17 seconds (30 mg/sec) – No test dose required – Least experience, but seems to have a good safety profile – Higher drug cost than other options What about Enteric Iron? Hepcidin, Inflammation and Iron Metabolism J Am Soc Nephrol 18: 394-400, 2007 Contraindications to Iron • Theoretical concern in infection / sepsis – some bacteria use iron as a growth factor • But remember, transfused blood provides iron in the form of heme • Immunomodulation increases risk of infection S. aureus and Iron-regulated Surface Determinant (IsdB) . Lowy FD. N Engl J Med 2011;364:1987-1990. Our Patient • With each EPO dose, we decide to give our patient 200 mg of I.V. iron sucrose (600 mg total) • Additional iron will be given post-op based on post-op hemoglobin – Approximately 500 mg iron required to replace depleted stores – Need additional 150 mg for each g/dL decrease in hemoglobin below 13 g/dL Our Patient • On the day of admission, our patient has a hemoglobin of 12.8 g/dL and an elevated reticulocyte count • The patient signs informed consent for transfusion only if needed to prevent death from severe hemorrhage Intraoperative Management – Day of Surgery • Acute normovolemic hemodilution (ANH) • Intraoperative autologous blood collection and re-adminstration (“cell salvage”) • DDAVP • Anti-fibrinolytics (e.g. tranexamic acid • Meticulous surgical hemostasis Acute Normovolemic Hemodilution • Conservation of red cell mass by decreasing hematocrit of shed blood • Fresh whole blood, with intact platelets and clotting factors, available at end of case for transfusion • Studies show reduced blood loss in joint arthroplasty, spine surgery, cardiac, hepatic resection, major colon operations, and radical cystectomy Acute Normovolemic Hemodilution – How Is It Done • Replace volume with crystalloid or colloid – We generally use HES (tetrastarch) • Usually requires 10 minutes / unit • Proper labeling • Blood typically remains at room temperature in O.R. prior to reinfusion • Generally re-administered in reverse order of collection – most hemodiluted given first – unit with most clotting factors last Our Patient • We anticipate the possibility of 2 liters of blood loss – Based on the professor’s body weight and hemoglobin, up to four units might be collected before surgery; we collect two – Replaced with 1,000 ml of hydroxyethyl starch • We use tetrastarch – His hemoglobin at the start of the procedure would be 10.0 g/dL Intraoperative Cell Salvage • Indicated when significant blood loss is anticipated (may be as little as 250 ml in a small patient with anemia) • Full set-up when significant blood loss is likely • Collection only set-up when significant blood loss is possible • Salvage efficiency is technique dependent – Low suction pressure – Eliminate skimming – Wash sponges Intraoperative Cell Salvage • Relative contraindications – Bacterial contamination – Some foreign material (antibiotics, topical hemostatic agents, methyl methacrylate) – Malignancy • Most contraindications can be addressed through a combination of increased wash volume and filtration – Two suctions, one for waste – Leukocyte reduction filter for bacteria and tumor cells – Irradiation for tumor? Blood Salvage and Cancer Surgery: Meta-analysis Conclusion: IBS is not inferior to traditional intraoperative allogeneic transfusion with regard to increased cancer recurrence or development of metastasis Waters et al, Transfusion doi: 10.1111/j.1537-2995.2011.03555.x Our Patient • We decide to set up the Cell Saver in anticipation of significant blood loss. • If the patient was having surgery for tumor, a leukocyte reduction filter would be used • Waste suction will be used to clear field if topical hemostatic agents used Pharmacologic Agents to Limit Blood Loss • Desmopressin (DDAVP, Stimate) – Releases von Willebrand’s factor from endothelial cells and increases factor VIII levels – 0.3 mcg/kg in 50 mL over 15-30 minutes – Can be repeated several times – Minimal evidence of efficacy in reducing surgical blood loss except in vWD Pharmacologic Agents to Limit Blood Loss • Antifibrinolytic agents – Amicar – Tranexamic Acid • Inhibits clot lysis • 10-30 mg/kg loading dose, followed by 1-2 mg/kg/hr • Decrease dose for renal insufficiency • Good evidence base: 30% reduction in blood loss in major orthopedic cases including multilevel spine and TJA Br J Anaesth 2004; 93:842-58 Pharmacologic and Other Agents to Limit Blood Loss • Topical hemostatic agents – Fibrin glue (thrombin and fibrinogen concentrate) – Mechanical hemostatic agents (collagen, cellulose, gelatins, etc.) – Active hemostatic agents • Bovine or human thrombin • Gelatin plus thrombin • Synthetic glues • Saline-cooled radiofrequency “cautery” Our Patient • Surgeon plans to use topical hemostatic agents as needed • This patient has a history of mild type 1 vWD – Plan to administer 30 mcg of DDAVP 15 minutes before surgery • Will administer 20 mg/kg of tranexamic acid just before the start of surgery and begin an infusion of 2 mg/kg/hr – Will discontinue infusion when surgery is completed • Some surgeons use TXA topically Day of Surgery • Both the femoral and acetabular component require revision • Unexpected surgical bleeding is encountered Intraoperative Course • Four cell “salvage” runs return a total of 1,075 ml of processed blood with an average hematocrit of 55% (equivalent to about 3 units from the blood bank) • The two ANH units are returned toward the end of surgery Post-op Day One • The patient’s post-op hemoglobin is 7.9 g/dL and our patient has been extubated • He is hemodynamically stable • As planned, a fourth dose of erythropoietin is administered • The surgeon initiates the “minimum blood volume” phlebotomy protocol to minimize blood lost for diagnostic testing Strategies for Reducing Phlebotomy Blood Loss • Eliminate “extra tubes” • Eliminate under and over draws • Individual nurse and phlebotomist education • Selection of testing equipment with low requisite sample volume • Increased point-of-care testing • Reduce unnecessary testing • Reduced tube size • Selective use of microtainers Highly Conservative Phlebotomy • Using a highly conservative protocol, median phlebotomyassociated blood loss (PBL) in the ICU was reduced 80% (40 ml vs. 8 ml) • Mean drop in hemoglobin in ICU decreased from 2 gm/dl to 1.2 gm/dl Harber CR. Anesthesia and Intensive Care 34:4, 2006 If on post-op day one… • • • • Our patient’s hemoglobin is 6.7 g/dL His reticulocyte percentage is 7.8% His iron saturation is 13% He is walking 15 feet with assistance, but becomes short of breath and feels tired What would you do? Post-op Iron Therapy • Post-op inflammatory response creates functional iron deficiency due to increased hepcidin (our patient also has RA) – Labs show decreased transferrin saturation (% saturation) below 20% • Oral iron salts (e.g. ferrous sulfate) are poorly absorbed and prolong post-op ileus Our Patient • We decide to administer 900 mg of low molecular weight iron dextran based on the patient’s IBW of 70 kg and hemoglobin deficit of 6 g/dL • Daily folate, 1 mg for one month • Daily Vitamin C for one month • Patient is discharged home on postop day 2 with a hemoglobin of 8.1 g/dL • One month after surgery, the patient is recovering nicely with a hemoglobin is 11.9 g/dL Patient Blood Management: The Three Pillars Optimize • Pre-op anemia screening erythro• ESAs poieis • Intravenous Iron • ANH • Cell Salvage • DDAVP • Minimize TXA •bleeding Topical & hemostatics loss • blood Meticulous surgical hemostasis • Minimize phlebotomy © Axel Hofmann/Shannon Farmer – SHEF Meeting Perth August 2010 Harness & • Optimize optimize hemodynamics •physiologic Optimize oxygenation tolerance of • Low hemoglobin threshold for anemia transfusion