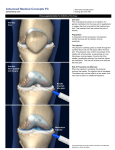
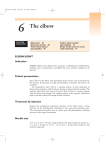
Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
JOINTS Injections & Aspirations Rationale • Primary care providers should master the technique of joint aspiration and injection for many reasons: – Diagnosing an inflamed joint – Pain relief of a distended joint – Injection of steroids for painful joint Indications • Diagnostic – To evaluate synovial fluid • • • • Infections Rheumatic Traumatic Crystal-induced etiology • Therapeutic – Remove exudate from septic joint – Relieve pain in grossly swollen joint – Inject lidocaine, saline, corticosteroids Contraindications • • • • Cellulitis or broken skin over entry site Anticoagulant therapy not well tolerated Septic effusion of a bursa More than 3 previous injections to weight bearing joint in last 12 months • Suspected bacteremia • Unstable joint • Inaccessible joint Contraindications • Absolute – – – – – Local sepsis Suspicion of infection Sepsis Hypersensitivity Early trauma – – – – – Hemarthrosis Prosthetic joint Very unstable joint Reluctant patient Children Contraindications • • • • • • • Diabetic Anticoagulated Bleeding disorder Immunosuppressed Psychogenic pain Severe anxiety Gut feeling Equipment • • • • • • • • Betadine Sterile gloves 22- to 27-gauge needle for injections 18-gauge needle for aspirations 10cc syringe 30cc syringe is aspirating large amount Lidocaine Culture tubes Pre-procedure Patient Education • Risks • Benefits • Possible complications – – – – Pain Infection Bleeding Tendon damage Technique • Before injection, consider differential. – X-rays if tumor or fracture possible • Identify entry site and mark • Prep with betadine • Inject wheel of lidocaine and advance for deeper anesthesia with 27-gauge needle • Use 18-gauge needle inserted into desired location and aspirate or 22-gauge and inject medication Lab Analysis of Fluid • White blood cell count – <50,000 inflammatory – >50,000 infectious • Polymorphonucleocyte percentage • Crystals • If fluid cloudy, culture Septic Arthritis • Infection occurs by : – – – – Hematogenous spread Contiguous source Direct implantation Postoperative complication Septic Arthritis • Early diagnosis essential: – – – – Growth impairment Articular destruction Osteomyelitis Soft tissue expansion Septic Arthritis • Neisseria gonorrheoae – Adolescents and young adults • Staphylococcus – Patients> 40, medical illnesses • Streptococcus N. gonorrhoeae • Majority in women – With or without anogenital symptoms • • • • Occurs during menstruation/pregnancy Positive culture 25%-60% Positive Gram stain 65% WBC and glucose helpful Synovial Fluid Analysis • • • • • String sign Cell count Glucose Gram stain Crystals Synovial Fluid Interpretation Diagnosis Appearance WBCs Glucose % blood level Crystals Culture Normal Clear <200 95+ None --- DJD Clear <4000 95+ None --- Traumatic Arthritis Straw, bloody, xanthochromic <4000 95+ None --- Acute Gout Turbid 200050,000 80-100 Needle like --- Pseudogout Turbid 200050,000 80-100 Rhomboid like --- Septic Arthritis Purulent/turbid 5000>50000 <50 None + usually Nontraumatic Arthritis Turbid 200050,000 75 None --- Joint Injection The Drugs Corticosteroids Rationale for Using Steroid Injection – Suppressing inflammation Short acting: Hydrocortisone Intermediate acting: Methylprednisone/Triamcinolone Long acting: Dexamethasone Side Effects • Systemic – – – – – – Facial flushing Uterine bleeding Deterioration of Diabetic glycemic control Significant falls in the ESR and CRP levels Other rare side effects Anaphylaxis Side Effects • Local – – – – – – – – Post-injection flare of pain Subcutaneous atrophy Bleeding or bruising Soft-tissue calcification Steroid arthropathy Tendon rupture Joint sepsis Soft tissue infection Local Anesthetics • Rationale for using – – – – Diagnostic Analgesic Dilution Distension • Commonly used – Lidocaine – Bupivacaine Safety Precautions • Aseptic Technique • Adverse Reactions – Syncope – Anaphylaxis Aspiration • • • • • • • Frank blood Serous fluid Serous fluid streaked Xanthochromic fluid Turbid fluid Frank pus Other Injection Technique • Equipment – – – – – Syringes Needles Corticosteroids Local anesthetic Dosage and volume Injection Technique • Technique – – – – – – Tissues Bursa and joint Tendons and ligaments Tendons with sheaths Blood vessels Aspirations Preparation Protocol • • • • • Prepare patient Prepare equipment Prepare site Assemble equipment Sterile technique Most Common Aspirations and Injections The Knee The Knee Landmarks: Medial patella – middle to superior portion Insertion 1 cm medial to anteromedial patella edge. Directed between posterior surface of patella and intercondylar femoral notch Knee Joint Lateral Medial Knee slightly flexed The Elbow The Elbow Landmarks Lateral epicondyle and radial head With elbow extended – the depression is palpated Insertion 22-ga needle from lateral aspect just distal to lateral epicondyle and direct medially The Elbow Lateral Epicondylitis (Tennis Elbow) Symptoms: pain with elevation of third digit against resistance, with wrist and elbow held in extension Approach: Point of Max Tenderness The Elbow Olecranon Bursitis Diagnosis obvious Approach: 20-ga needle into dependent aspect of sac The Wrist De Quervain’s Synovitis Injection: The needle is placed into the first extensor compartment and directed proximally toward the radial styloid. Questions?