Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
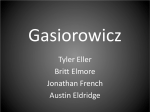
PERIODONTAL EFFECTS OF THE MAGNETAINER™ COMPARED TO FIXED RETENTION Don H. Dau, D.M.D. A Thesis Presented to the Graduate Faculty of Saint Louis University in Partial Fulfillment of the Requirements for the Degree of Master of Science in Dentistry 2015 © Copyright by Don Hoang Dau ALL RIGHTS RESERVED 2015 i COMMITTEE IN CHARGE OF CANDIDACY: Associate Clinical Professor, Donald R. Oliver, Chairperson and Advisor Associate Professor Ki Beom Kim Professor Douglas Miley ii I dedicate this work to my parents, my brother, and my sister. They have supported me throughout my life, and without them, I would not be where I am today. iii ACKNOWLEDGEMENTS This project would not have been possible without the mentorship of Drs. Donald Oliver, Ki Beom Kim, and Douglas Miley. Thank you for your support and guidance. Thank you to Drs. Gene and Aron Dellinger for your assistance with the sample for the MagneTainer™ group. Thank you to Dr. Randall Brown for your assistance with the sample for the bonded lingual retainer group. Thank you to Dr. Heidi Israel for your assistance with the statistical analysis. iv TABLE OF CONTENTS List of Tables......................................vii List of Figures....................................viii CHAPTER 1: INTRODUCTION..............................1 CHAPTER 2: REVIEW OF THE LITERATURE Stability and Relapse............................4 Removable Retention..............................6 Hawley Retainers............................6 Vacuum-Formed Retainers.....................7 Patient Compliance..........................8 Fixed Retention..................................9 Periodontal Implications of Fixed Retainers.....10 Magnets.........................................13 Magnet Properties and Types................13 Biological Considerations..................15 Corrosion Products.........................15 Magnetic Fields............................17 Statement of Thesis.............................19 Literature Cited................................20 CHAPTER 3: Journal Article Abstract........................................26 Introduction....................................28 Materials and Methods...........................32 Error Study.....................................35 v Statistical Analysis............................35 Results.........................................36 Discussion......................................39 Conclusion......................................41 Literature Cited................................42 Appendix.............................................47 Vita Auctoris........................................48 vi LIST OF TABLES Table 2.1 Criteria for the Gingival Index System.......11 Table 2.2 Criteria for the Plaque Index System.........12 Table 3.1 Criteria for the Gingival Index System.......34 Table 3.2 Criteria for the Plaque Index System.........34 Table 3.3 Mean, standard deviation, and standard of error for the GI score, PI score, Calculus score, brushing frequency, and flossing frequency....................................36 Table 3.4 Mann-Whitney U test for significant differences between the variables............37 Table 3.5 Frequency of brushing difficulty for both groups.......................................37 Table 3.6 Mann-Whitney U test to camper difficulty of flossing with GI score, PI score, Calculus score, brushing frequency, and flossing frequency....................................38 Table 3.7 Spearman’s correlation for GI score, PI score, Calculus score, brushing frequency, and flossing frequency.......................38 Table 3.8 Independent t-tests for significant differences in probing depths................39 vii LIST OF FIGURES Figure 1.1 The MagneTainer™ in place on a patient......3 Figure A1 Questionnaire Given to Patients............47 viii CHAPTER 1: INTRODUCTION Orthodontic supervision does not end once the appliances have been removed. Orthodontists and patients alike are concerned about the anticipated degree of stability following active orthodontic treatment, and it has been suggested that lifetime retention is necessary to maintain satisfactory alignment after treatment in many patients.1 As part of routine orthodontic protocol, a retention period after treatment is done with removable retainers, fixed retainers, or a combination of both. Perfect alignment after orthodontic treatment is unrealistic over a lifetime, and literature has shown that relapse following orthodontic treatment is both unpredictable and unavoidable.1-5 The challenge that many orthodontists find in retention is that it is impossible to predict which cases will undergo relapse and to what degree it will occur.6 The words relapse, physiologic recovery, rebound, post-retention settling, and other similar terms have been used by orthodontic practitioners to describe the changes that occur after orthodontic appliances have been removed.7 Relapse can occur anywhere in the dentition, but one of the more evident areas of potential instability is the 1 lower anterior region. Fixed retention was introduced to help improve post-treatment stability of the lower anterior teeth. Fixed retention in this area involves a wire that transverses the lingual surfaces of mandibular anterior teeth. While the main advantages of fixed lingual retention are the esthetic value and virtually compliance free nature, one of the major disadvantages is the tendency for plaque and calculus accumulation over time.8 As a result, there may be a negative effect on the periodontal health.9 The MagneTainer™ is being introduced as an alternative to traditional fixed lingual retention. The MagneTainer™ was developed by Drs. Gene and Aron Dellinger of Ft. Wayne, Indiana. It utilizes neodymium-iron-boron magnets that are bonded on all the marginal ridges from the mesial of the lower canine to the mesial of the contralateral canine as seen in Figure 1.1. The magnets maintain the alignment of the lower anterior teeth and allow patients to floss straight down the contact without any additional flossing auxiliaries. With the trend of using fixed lingual retainers for long-term retention, it is important to understand the effects that they may have on the periodontal tissues. The purpose of this study is to compare the periodontal health 2 of the mandibular anterior teeth retained with the MagneTainer™ versus a conventional fixed lingual retainer. Figure 1.1: The MagneTainer™ in place on a patient 3 CHAPTER 2: REVIEW OF THE LITERATURE Stability and Relapse The orthodontic literature has shown that relapse following orthodontic treatment is both unpredictable and unavoidable.1-5 The challenge that many orthodontists find in retention is that it is impossible to predict which cases will undergo relapse and to what degree it will occur.6 The words relapse, physiologic recovery, rebound, post-retention settling, and other similar terms have been used by orthodontic practitioners to describe the changes that occur after orthodontic appliances have been removed.7 Longitudinal studies have shown that during the posttreatment period, there is a trend towards decreased arch length, decreased arch width, increased overbite, increased overjet, and increased mandibular anterior crowding.4, 7, 10-12 Horowitz and Hixon stated that orthodontics may alter the course of the continuous physiologic changes, however, following the mechanotherapy and retention period restraint, the developmental maturation process resumes.13 In order to understand post-retention stability and relapse, it is important to examine the maturation of untreated normal occlusions. Sinclair and Little examined untreated cases from the mixed-dentition phase to early 4 adulthood and found a decrease in arch length, a small decrease in inter-canine width, minimal change in intermolar width, minimal change in overjet and overbite, and an increase in incisor irregularity.7 Changes that occur in the untreated dentition are less than that seen in treated cases post-retention.7 Eslambolchi et al. examined longitudinal changes in mandibular incisor alignment in treated and untreated patients. They found that treated and untreated patients had similar long-term changes. Intercanine width, interfirst premolar width, arch length, anterior space, and total space significantly decreased while Little’s irregularity index significantly increased in both groups.14 Blake and Bibby examined 15 potential factors of stability that included arch form, periodontal tissues, mandibular incisor dimensions, neuromusculature balance, growth, post-treatment results, third molars, original malocclusion, extraction treatment, expansion, and nonextraction treatment.15 They concluded that orthodontist should aim to remove the primary burden of preventing relapse from the patient by maintaining treatment goals that follow well-documented principles such as maintaining lower intercanine width and lower arch form.15 5 Even though there are many studies describing possible pretreatment factors leading to relapse, most attempts have been unsuccessful at showing any reliable predictors of stability.16-18 Ormiston et al. found that the initial severity of the malocclusion was correlated with the postretention instability.18 Despite orthodontists’ best efforts, the best way to maintain satisfactory alignment post-treatment is through an indefinite period of retention.1 One of the more unstable and unpredictable areas during the retention period is the lower anterior region.1921 According to Zachrisson, long-term retention of the lower anterior segment may be necessary in order to prevent or reduce unwanted post-treatment changes.22 Removable Retention The two main forms of removable retention utilized by orthodontists are Hawley retainers and vacuum formed retainers. Each of these has their own respective advantages and disadvantages; however, one commonality between the two is that they rely heavily on patient compliance. Hawley Retainers Charles Hawley designed the Hawley retainer in 1919. Hawley designs have evolved throughout the years, but the 6 current basic design includes a labial bow that contacts the anterior teeth and an acrylic plate that rests behind the teeth. Hawley retainers are known for their durability and adjustability during the retention period. They allow for relative vertical movement of the posterior teeth during retention, and this allows for post-treatment settling of the dentition.23 When compared to wearing vacuum-formed retainers, the use of Hawley retainers results in more occlusal contacts because the retainer does not involve occlusal coverage.23 Vacuum-Formed Retainers Vacuum-formed retainers were introduced in 1971.24 Their popularity has grown due to their esthetic qualities, ease of fabrication, and lower costs.6, 21, 25 The drawbacks of vacuum-formed retainers include occlusal wear of the appliance, cracking, reduced vertical settling, and adjustability of the appliance.6, 23 Various studies have shown that vacuum-formed retainers are effective as Hawley retainers in maintaining orthodontic corrections.6, 21, 26 Barlin et al. examined eighty-two patients who were randomly assigned either a Hawley or a vacuum-formed retainer.6 After a 12-month period, there was no difference in the measured arch width, arch length, or modified Little’s index.6 7 Two studies have shown, however, that vacuum-formed retainers are more effective in maintaining mandibular incisor positions during retention when compared with Hawley retainers.21, 27 Despite the statistically significant results of these studies, they can be considered clinically insignificant unless it relates to a single tooth displacement in the mandibular arch.21 Patient Compliance The retention phase is placed in the hands of the patient once they are given a retainer.28 The desire to keep the teeth aligned after years of orthodontic treatment now depends on the patient. Every orthodontist has a different retention protocol, but the end goal is the same. A survey of two thousands orthodontists was conducted and it was found that most orthodontists prescribed less than 9 months of full-time wear and advised life-long part-time wear.28 Despite that which is prescribed and how much emphasis is placed on the need for retention, patient behavior can vary. A survey of 428 retention patients showed that 20% of patients were not wearing their retainers after 2 years, but 45% were wearing them every night and 80% at least 1 night per week.29 They did not find age or sex to influence the levels of compliance.29 8 Fixed Retention Fixed lingual retainers are the main alternatives to traditional removable retainers, especially in the lower anterior region. Traditionally, bonded mandibular canineto-canine retainers are made from single stranded or multistranded wires bonded to the lingual surfaces of the lower anterior teeth. Their popularity has grown because they are esthetically pleasing, virtually free of patient compliance, and reliable as part of the retention phase. The major shortcomings include the time consuming placement procedure, bond failures, stress fractures, and the tendency for plaque and calculus accumulation.30 One of the main advantages of fixed lingual retainers is that they are reliable in maintaining post-retention stability due to their almost compliance free nature. Artun and coworkers found that fixed lower retainers effectively maintained incisor alignment 3 years posttreatment and these results have been supported by other studies as well.30-32 The effectiveness of fixed lingual retainers at maintaining alignment is only possible as long as the retainer is intact and does not have bond failures.30, 32, 33 When failures occur, more incisor irregularity is observed when compared to the retainers that did not fail.30, 32, 33 9 Failures can be intrinsic because of poor bonding technique, or they can be extrinsic due to wear or direct trauma to the retainer.32 Bond failure rates as reported in the literature range from 9% - 35%.30, 32, 33 Variation in bond failure rates reported can be attributed to how bond failures are recorded, whether a dentist fixed a bond failure during a hygiene check, and the length of the observation period. Since patients with retainer failures experienced more relapse than those without failures, it is important to minimize bond failures in order to maintain the effectiveness of lower lingual bonded retainers.30, 32 Lingual fixed retention may be compliance free in regards to wearing a retainer, however, it is not compliance free when it comes to care in food type selection and oral hygiene. Since the wire of a fixed lower retainer transverses the lingual surfaces of the mandibular anterior teeth, flossing and brushing can be more difficult. The result is a tendency for plaque and calculus buildup around the area of the retainer. Periodontal Implications of Fixed Retainers The Gingival Index system was introduced in 1963 and the Plaque Index system was introduced in 1964.34, 35 The Gingival Index system is used as a method to assess the gingival condition through qualitative changes in the 10 gingival soft tissue.36 Each tooth is broken down into four areas that make up the circumference of the marginal gingiva (buccal, mesial, distal, lingual).36 Each of the four gingival areas is assigned a score from 0-3 based on the criteria for the Gingival Index system as seen in Table 2.1. The average of the scores of the four areas of a tooth gives the GI for the tooth. The average of all the GI’s of the individual teeth examined gives the GI for the individual. Silness and Loe’s Plaque Index system is similar to their Gingival Index system in that it is used to clearly distinguish between the severity and location of soft debris aggregate.35 The individual locations, individual teeth, and overall individual scores are calculated similar to that of the Gingival Index system. The criteria for the Plaque Index system can be seen in Table 2.2. Table 2.1: Criteria for the Gingival Index System adapted from Loe and Silness34 Criteria for the Gingival Index System Score 0 Description Normal gingiva 1 Mild inflammation – slight change in color, slight edema. No bleeding on probing 2 Moderate inflammation – redness, edema and glazing. Bleeding on probing 3 Severe inflammation – marked redness and edema, ulceration. Tendency to spontaneous bleeding 11 Table 2.2: Criteria for the Plaque Index System adapted from Silness and Loe35 Criteria for the Plaque Index System Score Description 0 No plaque in gingival area 1 A film margin plaque across 2 Moderate accumulation of soft deposits within the gingival pocket, on the gingival margin, and/or adjacent tooth surface, which can be seen by the naked eye. 3 Abundance of soft matter within the gingival pocket and/or on the gingival margin and adjacent tooth surface of plaque adhering to the free gingival and adjacent area of the tooth. The may only be recognized by running a probe the tooth surface Loe and Silness’s Gingival Index and Plaque Index systems have been used throughout orthodontic literature to evaluate the quality of the gingiva. Artun et al. compared lower lingual fixed retainers and removable retainers utilizing the Gingival Index and Plaque Index.30 At threeyear follow-up, they found no differences in the indices and that plaque accumulation scored less frequently after 3 years in retention.30 Similarly another study found that the Gingival Index scores demonstrated no detrimental effects to the mandibular anterior gingiva after a 20-year follow-up study.37 Heier and colleagues found that there was slightly more plaque and calculus present in the fixed retention group, however, this did not result in more pronounced gingival inflammation than in the removable retainer group.38 12 In contrast, Pandis and his coworkers reported greater calculus accumulation, greater marginal recession, and increased probing depths in patients with mandibular fixed retention for long periods.39 Similarly, Levin et al. found greater probing depths, bleeding on probing, and plaque index in patients with fixed retention when compared to patients without fixed retention.9 Other researchers also found more plaque accumulation in those with bonded lingual retainers compared to removable retainers.40 Magnets Magnets are able to produce a measured force continuously over a long period of time.41 Since magnets can be made to attract or repel, they can be utilized to exert their force without the need for direct contact.41 Orthodontists have utilized magnets in a variety of ways that includes treatment of unerupted teeth, tooth movement along archwires, expansion, correction of anterior open bites, and functional appliances.41 With the introduction of utilizing magnets for retention, it is important to examine the potential biological effects that they may have when used intraorally. Magnet Properties and Types Magnets have magnetic fields around them that start from one pole of the magnet and returns to the other pole 13 of the magnet.41 They produce flux, which is the change induced by the magnet in the medium surrounding the magnet.41 The flux produced causes magnets to attract or repel other magnets and other materials containing iron.41 High-energy magnets were introduced in the 1970’s and have the advantage of being able to produce high forces relative to their size.41, 42 The increased magnetism is attributed to the property of magnetocrystaline anisotropy, which allows for single crystals to be preferentially aligned along the long C-axis.41 Rare earth metals have been incorporated into high-energy magnets and this has significantly increased the magnetism.41, 42 Rare earth magnets have high coercivity, which means that they can resist demagnetization better.41, 43 The downsides to the rare earth magnets include being brittle, having low corrosion resistance, and suffering irreversible magnetic loss when heated.41, 43 The two main rare earth magnets that have been utilized in orthodontics are samarium-cobalt magnets and neodymium-iron-boron magnets.44 Samarium-cobalt magnets are characterized by their high saturation magnetism and high Curie temperature of 680°C.42, 44 A higher Curie temperature indicates that the magnet can withstand high heat without demagnetization, 14 which is important when fabricating appliances in acrylic.42 They are more costly than other rare earth magnets.44 Neodymium-iron-boron magnets have very high magnetic saturation, good resistance to demagnetization, and the highest value of energy production.44 They are cheaper and less brittle than samarium-cobalt magnets, but they also have a lower Curie temperature at around 300°C.42, 44 Biological Considerations Any new material used clinically should not produce any side effects at a local or systemic level, and it is important to have biological safety testing done to ensure this as far as reasonably possible.45 Various studies have been done to test the biological safety of magnets by examining the effects of corrosion products and magnetic fields produced by the magnets.46-48 Corrosion Products Rare earth magnets are susceptible to corrosion and tarnish intraorally over time and the corrosion products can effect intraoral tissues.45-47 Corrosion is an electromechanical process that results in a deterioration of the metal and release of ions.45 Non-encapsulated neodymium-iron-boron magnets have poor corrosion resistance intraorally.49 Hopp et al. examined the effects of rare earth magnets on mouse fibroblasts and found that uncoated 15 samarium-cobalt magnets have a strong tendency for corrosion and exert a considerable cytotoxicity.50 They also found that uncoated neodymium-iron-boron magnets have a lesser tendency for corrosion and are only moderate cytotoxic.50 Uncoated samarium-cobalt magnets have demonstrated high to moderate cytotoxicity, while uncoated neodymium-iron-boron showed negligible cytotoxicity.48 Evans and McDonald examined the effects of the corrosion products of uncoated neodymium-iron-boron magnets on the proliferation of human oral mucosal fibroblasts and found that oral fibroblast attachment was not affected by corrosion products.45 They did note that fibroblast proliferation in the presence of corrosion products was lower than the control but not completely inhibited.45 To prevent the corrosion of magnets intraorally, it has been recommended that magnets be coated or hermetically sealed to isolate them from the oral environment.48, 50, 51 Corrosion resistance of samarium-cobalt and neodymium-ironboron magnets can be enhanced when rare earth magnets are hermetically sealed for use in dentistry.47 Noar et al. found that a thin parylene coating is unlikely to withstand intrao-oral forces, however, the shape of the magnets, the manufacturing process in production, and the thickness of the coating are important factors to consider with 16 intraoral magnets.52 Parylene coated samarium-cobalt and neodymium-iron-boron magnets have shown negligible cytotoxicity.48 Magnetic Fields The effectiveness of magnets used intraorally relies on the mechanical forces generated by magnetic fields.53 A variety of in vitro, animal, and in vivo studies have been done to see the potential effects magnetic fields may have on intraoral tissues. Linder-Aronson and Lindskog exposed cultured human periodontal fibroblasts in a static magnetic field for five weeks and found significantly and progressively impaired attachment and growth.53 They concluded that a static magnetic field itself is capable of influencing vital cell functions but did not rule out the possibility of corrosion products contributing to the cytotoxic and biological effects.53 Conversely, Bondemark et al. found short-term exposure to a static magnetic field in vitro did not cause any cytotoxic effect on the cells.48 Researchers examining human cultured cells and found that static magnetic fields had no effect on cell morphology, cell growth, DNA content, or DNA synthesis.54 17 Animal studies have shown negligible effects of magnetic fields on surrounding tissue.55-57 When magnetic appliances were placed in dogs for six months, no evidence of tissue damage was observed clinically and microscopically.57 Linder-Aronson and Lindskog examined tissue response of magnets placed in monkeys for space closure and found a lack of tissue effects of the magnets in respect to cell and tissue reactions.55 They concluded that there were negligible clinical side effects of orthodontic magnets.55 Szabo et al. examined tissue reactions of cobaltsamarium magnets by implanting them into the skulls of dogs and pigs.56 Upon histological examination, they found magnetic fields did not give rise to any tissue changes.56 There have been few in vivo studies done on the effects of magnetic fields. When human dental pulps and gingival tissues were examined after exposure to static magnetic fields in seven individuals, no change was observed in the dental pulps or gingival tissues adjacent to the magnets.58 Saygili et al. examined the effects of magnetic fields on neighboring capillary circulation in 10 subjects and found that there was no effect on blood flow when dental magnets were used.59 18 The evidence currently available from biological safety testing suggests that the conceivable risks of biological harm are neglible.41, 44 Statement of Thesis This study is a prospective study to determine whether patients with a MagneTainer™ have better periodontal health when compared to patients bonded with traditional fixed lingual retainers on the lower anterior teeth. were gathered for this study. Two samples The first sample contained 32 patients that have the MagneTainer™ in place. The second sample contained 33 patients with bonded canine-tocanine fixed lingual retainers. Periodontal health was evaluated on all patients using a gingival index, plaque index, calculus index, and probing depths. All patients were given a questionnaire relating to their oral hygiene habits. The dependent variable was the periodontal health of the patients. The alternate hypothesis is that there will be a difference in periodontal health in the MagneTainer™ group when compared to the conventional bonded lingual retainer group. The null hypothesis is that there will be no difference between these two groups. 19 Literature Cited 1. Little RM, Riedel RA, Artun J. An evaluation of changes in mandibular anterior alignment from 10 to 20 years postretention. Am J Orthod Dentofacial Orthop. 1988;93(5):423-8. 2. Little RM, Wallen TR, Riedel RA. Stability and relapse of mandibular anterior alignment-first premolar extraction cases treated by traditional edgewise orthodontics. Am J Orthod. 1981;80(4):349-65. 3. Little RM, Riedel RA, Engst ED. Serial extraction of first premolars--postretention evaluation of stability and relapse. Angle Orthod. 1990;60(4):255-62. 4. Little RM, Riedel RA, Stein A. Mandibular arch length increase during the mixed dentition: postretention evaluation of stability and relapse. Am J Orthod Dentofacial Orthop. 1990;97(5):393-404. 5. Sadowsky C, Sakols EI. Long-term assessment of orthodontic relapse. Am J Orthod. 1982;82(6):456-63. 6. Barlin S, Smith R, Reed R, Sandy J, Ireland AJ. A retrospective randomized double-blind comparison study of the effectiveness of Hawley vs vacuum-formed retainers. Angle Orthod. 2011;81(3):404-9. 7. Sinclair PM, Little RM. Maturation of untreated normal occlusions. Am J Orthod. 1983;83(2):114-23. 8. Artun J. Caries and periodontal reactions associated with long-term use of different types of bonded lingual retainers. Am J Orthod. 1984;86(2):112-8. 9. Levin L, Samorodnitzky-Naveh GR, Machtei EE. The association of orthodontic treatment and fixed retainers with gingival health. J Periodontol. 2008;79(11):2087-92. 10. Shapiro PA. Mandibular dental arch form and dimension. Treatment and postretention changes. Am J Orthod. 1974;66(1):58-70. 11. Johnson KC. Cases six years postretention. Angle Orthod. 1977;47(3):210-21. 20 12. Gardner SD, Chaconas SJ. Posttreatment and postretention changes following orthodontic therapy. Angle Orthod. 1976;46(2):151-61. 13. Horowitz SL, Hixon EH. Physiologic recovery following orthodontic treatment. Am J Orthod. 1969;55(1):1-4. 14. Eslambolchi S, Woodside DG, Rossouw PE. A descriptive study of mandibular incisor alignment in untreated subjects. Am J Orthod Dentofacial Orthop. 2008;133(3):343-53. 15. Blake M, Bibby K. Retention and stability: a review of the literature. Am J Orthod Dentofacial Orthop. 1998;114(3):299-306. 16. Shields TE, Little RM, Chapko MK. Stability and relapse of mandibular anterior alignment: a cephalometric appraisal of first-premolar-extraction cases treated by traditional edgewise orthodontics. Am J Orthod. 1985;87(1):27-38. 17. Fidler BC, Artun J, Joondeph DR, Little RM. Long-term stability of Angle Class II, division 1 malocclusions with successful occlusal results at end of active treatment. Am J Orthod Dentofacial Orthop. 1995;107(3):276-85. 18. Ormiston JP, Huang GJ, Little RM, Decker JD, Seuk GD. Retrospective analysis of long-term stable and unstable orthodontic treatment outcomes. Am J Orthod Dentofacial Orthop. 2005;128(5):568-74; quiz 669. 19. Kaplan H. The logic of modern retention procedures. Am J Orthod Dentofacial Orthop. 1988;93(4):325-40. 20. Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Syst Rev. 2006(1):Cd002283. 21. Rowland H, Hichens L, Williams A, Hills D, Killingback N, Ewings P, et al. The effectiveness of Hawley and vacuum-formed retainers: a single-center randomized controlled trial. Am J Orthod Dentofacial Orthop. 2007;132(6):730-7. 21 22. Zachrisson BU. Important aspects of long-term stability. J Clin Orthod. 1997;31(9):562-83. 23. Sauget E, Covell DA, Jr., Boero RP, Lieber WS. Comparison of occlusal contacts with use of Hawley and clear overlay retainers. Angle Orthod. 1997;67(3):22330. 24. Ponitz RJ. Invisible retainers. Am J Orthod. 1971;59(3):266-72. 25. Mai W, He J, Meng H, Jiang Y, Huang C, Li M, et al. Comparison of vacuum-formed and Hawley retainers: a systematic review. Am J Orthod Dentofacial Orthop. 2014;145(6):720-7. 26. Lindauer SJ, Shoff RC. Comparison of Essix and Hawley retainers. J Clin Orthod. 1998;32(2):95-7. 27. Demir A, Babacan H, Nalcaci R, Topcuoglu T. Comparison of retention characteristics of Essix and Hawley retainers. Korean J Orthod. 2012;42(5):255-62. 28. Valiathan M, Hughes E. Results of a survey-based study to identify common retention practices in the United States. Am J Orthod Dentofacial Orthop. 2010;137(2):170-7; discussion 7. 29. Kacer KA, Valiathan M, Narendran S, Hans MG. Retainer wear and compliance in the first 2 years after active orthodontic treatment. Am J Orthod Dentofacial Orthop. 2010;138(5):592-8. 30. Artun J, Spadafora AT, Shapiro PA. A 3-year follow-up study of various types of orthodontic canine-to-canine retainers. Eur J Orthod. 1997;19(5):501-9. 31. Edman Tynelius G, Petren S, Bondemark L, LiljaKarlander E. Five-year postretention outcomes of three retention methods--a randomized controlled trial. Eur J Orthod. 2015;37(4):345-53. 32. Renkema AM, Renkema A, Bronkhorst E, Katsaros C. Longterm effectiveness of canine-to-canine bonded flexible spiral wire lingual retainers. Am J Orthod Dentofacial Orthop. 2011;139(5):614-21. 22 33. Dahl EH, Zachrisson BU. Long-term experience with direct-bonded lingual retainers. J Clin Orthod. 1991;25(10):619-30. 34. Loe H, Silness J. Periodontal Disease in Pregnancy. I. Prevalence and Severity. Acta Odontol Scand. 1963;21:533-51. 35. Silness J, Loe H. Periodontal disease in preganancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand. 1964;22:121-35. 36. Loe H. The Gingival Index, the Plaque Index and the Retention Index Systems. J Periodontol. 1967;38(6):Suppl:610-6. 37. Booth FA, Edelman JM, Proffit WR. Twenty-year followup of patients with permanently bonded mandibular canine-to-canine retainers. Am J Orthod Dentofacial Orthop. 2008;133(1):70-6. 38. Heier EE, De Smit AA, Wijgaerts IA, Adriaens PA. Periodontal implications of bonded versus removable retainers. Am J Orthod Dentofacial Orthop. 1997;112(6):607-16. 39. Pandis N, Vlahopoulos K, Madianos P, Eliades T. Longterm periodontal status of patients with mandibular lingual fixed retention. Eur J Orthod. 2007;29(5):4716. 40. Johnsson AC, Tofelt LN, Kjellberg H. Subjective evaluation of orthodontic treatment and potential side effects of bonded lingual retainers. Swed Dent J. 2007;31(1):35-44. 41. Noar JH, Evans RD. Rare earth magnets in orthodontics: an overview. Br J Orthod. 1999;26(1):29-37. 42. Ravindran KV. Review Article: Role of magnets in orthodontics—a review. Indian J Dent. 2011;2:147-55. 43. Bondemark L, Kurol J, Wennberg A. Biocompatibility of new, clinically used, and recycled orthodontic samarium-cobalt magnets. Am J Orthod Dentofacial Orthop. 1994;105(6):568-74. 23 44. Sukh R, Tandon P, Singh A, Singh GP. Role of Magnets in Orthodontics and Dentofacial Orthopedics: A Comprehensive Review. Trends in Biomaterials & Artificial Organs. 2013;27(3):131-7. 45. Evans RD, McDonald F. Effect of corrosion products (neodymium iron boron) on oral fibroblast proliferation. J Appl Biomater. 1995;6(3):199-202. 46. Drago CJ. Tarnish and corrosion with the use of intraoral magnets. J Prosthet Dent. 1991;66(4):536-40. 47. Kitsugi A, Okuno O, Nakano T, Hamanaka H, Kuroda T. The corrosion behavior of Nd2Fe14B and SmCo5 magnets. Dent Mater J. 1992;11(2):119-29. 48. Bondemark L, Kurol J, Wennberg A. Orthodontic rare earth magnets--in vitro assessment of cytotoxicity. Br J Orthod. 1994;21(4):335-41. 49. Yiu EY, Fang DT, Chu FC, Chow TW. Corrosion resistance of iron-platinum magnets. J Dent. 2004;32(6):423-9. 50. Hopp M, Rogaschewski S, Groth T. Testing the cytotoxicity of metal alloys used as magnetic prosthetic devices. J Mater Sci Mater Med. 2003;14(4):335-45. 51. Mancini GP, Noar JH, Evans RD. The physical characteristics of neodymium iron boron magnets for tooth extrusion. Eur J Orthod. 1999;21(5):541-50. 52. Noar JH, Wahab A, Evans RD, Wojcik AG. The durability of parylene coatings on neodymium-iron-boron magnets. Eur J Orthod. 1999;21(6):685-93. 53. Linder-Aronson A, Lindskog S. Effects of static magnetic fields on human periodontal fibroblasts in vitro. Swed Dent J. 1995;19(4):131-7. 54. Sato K, Yamaguchi H, Miyamoto H, Kinouchi Y. Growth of human cultured cells exposed to a non-homogeneous static magnetic field generated by Sm-Co magnets. Biochim Biophys Acta. 1992;1136(3):231-8. 55. Linder-Aronson A, Lindskog S, Rygh P. Orthodontic magnets: effects on gingival epithelium and alveolar bone in monkeys. Eur J Orthod. 1992;14(4):255-63. 24 56. Szabo G, Miklos L, Suba Z, Csendes P. Long-term tissue tolerance of titanium-encapsulated cobalt-samarium implants. J Long Term Eff Med Implants. 1992;1(4):34755. 57. Cerny R. The reaction of dental tissues to magnetic fields. Aust Dent J. 1980;25(5):264-8. 58. Bondemark L, Kurol J, Larsson A. Human dental pulp and gingival tissue after static magnetic field exposure. Eur J Orthod. 1995;17(2):85-91. 59. Saygili G, Aydinlik E, Ercan MT, Naldoken S, Ulutuncel N. Investigation of the effect of magnetic retention systems used in prostheses on buccal mucosal blood flow. Int J Prosthodont. 1992;5(4):326-32. 25 Chapter 3: Journal Article Abstract Introduction: Orthodontists have struggled with stability and retention after orthodontic treatment, especially in the lower anterior region. The MagneTainer™ is a new retainer design that utilizes magnets bonded to the lower anterior teeth and is an alternative to traditional fixed lingual retainers. It is bonded on all the marginal ridges from the mesial of the lower canine to the mesial of the contralateral canine to maintain the alignment of the lower anterior teeth and allows patients to floss straight down the contact without any additional flossing auxiliaries. Purpose: The purpose of this study is to compare the periodontal health of the lower anterior teeth retained with the MagneTainer™ versus a conventional fixed lingual retainer. Materials and Methods: The periodontal health of 32 patients bonded with the MagneTainer™ and 33 patients bonded with conventional fixed lingual retainers were evaluated utilizing a modified Gingival Index, modified Plaque Index, modified calculus index, and probing depths. A questionnaire was also given to each individual to assess their oral hygiene habits. Results: There were no significant differences in the GI Score, PI Score, Calculus Score, brushing frequency, and flossing frequency between 26 the two groups. More patients found it easier to floss with the MagneTainer™ than the conventional bonded lingual retainer. Conclusions: There were no differences in the periodontal health between the two groups. Patients with the MagneTainer™ found it easier to floss, however, it did not result in them flossing more. 27 Introduction Orthodontic supervision does not end once the appliances have been removed. Orthodontists and patients alike are concerned about the anticipated degree of stability following active orthodontic treatment, and it has been suggested that lifetime retention is necessary to maintain satisfactory alignment after treatment in many patients.1 Perfect alignment after orthodontic treatment is unrealistic over a lifetime and relapse is unavoidable. The orthodontic literature has shown that relapse following orthodontic treatment is unpredictable.1-4 The challenge that many orthodontists find in retention is that it is impossible to predict which cases will undergo relapse and to what degree it will occur.5 The words relapse, physiologic recovery, rebound, post-retention settling, and other similar terms have been used by orthodontic practitioners to describe the changes that occur after orthodontic appliances have been removed.6 Longitudinal studies have shown that during the posttreatment period, there is a trend towards decreased arch length, decreased arch width, increased overbite, increased overjet, and increased mandibular anterior crowding.1, 6-9 Sinclair and Little examined untreated cases from the mixed-dentition to early adulthood and found a decrease in 28 arch length, a small decrease in inter-canine width, minimal change in intermolar width, minimal change in overjet and overbite, and an increase in incisor irregularity.6 Blake and Bibby examined 15 potential factors of stability including arch form, periodontal tissues, mandibular incisor dimensions, neuromusculature balance, growth, post-treatment results, third molars, original malocclusion, extraction treatment, expansion, and non-extraction treatment.10 They concluded that orthodontist should aim to remove the primary burden of preventing relapse from the patient by maintaining treatment goals that follow well-documented principles.10 Even though there are many studies describing possible pre-treatment factors leading to relapse, most attempts have been unsuccessful at showing any reliable predictors of stability.11-13 Despite orthodontists’ best efforts, the best way to maintain satisfactory alignment post-treatment is through an indefinite period of retention.1 Relapse can occur anywhere in the dentition, but one of the more evident areas of potential instability is the lower anterior region.14-16 Long-term retention of the lower labial segment is necessary to prevent unwanted posttreatment changes, and bonded lower lingual retainers have 29 been utilized to maintain the alignment of the lower anterior teeth.17 Fixed lingual retainers have the advantages of being esthetically pleasing, virtually free of patient compliance, and reliable as part of the retention phase. Many studies have found that they are effective at maintaining incisor alignment post-treatment.18-21 The major disadvantages of fixed lingual retainers include the time consuming procedure, bond failures, stress fractures, and the tendency for plaque and calculus accumulation.18 Since the wire of a fixed lower retainer transverses the lingual surfaces of the mandibular anterior teeth, flossing and brushing can be more difficult. The result is a tendency for plaque and calculus to build up in the area of the retainer.22-25 A new form of fixed lingual retainer called the MagneTainer™ (Ft. Wayne, USA) is being introduced as an alternative to traditional fixed lingual retention. The MagneTainer™ was developed by Drs. Gene and Aron Dellinger of Ft. Wayne, Indiana. The MagneTainer™ utilizes neodymium iron boron magnets that are gold plated and sealed inside a stainless steel cover. They are bonded on all the marginal ridges from the mesial of the lower canine to the mesial of the contralateral canine and allows patients to floss 30 straight down the contact without any additional flossing auxiliaries. The MagneTainer™ has been shown to be as effective as a conventional fixed lingual retainer in maintaining incisor alignment at two years post-retainer placement.26 Rare earth magnets were developed in the 1970s and are known for their high coercivity and small size.27, 28 The two main types of rare earth magnets are samarium cobalt magnets and neodymium iron boron magnets. Orthodontics has utilized rare earth magnets in a variety of ways that includes treatment of unerupted teeth, tooth movement along arch wires, expansion, correction of anterior open bites, and functional appliances.27 Various studies have been done to test the biological safety of magnets by examining the effects of their corrosion products and magnetic fields.28-43 The evidence currently available from biological safety testing suggests that the conceivable risks of biological harm are negligible as long as the magnets are isolated from the intraoral environment either by being coated or encased in a protective casing.27-43 With the trend of using fixed lingual retainers for long-term retention, it is important to understand the effects that they have on the periodontal tissues surrounding the teeth. The purpose of this study is to 31 compare the periodontal health of the mandibular anterior teeth retained with the MagneTainer™ versus a conventional fixed lingual retainer. Materials and Methods There were two groups for this study: a MagneTainer™ group and a conventional fixed lingual retainer group. The MagneTainer™ group was from Dr. Aron Dellinger’s orthodontic practice in Ft. Wayne, Indiana. The conventional fixed lingual retainer group was acquired from Saint Louis University Center for Advanced Dental Education (St. Louis, MO) and Dr. Randall Brown’s orthodontic practice (Evansville, IN). The following inclusion criteria were used: lingual fixed retention, no cavities or restorations on mandibular anterior teeth, no dental cleaning within one month, and absence of smoking habits. A total of 65 patients participated in the study. The conventional fixed lingual retainer group had 33 patients and the MagneTainer™ group had 32 patients. All patients were seen at 2 months or more after orthodontic appliances have been removed. The fixed lingual retainer group had lingual retainers bonded on the canines. The periodontal health of the lower anterior teeth (canine to canine) was evaluated by one-examiner utilizing 32 a modified Gingival Index, modified Plaque Index, modified calculus index, and probing depths. Measurements were done on each tooth in the following gingival six areas: mesiobuccal (MB), buccal (B), distobuccal (DB), mesiolingual (ML), lingual (L), and distolingual (DL). An adaptation of Loe and Silness’s Gingival Index was used to determine the GI score of each patient.44 tooth was measured at the six gingival areas. Each Each of the six gingival areas were assigned a score from 0-3 based on the criteria for the Gingival Index system as seen in Table 3.1. The average of the scores of the six areas of a tooth gave the GI for the tooth. The average of all the GI’s of the individual teeth examined gave the GI for the individual. An adaptation of Silness and Loe’s Plaque Index system was used to determine the PI score of each patient.45 The individual locations, individual teeth, and overall individual scores were calculated similar to that of the Gingival Index system. The criteria for the Plaque Index system can be seen in Table 3.2. 33 Table 3.1: Criteria for the Gingival Index System adapted from Loe and Silness44 Criteria for the Gingival Index System Score 0 Description Normal gingiva 1 Mild inflammation – slight change in color, slight edema. No bleeding on probing 2 Moderate inflammation – redness, edema and glazing. Bleeding on probing 3 Severe inflammation – marked redness and edema, ulceration. Tendency to spontaneous bleeding Table 3.2: Criteria for the Plaque Index System adapted from Silness and Loe45 Criteria for the Plaque Index System Score Description 0 No plaque in gingival area 1 A film margin plaque across 2 Moderate accumulation of soft deposits within the gingival pocket, on the gingival margin, and/or adjacent tooth surface, which can be seen by the naked eye. 3 Abundance of soft matter within the gingival pocket and/or on the gingival margin and adjacent tooth surface of plaque adhering to the free gingival and adjacent area of the tooth. The may only be recognized by running a probe the tooth surface An adaptation of the Calculus Surface Index as described by Ennever et al. was used for calculus assessment.46 The total number of surfaces on which calculus was detected will be the patient’s calculus score. Probing depths were done from lower canine to lower canine using a number 12 UNC periodontal probe. 34 Probing depths were measured at the six gingival areas of each tooth. A questionnaire was given to each patient that related to his or her oral hygiene habits (see Figure A1). The patients were asked how often they brushed per day, how often they flossed, and if they found it difficult to floss. Error Study Three patients were selected at random from the control group and four patients were selected at random from the experimental group to be re-measured. All variables in both samples had intra-class correlation values of 90% or above. Statistical Analysis Independent samples Mann-Whitney U tests were done using SPSS® software (IBM Corporation, Armonk, New York). These tests were used to determine if there were any differences between the two groups in regards to Gingival Index Score, Plaque Index Score, Calculus Index, brushing frequency, and flossing frequency. An independent samples Mann-Whitney U test was done to compare flossing difficulty with Gingival Index Score, Plaque Index Score, Calculus Index, brushing frequency, and flossing frequency. Independent t-tests were used to compare the probing depths 35 between both groups. Spearman’s correlation coefficients were measured to determine the relationship between all variables. Results The mean of values of the GI score, PI score, Calculus score, brushing frequency, and flossing frequency can be seen in Table 3.3. There were no significant differences in the GI score, PI score, Calculus score, brushing frequency per day, and flossing frequency per day across the two retainer groups. The results of these tests can be seen in Table 3.4. Table 3.3 Mean, standard deviation, and standard error of the mean for the GI score, PI score, Calculus score, flossing frequency per day, and brushing frequency per day. Group Mean Standard Std Error Deviation mean Conventional 1.131 0.541 0.094 GI Score Magnetainer™ 0.940 0.441 0.078 Conventional 0.836 0.500 0.087 PI Score Magnetainer™ 0.688 0.372 0.066 Conventional 3.270 7.686 1.338 Calculus Magnetainer™ 2.380 4.210 0.744 Conventional 0.481 0.710 0.123 Flossing Magnetainer™ 0.358 0.428 0.076 Brushing Conventional 1.850 0.508 0.088 Magnetainer™ 1.880 0.609 0.108 36 Table 3.4 Independent samples Mann-Whitney U test were used to compare the two retainer groups with GI score, PI score, Calculus Index, flossing frequency per day, and brushing frequency per day. Significance GI Score 0.152 PI Score 0.265 Calculus Score 0.819 Brushing Frequency 0.775 Flossing Frequency 0.612 * Tests were significant with a p-value of ≤0.05 When patients were asked if they found it difficult to floss with their retainers, 84% of the MagneTainer™ group found it not difficult while 30% of the conventional bonded lingual retainer group found it not difficult. seen in Table 3.5. This can be There was a significant difference in the Plaque Index and flossing frequency per day when they were compared with the perception of flossing difficulty by the patient (see Table 3.6). Table 3.5 The frequency of patients reporting whether or not they found it difficult to floss n Difficult Not Difficult Conventional 33 23 (70%) 10 (30%) Magnetainer™ 32 5 (16%) 27 (84%) 37 Table 3.6 Independent samples Mann-Whitney U test were used to compare the difficulty of flossing with GI score, PI score, Calculus Index, flossing frequency per day, and brushing frequency per day. Significance GI Score .064 PI Score .001* Calculus Score .504 Flossing Frequency .047* Brushing Frequency .522 * Tests were significant with a p-value of ≤0.05 The correlations for the variables can be seen in Table 3.7. The GI score was highly correlated with both the PI score and flossing frequency. The frequency of flossing per day was slightly correlated with the GI score and the PI score. The difficulty of flossing was correlated with the frequency of flossing and plaque score. Table 3.7 Spearman’s correlation used to find relationships among GI score, PI score, Calculus score, flossing frequency per day, and brushing frequency per day. GI GI PI Calculus Brushing Flossing * Correlation Significance Correlation Significance Correlation Significance Correlation Significance Correlation Significance PI .654 < .001* 1 .654 <.001* .109 .552 -.343 .054 -.538 .001* 1 .166 .363 -.162 .377 -.427 .015* Calc .109 .552 .166 .363 1 .018 .920 .117 .616 Tests were significant with a p-value of ≤0.05 38 Brush -.343 .054 -.162 .377 .018 .920 1 .364 .041* Floss -.538 .001* -.427 .015* .092 .616 .364 .041* 1 There were significant differences in the probing depths for the following sites: L, LL2-L, LR3-ML, LR3-L. LL1-B, LR1-MB, LR3-B, LL3- These results can be seen in Table 3.8. Tables 3.8 Independent t-tests were used to compare the probing depths between both groups. Significant results shown. Group Mean Standard Std Error Sig. Deviation mean Conventional 1.33 .479 .083 .047 LL1-B Magnetainer™ 1.13 .336 .059 Conventional 1.67 .540 .094 .021 LR1-MB Magnetainer™ 2.03 .695 .123 Conventional 1.67 .479 .083 .030 LR3-B Magnetainer™ 1.41 .499 .088 Conventional 1.52 .508 .088 .037 LL3-L Magnetainer™ 1.25 .508 .090 Conventional 1.52 .508 .088 .005 LL2-L Magnetainer™ 1.19 .397 .070 Conventional 2.03 .467 .081 .027 LR3-ML Magnetainer™ 1.78 4.20 .074 Conventional 1.58 .502 .087 < .001 LR3-L Magnetainer™ 1.16 .369 .065 Discussion The periodontal health of the lower incisors and canines were determined by utilizing a Gingival Index, Plaque, and Calculus Index. When these were compared for each retainer group, there were no significant differences between the conventional bonded lingual retainer group and the MagneTainer™ group. The type of retainer did not make 39 a difference in the overall periodontal health of the patient. The GI score and PI score were correlated with flossing frequency. The more the patients flossed, the better their GI scores and PI scores were. There was no significant difference between the brushing habits between both groups, however, this does not take into account how well patients brush. Better oral hygiene resulted in better periodontal health regardless of the type of retainer. There were significant differences in probing depths at six locations. None of these differences were greater than 0.5 mm when comparing the means. These differences can be considered clinically insignificant. Patients with the MagneTainer™ in place found that it was less difficult to floss than those with the conventional fixed lingual retainer, however, patients with the MagneTainer™ did not floss more often than those with conventional fixed lingual retainers. Periodontal health was more dependent on the patient and their willingness to brush and floss rather than the retainer type. The MagneTainer™ makes it easier for the patient to floss, however, it does not encourage patients to floss more. As a result, there were no significant differences 40 in Gingival Index, Plaque Index, and Calculus Index between the conventional fixed lingual retainer group and the MagneTainer™ group. Conclusion 1. There were no significant differences in GI score, PI score, and calculus score between the conventional bonded lingual retainer group and the MagneTainer™ group. Thus there were no differences in periodontal health between the two groups. 2. GI score and PI score were correlated with flossing frequency 3. Patients with the MagneTainer™ found it less difficult to floss than those with the conventional bonded lingual retainer. 4. There was no significant difference in flossing frequency per day between the MagneTainer™ group and the conventional bonded lingual retainer group. 41 Literature Cited 1. Little RM, Riedel RA, Artun J. An evaluation of changes in mandibular anterior alignment from 10 to 20 years postretention. Am J Orthod Dentofacial Orthop. 1988;93(5):423-8. 2. Little RM, Riedel RA, Engst ED. Serial extraction of first premolars--postretention evaluation of stability and relapse. Angle Orthod. 1990;60(4):255-62. 3. Little RM, Riedel RA, Stein A. Mandibular arch length increase during the mixed dentition: postretention evaluation of stability and relapse. Am J Orthod Dentofacial Orthop. 1990;97(5):393-404. 4. Sadowsky C, Sakols EI. Long-term assessment of orthodontic relapse. Am J Orthod. 1982;82(6):456-63. 5. Barlin S, Smith R, Reed R, Sandy J, Ireland AJ. A retrospective randomized double-blind comparison study of the effectiveness of Hawley vs vacuum-formed retainers. Angle Orthod. 2011;81(3):404-9. 6. Sinclair PM, Little RM. Maturation of untreated normal occlusions. Am J Orthod. 1983;83(2):114-23. 7. Shapiro PA. Mandibular dental arch form and dimension. Treatment and postretention changes. Am J Orthod. 1974;66(1):58-70. 8. Johnson KC. Cases six years postretention. Angle Orthod. 1977;47(3):210-21. 9. Gardner SD, Chaconas SJ. Posttreatment and postretention changes following orthodontic therapy. Angle Orthod. 1976;46(2):151-61. 10. Blake M, Bibby K. Retention and stability: a review of the literature. Am J Orthod Dentofacial Orthop. 1998;114(3):299-306. 11. Shields TE, Little RM, Chapko MK. Stability and relapse of mandibular anterior alignment: a cephalometric appraisal of first-premolar-extraction cases treated by traditional edgewise orthodontics. Am J Orthod. 1985;87(1):27-38. 42 12. Fidler BC, Artun J, Joondeph DR, Little RM. Long-term stability of Angle Class II, division 1 malocclusions with successful occlusal results at end of active treatment. Am J Orthod Dentofacial Orthop. 1995;107(3):276-85. 13. Ormiston JP, Huang GJ, Little RM, Decker JD, Seuk GD. Retrospective analysis of long-term stable and unstable orthodontic treatment outcomes. Am J Orthod Dentofacial Orthop. 2005;128(5):568-74; quiz 669. 14. Kaplan H. The logic of modern retention procedures. Am J Orthod Dentofacial Orthop. 1988;93(4):325-40. 15. Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Syst Rev. 2006(1):Cd002283. 16. Rowland H, Hichens L, Williams A, Hills D, Killingback N, Ewings P, et al. The effectiveness of Hawley and vacuum-formed retainers: a single-center randomized controlled trial. Am J Orthod Dentofacial Orthop. 2007;132(6):730-7. 17. Zachrisson BU. Clinical experience with direct-bonded orthodontic retainers. Am J Orthod. 1977;71(4):440-8. 18. Artun J, Spadafora AT, Shapiro PA. A 3-year follow-up study of various types of orthodontic canine-to-canine retainers. Eur J Orthod. 1997;19(5):501-9. 19. Edman Tynelius G, Petren S, Bondemark L, LiljaKarlander E. Five-year postretention outcomes of three retention methods--a randomized controlled trial. Eur J Orthod. 2015;37(4):345-53. 20. Renkema AM, Renkema A, Bronkhorst E, Katsaros C. Longterm effectiveness of canine-to-canine bonded flexible spiral wire lingual retainers. Am J Orthod Dentofacial Orthop. 2011;139(5):614-21. 21. Dahl EH, Zachrisson BU. Long-term experience with direct-bonded lingual retainers. J Clin Orthod. 1991;25(10):619-30. 43 22. Heier EE, De Smit AA, Wijgaerts IA, Adriaens PA. Periodontal implications of bonded versus removable retainers. Am J Orthod Dentofacial Orthop. 1997;112(6):607-16. 23. Pandis N, Vlahopoulos K, Madianos P, Eliades T. Longterm periodontal status of patients with mandibular lingual fixed retention. Eur J Orthod. 2007;29(5):4716. 24. Johnsson AC, Tofelt LN, Kjellberg H. Subjective evaluation of orthodontic treatment and potential side effects of bonded lingual retainers. Swed Dent J. 2007;31(1):35-44. 25. Levin L, Samorodnitzky-Naveh GR, Machtei EE. The association of orthodontic treatment and fixed retainers with gingival health. J Periodontol. 2008;79(11):2087-92. 26. Armstrong A. Lower incisor stability comparing traditional bonded retainers to the MagneTainerTM: Saint Louis University; 2012. 27. Noar JH, Evans RD. Rare earth magnets in orthodontics: an overview. Br J Orthod. 1999;26(1):29-37. 28. Bondemark L, Kurol J, Wennberg A. Biocompatibility of new, clinically used, and recycled orthodontic samarium-cobalt magnets. Am J Orthod Dentofacial Orthop. 1994;105(6):568-74. 29. Drago CJ. Tarnish and corrosion with the use of intraoral magnets. J Prosthet Dent. 1991;66(4):536-40. 30. Kitsugi A, Okuno O, Nakano T, Hamanaka H, Kuroda T. The corrosion behavior of Nd2Fe14B and SmCo5 magnets. Dent Mater J. 1992;11(2):119-29. 31. Evans RD, McDonald F. Effect of corrosion products (neodymium iron boron) on oral fibroblast proliferation. J Appl Biomater. 1995;6(3):199-202. 32. Yiu EY, Fang DT, Chu FC, Chow TW. Corrosion resistance of iron-platinum magnets. J Dent. 2004;32(6):423-9. 44 33. Hopp M, Rogaschewski S, Groth T. Testing the cytotoxicity of metal alloys used as magnetic prosthetic devices. J Mater Sci Mater Med. 2003;14(4):335-45. 34. Noar JH, Wahab A, Evans RD, Wojcik AG. The durability of parylene coatings on neodymium-iron-boron magnets. Eur J Orthod. 1999;21(6):685-93. 35. Linder-Aronson A, Lindskog S. Effects of static magnetic fields on human periodontal fibroblasts in vitro. Swed Dent J. 1995;19(4):131-7. 36. Bondemark L, Kurol J, Wennberg A. Orthodontic rare earth magnets--in vitro assessment of cytotoxicity. Br J Orthod. 1994;21(4):335-41. 37. Sato K, Yamaguchi H, Miyamoto H, Kinouchi Y. Growth of human cultured cells exposed to a non-homogeneous static magnetic field generated by Sm-Co magnets. Biochim Biophys Acta. 1992;1136(3):231-8. 38. Cerny R. The reaction of dental tissues to magnetic fields. Aust Dent J. 1980;25(5):264-8. 39. Linder-Aronson A, Lindskog S, Rygh P. Orthodontic magnets: effects on gingival epithelium and alveolar bone in monkeys. Eur J Orthod. 1992;14(4):255-63. 40. Szabo G, Miklos L, Suba Z, Csendes P. Long-term tissue tolerance of titanium-encapsulated cobalt-samarium implants. J Long Term Eff Med Implants. 1992;1(4):34755. 41. Bondemark L, Kurol J, Larsson A. Human dental pulp and gingival tissue after static magnetic field exposure. Eur J Orthod. 1995;17(2):85-91. 42. Saygili G, Aydinlik E, Ercan MT, Naldoken S, Ulutuncel N. Investigation of the effect of magnetic retention systems used in prostheses on buccal mucosal blood flow. Int J Prosthodont. 1992;5(4):326-32. 43. Sukh R, Tandon P, Singh A, Singh GP. Role of Magnets in Orthodontics and Dentofacial Orthopedics: A Comprehensive Review. Trends in Biomaterials & Artificial Organs. 2013;27(3):131-7. 45 44. Loe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol Scand. 1963;21:533-51. 45. Silness J, Loe H. Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand. 1964;22:121-35. 46. Ennever J, Sturzenberger O, Radike A. The calculus surface index method for scoring clinical calculus studies. J Periodontol. 1961;32(1):54-7. 46 APPENDIX Figure A1: Questionnaire given to patients regarding oral hygiene habits 47 VITA AUCTORIS Don Dau was born in Portland, Oregon on November 29th, 1986 and was raised in Tampa, Florida. brother and a younger sister. He has an older Don attended the University of South Florida and graduated with a Bachelor of Science in Interdisciplinary Natural Sciences in 2009. Don graduated dental school from the University of Florida in 2013. He began his orthodontic training at Saint Louis University in 2013. 48