Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
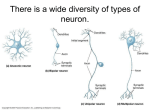
Motor neuron disease Multiple sclerosis Motor neuron disease Motor neuron disease is degenerative disease which selectively affect motor tract fibers (corticospinal tract+ anterior horn cell) UMN signs LMN signs Motor pathway cortex motor area Corticospinal fiber & corticobulber AHC Peripheral nerves NMJ muscle motor neuron disease pathology Degeneration of the neurons path physiology Sporadic:90% unclear Inherted:10% familial ALS,25% mutation in gene encoding copper zinc super oxide dismutase (SOD1) course Is progressive : median survival is approximately 3y classification Classic ALS (amyotrophic lateral sclerosis)..UMN+LMN signs others Progressive muscular atrophy Primary lateral sclerosis Progressive bulbar palsy Progressive pseudo bulbar palsy Classic ALS Mixed upper motor neuron + upper motor neuron signs Early patient may exhibit only LMN signs or upper LMN signs Weakness begin a symmetrical and distally then spread to involve contiguous group of motor neurons Bulbar &pesudobulber palsy involvement ..dysphagea & dysarthria Nooooooooooo Cognitive Sensory Ocular Autonomic Sphincter dysfunction diagnosis El Escorial criteria for dx Definitive Probable possible Electrophysiological NCS: sensory..N motor:normal or decreased amplitude EMG: denervation treatment Riluzole :50 mg bid ( extend tracheotomy free survival by 2-3 months, not improving the survival or muscle strength Supportive care physiotherapy, respiratory, swallowing….. Multiple sclerosis MS is the most disabling neurological condition of young adults Epidemiology Onset is typically in the mid 20s,although the dx may be delayed for several years The ratio of f to m 1.77 to 1 The incidence of MS in blacks residing in the united states is about 25% that of whites High incidence includes all of Europe,North america,New Zealand,southern austeralia but the incidence also increasing in middle east pathophysiogy Inflamatory rxn causes variable tissue damage Destruction of myelin producing cells (oligodendrocytes) Some cells damaged without remyelination but oligodendrocytes precursors ..remyelinate..plaque Risk factors Genetic Infection :viral autoimmune genetic In general in the united states, the prevalence of MS is about ,1% If a mother has MS,, her children's have a chance 3-5% . If father has MS, his son has a1% chance & his daughter a 2% chance Non identical twins has 3-4% Identical twins:30% Clinical presentation Relapsing remitting: the commonest (>one attack in >one site (multifocal) Progressive relapsing Primary progressive Secondary progressive diagnosis Clinical :typical relapses come on over a few days, lasts for weeks or months ,and then clear, over 80% of patients begin with relapses All central nervous system can be affected Typical relapses A-optic neuritis B-myelopathy(spinal cord) C-brain stem &cerebellar Optic neuritis: clouding or blurring of central vision in one eye loss of measured activity, impair pupillary light reflex, some local pain made worse by eye movement…usually full recovery Myelopathy: often sensory only; numbness &tingling from a certain level on the trunk on down through the rest of the body. if marked ..weakness Brain stem Each of these relapses may leave some residual After several attacks of various types, a patient may present common deficit Mild reduction in vision in one eye No conjugate eye movements Extensor planter responses &inability to walk heel and toe Reduced vibration sense in the legs Urgency of bladder function Late stage deficit include: dementia, inability to stand or walk, slurred speech, ataxic, incontinence ,and marked sensory loss in hands &legs Lehrmit sign Athoufs phenomena Diagnostic workup MRI Mri is now the dominant laboratory method of diagnosis in MS MS lesions are usually easily detected and often characteristic… Multiple bright lesion in T2 Contrast enhanced lesion Shape :ovoid Size:>5mm Site: adjacent to the lateral ventricles, corpus callosum, cerebellum LP: modest no of lymphocytes <50/mm,total protein <.8g/L,elevated immunoglobulin G(IgG), level oligoclonal banding on electrophoresis(80%) Evoked potentials: VER,BAR,somatosensory evoked potential diagnosis McDonald criteria: Confirm lesion >one site +> one attack Diffrential diagnosis Clinically: Multiple infarctions Autoimmune diseases Vascuilities: behcets Sarcidosis Infection: chronic meningitis Diseases that cause similar MRI pictures Vascular: vascuilities,small vesseles disease,migraine Infection:HIV.Lyme disease Granulomtous :sarcidosis ADEM Treatment: Definitive supportive definitive Six principles of management in multiple sclerosis 1-relapses with significant impairment of function should be treated with high dose IV corticosteroid 2-All relapsing remitting patients should be receiving long term immunomodulatory treatments 3-Secondary progressive need aggressive tt early,late treatment <few years little benefit 4- primary progressive patients can not be expected to response to any treatment 5-multiple sclerosis is a life long disease ,no specific time when to discontinue treatment once it started, if one modality of treatment fail or not tolerated ,another medication should be tried 6-patients need to be watched for signs of disease activity by clinical or magnetic resonance monitoring or both. Drug for acute phase Methylpredinsolone 1g iv for 5d Side effects: Drug used for long term management Interferon –B(avonex,betaseron,rebif.. decrease the risk of the attacks by 30%(sc.IM) Side effects: Depression, flu like, hepatitis Copaxon: Widespread articaria Supportive care symptomatic Spasticity Depression Fatigue Urinary urgency pain