Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
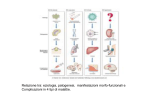
Aplastic Anemia Fanconi Anemia NPH Severe Aplastic Anemia (SAA) • Pancytopenia caused by hypoplasia of the marrow • May be congenital or acquired • Incidence: 2 new cases / million population / year • In 50% of acquired forms no cause can be found • The response to IS therapy (ATG, CSA) suggests an immune mechanism may be involved Drugs & Chemicals associated with SAA • Agents that regularly produce marrow depression as major toxicity in commonly used doses or normal exposures • Cytotoxic drugs used in cancer chemotherapy • Benzene • Agents probably associated with SAA but with a low probability relative to their use • Chloramphenicol, insecticides • Non steroidal antiinflammatory drugs • Anticonvulsants, Gold salts, sulfonamides, estrogens • Agents more rarely associated with SAA • Antibiotics (streptomycin, tetracycline, bactrim) • Antihistamines, sedatives, allopurinol, lithium Ionizing radiation • SAA has been reported after exposure io radiation due to: • Nuclear bomb explosion • Radioactive fallout • Medical or occupational exposure • SAA is observed at total body exposures between 1.0 and 2.5 Gy • LD50 is observed at 4.5 Gy • 100% mortality in the range of 10 Gy Viruses • Antecedent Acute hepatitis has been noted in 2-5% of SAA. Aplasia occurs 2 months after the acute episode • EBV, CMV, HIV • Viruses may be directly cytotoxic to bone marrow cells or alternatively, may stimulate an immune response against those cells • Infection of BM stromal cells has also been postulated to compromise the BM microenvironment Pathophysiology (I) • Quantitative stem cell defect – LTIC and CD34+ cells are reduced – 50% of matched BMT works without conditioning • Qualitative stem cell defect – increased incidence of late clonal dosorders (MDS, Acute Leukemia) • BM Stroma defect – Abnormal adipocyte proliferation – However, after BMT, most stromal cells remain of host origin and adequately support the donor’s stem cells Pathophysiology (II) • Immune suppression of hematopoiesis – AA responds to ATG, CSA treatment – Patient’s BM cells inhibit normal BM colony formation (serum??) – Lymphocyte infiltration of aplastic BM Clinical Features • Anemia • Fatigue, lack of energy, shortness of breath, angina secondary to anemia, excessive sleep • Bleeding is an alarming symptom • Gum oozing, hepistaxis, easy bruising • Heavy menstrual flow or menorrhagia • Serious Infections is unusual early in the course of disease Classification of Aplastic Anemia by counts SAA. Hemorrhages • Petechiae are usually located over dependent surfaces, oropharynx, palate. • Petechiae of the mucosa are the most common oral manifestations SAA. Hemorrhages • Retinal hemorrhages in a patients with SAA and profound thrombocytopenia (1 x 109/l) • Spontaneous mucosal hemorrhages in a 10-y old boy with Fanconi anemia (PLT <5x109/l) • Spontaneous facial ecchymoses in pt with undetectable platelets in PB SAA. Infections • Ulceration of the buccal mucosa associated with severe neutropenia (<500 x 109/l) • Raised, erythematous skin nodule from infection with candida albicans, which was also present in the bloodstream Diagnosis • • • • • Anemia (Hb<7 gr/dl, MCV 95-110 fl) Granulocyte count below 0.5 x 109/L Platelet count below 20 x 109/L Absolute reticulocyte count ≤ 40 x 109/L BM biopsy must contain <25% of the normal cellularity • BM Cytogenetics are normal • EPO levels are usually increased • Iron and ferritinemia are increased Normal bone marrow Aplastic bone marrow Bone marrow • Bone marrow biopsy shows the characteristic hypocellularity. • The few cellular elements are comprised primarly of lymphocytes Differential Diagnosis Differential Diagnosis SAA and Thymoma • SAA may appear in conjunction with thymoma • Upper mediastinal CT scan shows a thymoma as retrosternal mass of irregular outline in a 62-yr old man with myastenia and PRCA. • Section of thymoma showing spindle cells and epithelial cells Terapia • Generica: – Terapia anti-infettiva (contro batteri e funghi) – Ricovero in camera a pressione positiva • Specifica: – Se secondaria: rimozione patologia di base – Se idiopatica : dipende dall’età Algoritmo Terapeutico < 50 > 50 Tipizzazione HLA immediata Donatore HLA identico SI CSA, ATG NO Risposta HSCT +/condizionamento NO HSCT da Donatore alternativo SI Overall Survival Age > 20 N > 200 Age < 20 N < 200 Fanconi Anemia • • • • • • Autosomal recessive disease The mean age at Dx is 7 to 9 yrs 75% diagnosed between 4 and 14 yrs Similar frequencies in both genders No ethnic restriction Is genetically heterogeneous with 8 different complementation groups • 10% develop acute myeloid leukemia Anemia di Fanconi: gruppi e geni identificati Gruppo Gene identificato Frequenza (%) Localizzazione cromosomica FA-A FA-C FANCA FANCC 66 12 16q24.3 9q22.3 FA-D1 FA-D2 BRCA2 FANCD2 <1 <1 13q12-13 3p25.3 FA-E FA-F FA-G FANCE FANCF FANCG 4 4 12 6p21.3 11p15 9p13 FA-L FANCL <1 2p16 malformazioni congenite più frequenti Tipo di malformazione Pigmentazione cutanea (macchie caffè-latte, iper- e ipo-pigmentazione) Frequenza (%) 60-70 Ritardo di crescita (bassa statura) 65 Alterazioni del radio e del pollice 60-70 Anomalie apparato genito-urinario 50-57 Anomalie oculari (microftalmia) 35-45 Alterazioni gastrointestinali (atresia esofago, duodeno o ano) 10-15 Diagnosis • The underlying problem seems to be defective DNA repair • Cells from FA have an high frequency of spontaneous chromosomal breakage • Increased chromosomal fragility is enhanced in the presence of DNA clastogenic agents : – Mitomycin C (MMC) – Diepoxybutane (DEB) Emoglobinuria Parossistica Notturna. EPN • Anemia emolitica acquisita da difetto intrinseco – Coesistono GR monoclonali patologici e GR policlonali normali • Rara (1/100.000 abitanti), colipsce adulti (40 a) • Clinicamente caratterizzata da: – Emolisi cronica con tipiche crisi notturne di emoglobinuria macroscopica – Tendenza alla trombosi venosa – Associazione con aplasia midollare severa • Patogenesi: – Malattia della cellula staminale determinata dalla mutazione del gene PIG-A coinvolto nella sintesi del legame fosfatidil-inositolo, attraverso il quale proteine di superficie si ancorano alla membrana eritrocitaria. Complement regulatory proteins on normal erythrocytes GPI-anchored proteins Transmembrane protein DAF MIRL CR1 Membrane Lipid Bilayer CR1: complement receptor 1 (CD35) DAF: decay accelerating factor (CD55) MIRL: membrane inhibitor of reactive lysis (CD59) GPI: glycosylphosphatidylinositol Ethanolamine Glucosamine Mannose 20% to 50% dei pazienti con SAA hanno il fenotipo della EPN al citofluorimetro DAF: decay-activating factor (CD55) MIRL: membrane inhibitor reactive lysis (CD59)