Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
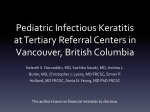
Recrudescent Acanthamoeba Keratitis Related to Persistent Contact Lens Wear Elmer Y Tu1A, Charlotte E Joslin1, Megan E Shoff2, Janet A. Lee1, Ali Djalilian1 1Department of Ophthalmology and Visual Sciences University of Illinois Eye and Ear Infirmary Chicago, Illinois 2Department of Molecular Genetics The Ohio State University Columbus, Ohio 1A Allergan – travel honoraria No conflicts of interest pertaining to this presentation. Off-label use will be discussed Purpose: To report patients with a second diagnosis of Acanthamoeba keratitis after continuing contact lens wear Methods: Acanthamoeba keratitis patients diagnosed between 06/2003 – 09/2007 University of Illinois Eye and Ear Infirmary Cases reviewed for involvement of multiple eyes Results 88 total patients identified with Acanthamoeba keratitis 9 patients diagnosed with multiple infections 7 presenting with bilateral disease 1 patient had the contralateral eye involved 3 months later 1 patient presented with re-involvement of the same eye 17 months later Case 1 Resolved scar 17 year old white male presented 6/1/07 with a severe, painful recurrent keratitis OS Failed treatment topical antibiotics, antivirals and corticosteroid Confocal microscopy c/w Acanthamoeba Cultures negative Resolution over three months with propamidine and chlorhexidine with small residual scar (figure above) Patient continued contact lens wear OD, despite warnings to discontinue Stroma Case 1 Acanthamoeba Cysts Epithelium Patient presented with necrotic ulcer OD 9/7/07 Partially treated ulcer was culture negative Fortified cefazolin and gentamicin Good response clinically and symptomatically 9/18/2007 Reports increasing discomfort and forms an immune ring (figure below) Confocal positive (see above) Partial immune ring Case 2 Bright-centered Acanthamoeba cysts 16 year old African-American male 2/13/06 SCL wearer treated for 2 weeks with Viroptic and Acyclovir Referred for keratitis with radial neuritis OD Confocal/ Diff-Quick Smear/ Culture positive 20/20 vision after 3 months of therapy Propamidine and chlorhexidine Patient resumed contact lens wear 3 months later Sports scholarship to college Case 2 Presented 7/26/07 with pain and decreased vision (20/40) OD x 2 weeks SCL wear/ AMO Complete Moisture Plus Swimming in lenses 3 weeks prior in another state where he was in school for the past 9 months Confocal/ Diff-Quick Smear/ Culture positive Genotype distinct from first isolate Diff-Quik Stain (Original magnifiction 100x oil) Genotyping results Sequence comparison of the two isolates obtained from Case 2 for a 135 nucleotide base region within one of the highly informative diagnostic fragments of the Acanthamoeba 18S rRNA gene. The two isolates, 06005 and 07-072, clearly differ from each other, with 13/135 base differences. However, as shown, each isolate separately closely resembles different previously reported Acanthamoeba sequences found in the DNA database GenBank. Discussion A common question from patients successfully treated for Acanthamoeba keratitis (AK) is the safety of subsequent contact lens wear. Since AK is a rare disease estimated to affect approximately 2-20 wearers per million contact lens wearers per year, by chance alone, the likelihood of a second infection is remote. The understanding of the risk factors and mechanisms for the development of AK remain, however, incomplete. While the sequential nature of bilateral AK has been previously described, as seen in case 1, it does not distinguish the roles of environment and individual susceptibility since these patients usually have little change in their environment during the short time between occurrences. Re-occurrence in the same eye 17 months apart, as illustrated in Case 2, may still represent either a reactivation of the original infection or a second, new infection. The interval lack of symptoms and signs of infection and the identification of two genetically distinct pathogenic Acanthamoeba isolates make it strongly likely that patient 2 contracted a new infection after persisting with soft contact lens wear. Discussion While uncommonly highlighted, bilateral, contemporaneous disease may occur in up to 8-10% of patients and is congruent with our own experience during the Chicago Acanthamoeba outbreak. Whether this is more common to environmentally sourced outbreaks is unclear. The odds of contracting two separate infections without significantly common risk factors are prohibitively unlikely, but in bilateral disease could be attributed to a common exposure, or load, of organisms either in the environment, as we have previously hypothesized, or overgrowth within an individual’s contact lens care system. It is also unknown whether individual patients may be uniquely susceptible to Acanthamoeba keratitis. Case 2 indicates that, despite its rare incidence, an individual can contract a separate rare infection in a different environment while attending college 900 miles away. Although hygiene factors may play a role, the relative permissiveness of ocular defense mechanisms including local and systemic immune defenses may also contribute. Conclusion These cases indicate an ongoing risk for the development of Acanthamoeba keratitis in patients previously infected. Acanthamoeba keratitis may require not only the presence of organisms, but also some measure of individual susceptibility. The understanding of the mechanisms and risk factors for human corneal infection with Acanthamoeba remains incomplete and deserves further study. Selected References Acknowledgments Joslin CE, Tu EY, Shoff ME, et al. The Association of Contact Lens Solution Use and Acanthamoeba Keratitis. Am J Ophthalmol 2007. Joslin CE, Tu EY, McMahon TT, Passaro DJ, Stayner LT, Sugar J. Epidemiological characteristics of a Chicago-area Acanthamoeba keratitis outbreak. Am J Ophthalmol 2006;142:212-7. Wilhelmus KR, Jones DB, Matoba AY, Hamill MB, Pflugfelder SC, Weikert MP. Bilateral acanthamoeba keratitis. Am J Ophthalmol 2008;145:193-197. Bernauer W, Duguid GI, Dart JK. [Early clinical diagnosis of acanthamoeba keratitis. A study of 70 eyes]. Klin Monatsbl Augenheilkd 1996;208:282-4. Ficker L, Seal D, Warhurst D, Wright P. Acanthamoeba keratitis--resistance to medical therapy. Eye 1990;4 ( Pt 6):835-8. Johnson AM, Fielke R, Christy PE, Robinson B, Baverstock PR. Small subunit ribosomal RNA evolution in the genus Acanthamoeba. J Gen Microbiol 1990;136:1689-98. University of Illinois Eye and Ear Infirmary Joel Sugar, MD Leslie T. Stayner, PhD Jamie Brahmbhatt, COMT The Ohio State University, Dept. Molecular Genetics Gregory C. Booton, PhD Paul A. Fuerst, PhD Support: Prevent Blindness America Midwest Eye-Banks NIH/NEI K23 15689 UIC Campus Research Board Gerhard Cless Foundation