Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
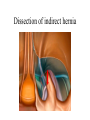
Hernia Dr. Nachmany Lecture Subjects • Anatomy – Inguinal & Femoral canals • Clinical aspects of hernia • Repair of Inguinofemoral Hernia: – Open – Rrhaphy; Tension free. – Laparoscopic The Inguinal Canal Anatomy, Embryology & Physiology Anatomy • Extends from the deep (fascia transversalis) to the superficial inguinal ring (ext. oblique) • Parallel and above the inguinal ligament • Walls of the Inguinal Canal: – – – – Anterior Posterior Superior Inferior Walls of the Inguinal Canal • Anterior wall - Aponeurosis of Ext. oblique – Reinforced in its lateral third by origin of the Int. oblique • strongest where it lies opposite the weakest part of the posterior wall (deep ring) Walls of the Inguinal Canal • Posterior wall - Fascia transversalis – Reinforced in its medial third by the conjoint tendon • Strongest where it lies opposite the weakest part of the anterior wall (superficial ring) Walls of the Inguinal Canal – Cont. • Inferior (floor) - Rolled-under inferior edge of aponeurosis of the Ext. oblique (→the inguinal lig.) • Superior (roof) - Arching lowest fibers of the Int. oblique and transversus abdominis muscles Deep Inguinal Ring • • • • ½ inch above the ligament Midway between ASIS and the Symphysis Lateral to the inferior epigastric vessels Margins of ring give origin to the internal spermatic fascia Superficial Inguinal Ring • Triangular defect in the aponeurosis of the external oblique • Immediately above and medial to the pubic tubercle • Margins give origin to the external spermatic fascia • Physical Exam Physiology and Mechanics Physiology • Inguinal canal - a passage through the lower abdominal wall • Males - to and from the testis • Females - round ligament of the uterus to the labium major • Both sexes – Ilio-inguinal nerve Mechanics of the inguinal Canal • A potential weakness • A design to lessen weakness: – Oblique passage → weakest areas lying some distance apart – Anterior reinforcement by Int. oblique in front of deep ring – Posterior reinforcement by Conjoint tendon behind superficial ring Mechanics of the inguinal Canal – Cont. • On coughing/straining (defecation, parturition etc.) → Int. oblique and transversus abdominis muscles contract → flattening the roof → canal is virtually closed Embryology • Processus Vaginalis • Spermatic Fasciae • Gubernaculum Embryology of the Inguinal Canal – Processus Vaginalis • Prior to testicular/ovarian descent a peritoneal diverticulum called the processus vaginalis is formed Embryology - Processus Vaginalis and creation of Spermatic fasciae • The processus vaginalis passes through the layers of the abdominal wall and acquires a tubular covering from each layer: – Fascia transversalis - Internal spermatic fascia – Lower part of Int. oblique muscle - it takes some of its lowest fibers (Cremaster muscle & Fascia) – Aponeurosis of the external oblique – Ext. spermatic fascia Spermatic Cord • Forms at the level of the Deep ring • It is covered with three concentric layers of fascia derived from the layers of the anterior abdominal wall Embryology oriented anatomy of spermatic fasciae Embryology - Gubernaculum • Extends from the lower pole of the developing gonad to the labioscrotal swelling • In the male the testis descends during the 7th and 8th months of fetal life Embryology - Gubernaculum • The stimulus for the descent is testosterone, secreted by the fetal testes • The testis follows the gubernaculum and descends behind the processus vaginalis • Pulls down its duct, blood vessels, nerves and lymphatics • In the female - extends from the uterus into the developing labium major • Persists as the round ligament Herniae of the Myopectineal orifice • A hernia - protrusion of part of the abdominal contents beyond the normal confines of the abdominal wall • Consists of: – Sac – Contents of the sac – Coverings of the sac • Complications: – Incarceration – Strangulation – Bowel obstruction Common Abdominal herniae are • Inguinal: – Indirect – Direct • Femoral • Umbilical: – Congenital – Acquired • Epigastric • Separation of the rectiabdominis • Diaphragmatic: – Sliding – Paraesophageal • Incisional (POVH) Indirect Inguinal Hernia • • • • • • The most common form of hernia 20 times more common in males one-third are bilateral more common on the right Congenital in origin Hernial sac is the remains of the processus vaginalis • The sac enters the inguinal canal through the deep inguinal ring lateral to the inferior epigastric vessels Direct Inguinal Hernia • About 15 percent of all inguinal hernias • Majority is bilateral • The sac bulges directly anteriorly through the posterior wall of the inguinal canal • Medial to the inferior epigastric vessels • A disease of old men with weak abdominal muscles. Femoral Hernia • The femoral sheath - a protrusion of the fascial envelope lining the abdominal walls • Surrounds the femoral vessels & lymphatics for 1 inch below the inguinal ligament The Femoral Canal • The femoral canal, the compartment for the lymphatics, occupies the medial part of the sheath. • Its upper opening is the femoral ring: – – – – Anterior -Inguinal ligament Posterior - Pectineal ligament and the pubis Medial - sharp free edge of the Lacunar ligament Lateral - Femoral vein • The femoral septum, which is a condensation of extraperitoneal tissue, plugs the opening • The femoral vein is separated from it by a fibrous septum Femoral Hernia • Much more common in women • The sac passes down the canal, pushing the septum • On the lower end, it forms a swelling in the upper thigh • With further expansion the sac may turn upward to cross the inguinal ligament • The neck always lies below and lateral to the pubic tubercle Surgical Repair of Hernia Classification • Those that close all or part of the myopectineal orifice • Anterior Vs. Posterior • Repair by suturing the tissues at boundaries: – Bassini – Shouldice – Cooper (McVay) • Those that cover the orifice with prosthetic mesh: – Lichtenstein – Plug and patch – Laparoscopic Anterior Repairs • Dissection and hernia reduction is the same: • incision 2 to 3 cm above and parallel to the inguinal ligament • Dissection through the subcutaneous tissues and Scarpa’s fascia • The external oblique fascia and external ring is identified • The external oblique fascia is incised to expose the inguinal canal • The ilioinguinal and iliohypogastric nerves should be preserved Open Repair – Cont. • The spermatic cord is mobilized at the pubic tubercle • The Cremaster muscle is divided and separated from the cord • The hernia sac is dissected from adjacent cord structures • The sac should be opened and examined for visceral contents if it is large • Neck of the sac is ligated at the level of the internal ring Herniorrhaphy • • • • Bassini Shouldice McVay (Coopers ligament repair) Ileopubic tract The Bassini repair • Suturing the conjoined tendon to the inguinal ligament • was the most popular repair before the tension-free repairs The Shouldice repair • Multilayer imbricated repair of the posterior wall of the inguinal canal with a continuous running suture technique: – 1st suture line - transversus abdominis aponeurotic arch to the iliopubic tract – 2nd line - internal oblique and transversus abdominis muscles and aponeuroses (Conjoint) to the inguinal ligament – 3rd line - Conjoint to Ext. oblique – 4th line - Conjoint to Ext. oblique 1st posterior suture - Transversus abdominis to Iliopubic tract 1st posterior suture - Transversus abdominis to Iliopubic tract (Cont.) 2nd posterior suture – Int. oblique and transversus abdominis to inguinal ligament 3rd posterior suture - Conjoint to Ext. oblique 4th posterior suture - Conjoint to Ext. oblique Relaxing incision Cooper Ligament (McVay) Repair • For correction of all the Myopectineal orifice: – – – – Direct inguinal hernias Large indirect hernias Recurrent inguinal hernias Femoral hernias • Transversus abdominis aponeurosis to Cooper’s ligament • Lateral to the medial aspect of the femoral canal , the transversus abdominis aponeurosis is secured to the iliopubic tract • An important principle - relaxing incision Lichtenstein Repair • Tension is the principal cause of recurrence • Synthetic mesh prosthesis to bridge the defect – Inferior suture line - Shelving edge of the inguinal (Poupart’s) ligament – Superior line – Conjoint muscle & tendon Posterior Repairs • Open Repair: – Stoppa – Laparoscopic • Trans Abdominal Pre-Peritoneal (TAPP) • Total Extra Peritoneal (TEP) Preperitoneal Anatomy What’s that? …and that? Danger areas The approach to the preperitoneal space Arcuate line (3) TEP TAPP Direct Hernia Indirect Hernia Trans-abdominal approach to the preperitoneal space Dissection of indirect hernia TAPP Post Op. Complications