Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
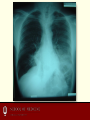
Approach to Neurologic Emergencies Indiana University School of Medicine Emergency Medicine Clerkship Objectives • From the IU EM Didactic Learning Objectives: – 13. Discuss the differential diagnosis of patients presenting to the Emergency Department with altered mental status. – 14. Identify the appropriate candidate for thrombolytic therapy in the Emergency Department. – 36. Discuss the approach to the actively seizing patient, new onset seizure patient, chronic seizure patient, and the febrile seizure patient in the Emergency Department. • NB: Febrile seizures not covered in this lecture; covered in Peds lecture Case #1 • You are working a late evening shift and receive an EMS call – 94 year old female; unknown PMH – Normally A&O x3 at baseline; lives independently – Daughter called to “check in this evening” and had no response – EMS found patient lying on floor, confused Case #1 • EMS glucose—146 • The medic tells you that the patient’s pupils were slightly sluggish, so he gave a dose of Narcan without any response Coma Cocktail • Not routinely given, but considered • Glucose – Check early and administer D50 if low • Consider empiric D50 if no meter available • Naloxone (Narcan) – Reverses the effects of narcotics that may be affecting mentation and or breathing • Use if patient apneic or suspect narcotic toxicity – May precipitate withdrawal in chronic users • Thiamine – Consider in alcoholics • Does our patient have dementia or delirium? Delirium Dementia Sudden Insidious Course/day Fluctuating Stable Consciousness ↓ / Clouded Alert Attention Abnormal Normal Cognition Abnormal Abnormal Orientation Impaired Often impaired Hallucinations Usu visual Absent Delusions Transient Absent Asterixis/tremors Absent Onset Movements Altered Mental Status-Differential Dx • • • • • A-Alcohol E-Endocrine I-Insulin- Diabetes O-Oxygen and opiates U-Uremia, hypertensive encephalopathy • • • • T-trauma, temperature I-infection P-Psychiatric S-Space occupying lesion, stroke, subarachnoid hemorrhage, shock Altered Mental Status-Differential Dx • Not all conditions listed on previous slide need a test to rule them out • Use information obtained from history, physical examination, family to narrow differential diagnosis and guide approach Case #1 • On arrival, the patient is awake and alert, making moaning noises and not following commands well • VS: P 86 BP 124/84 RR 24 T 100.8 Biox-84% on RA • Exam – Pupils 2 mm and reactive; no focal neurologic weakness – Left lower lung rales Vital Signs • Often provide clue to underlying etiology • Hypoxia- either as a cause of confusion or as a result of hypoventilation because of neurologic insult – Needs to be rapidly recognized and treated Vital Signs-continued • Hypotensive-shock – May see tachycardia as well • Hypertensive- consider intracranial hemorrhage • Fever – Moves infectious etiologies higher on the list – Although some septic patients may be afebrile or hypothermic Altered Mental Status-Workup • Focus based on history and exam as possible – Can be difficult especially when limited information present in H&P • For our patient – CBC, BMP, ECG, U/A, CXR Case #1 • WBC 8,000 • BMP WNL • ECG sinus tachycardia without ischemic change • CXR next slide Case #1 Case #1 Diagnosis • Community Acquired Pneumonia – Causing hypoxia and resulting mental status changes • Patient admitted for IV ATBx and oxygen therapy Case #2 • 75 year old male • Fell off ladder two days ago • Has been increasingly confused at home Case #2 • Vitals T 98.4 F BP 178/104 HR 72 RR 14 Biox 97% • Patient lying on the stretcher • Eyes closed, responds to voice • Speech confused • Moves all extremities spontaneously, follows commands slowly GCS • What’s his GCS score? GCS • • • • Glasgow Coma Scale Minimum score = 3 Maximum score = 15 Assess eye opening, motor response, verbal response GCS-Mnemonic • • • • Helps with maximum score in each category Eyes- “Hey four eyes” (4) Motor- “Six cylinder motor” (6) Verbal- “Jackson Five” (5) GCS-Eye Opening • 4-Spontaneously • 3-To Verbal • 2-To pain • 1-None GCS-Best Verbal Response • 5- Oriented, converses • 4-Disoriented, confused • 3-Inappropriate words • 2-Incomprehensible sounds • 1-None GCS-Best Motor Response • 6-Obeys commands • 5-Localizes pain • 4-withdraws to pain • 3-decorticate posturing • 2-decerebrate posturing • 1-none Obtaining a History • In the altered patient, important to contact family members, nursing staff at ECF, caregivers • Review the EMR, look in wallet for alerts/medication lists • They will often be the only potential history source and can provide crucial information History-Altered Mental Status • • • • Focus upon trying to find out their baseline Recent illnesses? New medications? Ingestions/Polypharmacy? Pupils-Altered Mental Status Generally preserved in metabolic causes – Unilateral dilated pupil in unresponsive patient • Think uncal herniation secondary to bleed/space occupying lesion Pupils-Altered Mental Status • Bilaterally fixed dilated pupils= anoxic injury • Pinpoint, nonreactive without systemic response to Naloxone= pontine injury Physical Exam-Altered Mental Status • Look for pallor (anemia), needle tracks (IVDU), cyanosis (hypoxia) • Breath-smell for ETOH or ketones (fruity) • Head-look for abrasions, contusions, craniotomy scars, shunts • Eyes-icterus, fundoscopic, gaze preference Physical Exam-Altered Mental Status • Mouth-look for tongue lacerations (on the sides) suggesting seizure • Neck-evaluate for meningismus; remember to have a low threshold to immobilize the cervical spine if there is any question of trauma • Lungs-wheezing or abnormal breath sounds; suggesting COPD leading to hypercarbia Physical Exam-Altered Mental Status • Abdomen-ascites, stigmata of liver failure that might tip you off to hepatic encephalopathy Case #2 • Concern for traumatic intracranial hemorrhage given history of fall and new onset altered mental status • CT obtained Case #2 Case #2 • Neurosurgery consulted • Patient admitted to NSICU Case 3 • 67 yo male brought in by ambulance with 2 hour history of right sided weakness and facial droop • PMH: HTN, DM • VS: T: 36.3 BP: 130/80, HR: 90, SpO2: 99% on RA Case 3-Exam • Gen-awake, alert, GCS 15 • PERRLA, EOMI, no nystagmus • Right facial droop; some slurring noted on spontaneous speech • 4/5 strength RUE/RLE; remainder nonfocal • Follows commands well Acute Stroke • #1 priority—is this patient a candidate for thrombolytics? • Safe, effective administration of thrombolytics is time and criteria dependent • Failure to follow time/criteria guidelines increases the risk of iatrogenic intracranial bleed Acute Stroke-Initial Priorities • Is this patient in the time window? – 3-4.5 hours from symptom onset depending on institution (discussion to follow) – Patients who went to bed normal and awoke with deficit-disqualified from consideration – Priority-get patient quickly to CT to rule out ICH and remain within time window Acute Stroke-Initial Priorities • Rule out other causes of neurologic findings – ICH-Get head CT – Hypoglycemia-get finger stick glucose – Aortic dissection-assess for chest pain, abdominal pain occurring with the neurologic symptoms – Obtain EKG to assess rhythm Thrombolytics • Must weigh risks and benefits • Benefit: potential return of neurologic function • Risk: ICH, non CNS hemorrhage death, poor functional outcome • Essential to discuss with patient, family, and document this discussion • MUST apply current evidence and carefully apply inclusion/exclusion criteria Thrombolytics-Inclusion Criteria • Inclusion Criteria – Age 18 or over – Clinical diagnosis of acute ischemic stroke causing a measurable neurologic defect – Time of symptom onset well established to be less than 180 minutes before treatment would begin • This excludes many patients as duration is frequently longer than 3 hrs, includes time to obtain and read head CT Thrombolytics-The evidence • Controversial – study done by NINDS in 1995 • NNT=9 for increase in normal function at 3 months • Significant Intracranial Hemorrhage rate about 6% – NNH=15 – Most with worse deficits than stroke » About half of ICH fatal • Not reproduced outside of NINDS – Until ECASS 3 published in 2008 NINDS study group 1995 Thrombolytics-ECASS 3 • Prospective, randomized, double blind trial to assess safety and efficacy of thrombolysis up to 4.5 hours from symptom onset – Higher rate of favorable outcome in treatment group versus placebo (52% versus 45%) – Higher rate of ICH in treatment group (27% versus 17%) Hacke et al 2008 Thrombolytics-ECASS 3 • Thrombolytics less efficacious from 3-4.5 hours than from 0-3 hours – Odds ratio for favorable outcome • 2.80 for 0-90 minutes • Only 1.40 for 3-4.5 hours Hacke et al 2008 Thrombolytics-ECASS 3 • ICH rate reported in study higher than original NINDS trial • Bottom line: From 3-4.5 hours, modest increase in improved functional outcome. Increase in intracranial hemorrhage risk Hacke et al 2008 Case 3 • Patient’s blood sugar normal, EKG is NSR, labs drawn and patient sent for urgent head CT. • On return from head CT patients symptoms have resolved – Normal motor function bilaterally on exam • Head CT neg but defer on TPA as patients symptoms have resolved spontaneously. • What is your next step? Case 3-Diagnosis/Workup • TIA-transient ischemic attack • Patient needs Neurology consult – Evaluation for reversible cause or stroke and risk factor modification • Carotid us, MRI/MRA, Cardiac Echo – Frequently done as inpatient • TIA patients at increased risk of stroke especially in the days after a TIA • Can be done as outpatient if patients deficits have resolved and expedient workup can be arranged TIA-Short Term Outcomes • JAMA study (2000) • 1707 TIA patients • Observed for rate of stroke, recurrent TIA, cardiovascular events, death in 90 days after initial ED evaluation for diagnosis of TIA Johnston et al 2000 TIA-Short Term Outcomes • 180 (10.5%) patients returned to ED with CVA • 91 of the CVAs occurred in the first 2 days – Risk factors associated with risk of returning with CVA: • • • • • Age >60 (odds ratio: 1.8) Diabetes mellitus (OR: 2.0) Symptom duration >10 minutes (OR: 2.3) Weakness (OR: 1.9) Johnston et al 2000 Speech disturbance (OR: 1.5) TIA Short Term Outcomes • Increased risk of CVA short term following TIA • Take risk factors into consideration when making inpatient versus outpatient workup decision Case 3-Treatment • Aspirin therapy – Started on all patients with ischemic stroke or TIA • To prevent further stroke • Platelet Aggregation – Clopidogrel, ticlopidine – Used in patients intolerant to ASA – Also in patients who have CVA while on ASA Beware Stroke Mimics • Hypoglycemia • Todd’s Paralysis – Post-ictal neurologic deficits • Complex Migraines • Conversion Disorder Usually suspect given history and physical – Assume stroke if uncertain Case 4 • 22 year old female • Brought in by ambulance • Observed to have seizure like activity at home and is now sleepy and confused • On arrival, the patient is sleepy, but opens her eyes to voice, pushes away in response to pain • You note that she has urinated on herself Case 4 • VS: T: 36.3, HR 80, BP 120/80, RR 18, SpO2 100% • Finger stick blood glucose for EMS: 100 • As you continue your assessment, the patient begins having a generalized tonic clonic seizure • What’s your next step? Active Seizures-Treatment • First line-Benzodiazepines – Lorazepam IV preferred agent – Lorazepam pediatric dose 0.1 mg/kg up to max of 1-2 mg per dose – Adults: Lorazepam 1-2 mg/dose, okay to repeat every 1-3 minutes if seizures continue • Dosing ultimately limited by respiratory depression, which can be managed with intubation if necessary Active Seizures-Treatment • Supportive measures – Ensure bed rails up, seizure pads (if available) in place – Place supplemental oxygen (non rebreather) on patient – Place oral/nasal airway as necessary to maintain patent airway Active Seizures-Treatment • If no control despite multiple doses of benzos, consider alternative agents – Fosphenytoin (18-20 PE/kg) – Phenobarbital (10-20 mg/kg) – If you need to secure the patient’s airway, may need to involve neurology for EEG monitoring if the patient is paralyzed Case 4 • Seizure stops after 2 doses of lorazepam • The patient is maintaining her airway, and appears postictal • The nurse asks you, “What are you going to do to work her up?” Seizure-Evaluation • Depth of workup depends upon whether or not event is a first time seizure First Time Seizure Workup • Electrolytes • CT of the head to evaluate for SAH, mass lesion • Other tests dependent upon clinical scenario – If suspicion for CNS infection, perform LP First Time Seizure-Disposition • If no further seizure activity, returned to baseline and competent caretaker with patient: – May return home with Neurology follow up arranged – Will need outpatient MRI, EEG – No driving, no bathing/showering alone – Good dismissal instructions including reasons to return Breakthrough Seizure-Workup • Medication non compliance common-check drug levels • Evaluate for infection • Check finger stick glucose • Most patients do not require neuroimaging – Consider if long period of decreased LOC or other new focal neurologic finding Breakthrough Seizure-Disposition • May be discharged home if neurologically normal after postictal period and drug levels are within normal limits References • NINDS study group. “Tissue plasminogen activator for acute ischemic stroke”. New England Journal of Medicine. 333: 1581-1587. • Hacke W et al. “Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke”. New England Journal of Medicine. 359: 1317-1329. • Johnston SC et al. “Short-term prognosis after emergency department diagnosis of TIA”. JAMA. 284:2901-2906.