Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Whither Teledermatology?
Why get a second opinion?
Help with……..
Diagnosis
Management
Confirmation of same
Patient driven
Why Teledermatology?
Visual
Poor relation
Non urgent
Common
Why Teledermatology?
Long waiting times
Long distances
Accurate
Diagnosis (hard) v. Management (easy)
Why Teledermatology?
True consultation.
What’s needed?
Patient
Camera
Computer/e-mail
‘Normal’ medical skills
The referring doctor has to…
Take and transmit images/history
Enact advice received
How long……????
Traditional referral
Dear Jim, please see re skin.
Yours sincerely
Telemedicine and you…..
Work load increased
Responsibility increased
Time commitment increased
Telemedicine and you…..
Educational opportunity
Financial opportunity?
Telemedicine and you…..
Acquire new skills?
Wet wraps, dressings, dithranol, efudix,
surgery, phototherapy, isotretinoin etc etc
Telemedicine and you…..
Increased patient demand.
Dermatology patients expand to meet the
number of dermatologists available.
Telemedicine and you…..
“Don’t you think you should check with the
teledermatologist?”
Telemedicine and you…..
Fewer patients lost in ‘specialist land’
Telemedicine and you…..
Medicolegal issues?
Who is responsible?
Where does the consultation take place?
Informed consent?
Privacy concerns?
Telemedicine and you…..
Cost you or make you money??
Will you use it if it costs you money?
Telemedicine and you
Should the existence of telemedicine
services be advertised to the general
public if they can only access them
through a doctor?
Teledermatology and the
patient…….
Rapid access
Decreased cost
No travel
?Equal service
Telemedicine and you
Should patients be able to directly
access specialist telemedicine
services?
Tele-Derm Consults
Examples of Cases Submitted to
Jim
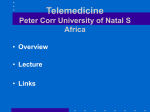
Flaky Rash Face and Arm
• I submit this case on behalf of a colleague who has no
access to the internet at the remote location. 21/10, 15:58
" a 42 year old indigenous
lady from Groote Eyland
(NT)who presents at Lockhart
River (Qld) with a one year
history of these raised flaky
lesions which started around
the lips, now has spread to
nose and cheek with some
lesions starting on the left
upper arm. A biopsy was
reported as "non specific
inflammation" only."
What is this?
Jim’s Reply 21/10 17:47
• This should be discoid lupus. The lip is pretty classic [a
diagnosis I missed on an aboriginal woman in Mossman in
1986].
Ask the lab to review the histology with that diagnosis in
mind.
If no luck with path review repeat biopsy from non ulcerated
skin.
Do ANA/ENA etc for SLE and work up for plaquenil. Sun
protection and potent topical steroids will help but need
diagnosis first. See case 400 and 344 for much less severe
examples.
To be complete I'd throw leprosy and nasty tinea into
differential but if this isn't lupus I will return to my singing
career!
jim
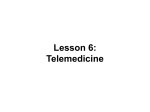
30/9, 14:07
• Just after some input on this 3yo boy who
has a 1 month history of well demarcated
skin lesions.
• These were initially treated with an antifungal
cream which has had no effect.
• The lesions become more pronounced when
exposed to the sun, appear dry, and have scaly
skin on the peripheries of the lesions. They are
on his cheeks, neck, and anterior torso.
• The child is otherwise well. I am considering
psoriasis or discoid eczema and have a
prescribed a few days of a moisturiser to see if
this has effect.
Would lupus present like this?
Jim’s Reply 30/9, 16:04
• They look eczematous to me. Probably endogenous dermatitis i.e.
atopic.
Ask re history of same.
{in an adult on those snaps I would have included mycosis fungoides
and leprosy too!!]
Suggest fungal scrape, emollient and some steroid ointment. Use a
potent one e.g. diprosone/elocon fo three or four days and then reduce
to celestone M [ointment not cream].
Use 1% hydrocortisone ointment on face.
Review at 1 week.
Make sure they really push the moisturiser.
Keep me posted.
There is some post inflammatory hypopigmentation which explains the
more prominence with sun possibly i.e. the non - affected skin darkens.
Am in the wilds of NSW at the moment.
Case Submitters Response
• Just to let you know that this child had a
good response to the topical steroids with
barely any lesions remaining. His mother
will keep up with the skin moisturisers.
Dx Eczema!
Jim’s Response
• Good one!!
It will probably recur but the emollients are
vital.
They need to try to minimise steroid use in
the long term but not be afraid of it!
Persistent Itchy Rash 10/10 11:38
History:
• Started in groin and upper thighs
and lower abdo
• Spread to chest arms hands + lower
legs
• Used pinetarsal some relief initially
• Using loafer on skin
• Using soap free wash
• Having 6 showers per day
• Used scabies treatment initially with
no effect
• Ceased perindopril 6/52 ago
• Some improvement
• Has reoccurred again worse on
lower abdomen
• Steroid creams used with no effect
• Phenergen making very drowsy so
not using
• RAST -ve
• Had itchy rash for 3/12
Examination:
• Scratch marks ++
• ? herald patch abdo
• Confluent areas on posterior elbows +
over scapula bilaterally
• Upper arms and lower abdo + upper back
worst areas
• Also web spaces and creases of wrists
• groin + legs
• Red papules in clusters
Diagnosis:
Medications:
• Aspirin 100mg Tablets 1 in the morning with food
• Atorvastatin calcium 20mg Tablets 1 at night
• Elocon 0.1% Cream apply daily
• Glucosamine sulfate 1000mg Capsules 1 in the morning with food
• Indapamide hemihydrate 1.5mg Tablet SR 1 in the morning
• Mobic 15mg Tablet 1 in the morning with food
• Norvasc 10mg Tablets 1 in the morning
• Phenergan Tablets 25mg Tablets 1 tab
• Tenormin 50mg Tablets 1 in the evening
Plan:
• Skin scarpings and send photos and story to telederm for further advice.
Stop scratching + using washer in shower to scratch. Restrict showers.
cetaphil wash only. Moistuiser bd. Try non sedating anti-histamine. Avoid
heat.
• Cessation of perindopril seemed to help initially but it has since gotten
wrose while off perindopril. The rash as described is extensive and
extremely itchy which I felt was not consistent with pityriasis. I performed a
skin scraping which has come back negative on microscopy with culture
pending. I have attached some photos. Thank you for reviewing and
advising on further investigation/ treatment.
• ? Pityriasis rosacea ? Drug reaction
Jim’s Reply 10/10 13:47
•
On the images he has eczematous areas and also on the back some
lesions of Grovers disease.
Sudden onset like this think drug reaction and scabies.
Ask re itchy penis/scrotum and look carefully for burrows especially
between fingers. Ask if anyone at home itchy.
Do a couple of 3 mm punch biopsies and let me know the results.
If no evidence of scabies and after biopsies done start on Elocon ointment
[not cream] b.d. with wet wrap occlusion applied for half an hour after a
shower.
Let me know the histology.
We then may have to start stopping medications. See if you can work out
what was most recently started and ensure list is complete i.e. no hidden
drugs.
If find evidence of scabies need whole household treated with Lyclear.
Let me know results.
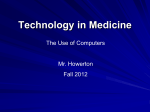
Case Submitters Response
• Scabies was certainly high on the list initially particularly
given the appearance of the hands (see photos). He and
his partner (who has no symptoms) were both treated
with Permethrin with no improvement.
He has been taking Atorvostatin for many years
The rash has gotten worse since cessation of perindopril
I will take some punch biospies and send you the results.
Do you think we should stop atorvostatin in the
meantime ?
Thanks for your help
Jim’s Reply
• No wait and see.
Scabies is a classic thing to fail treatment.
If he has itchy bits on his genitals it is proabbaly
scabies so ask and look!
See case 111
Case Submitters Response
• He did indeed have genital itch + rash
early on. I have asked him to retreat with
Lyclear and his partner will also be treated.
Will he need to repeat the treatment after
1/52 ?
The biopsy result is pending
Jim’s Reply
• No point half doing it. Repeat treatment is
to kill the recently emerged babies after
hatching but before they breed.
Will be interested to hear how he fares.
Case Submitters Response 21/10
• I received a lovely bunch of flowers today and a request
to thank you also from a very relived man who can sleep
again ! He had an improvement by 1/7 post Lyclear
which he interestingly did not get with the first treatment.
The rash has improved dramatically already.
Interestingly I had a phone call from the pathologists
today asking if the rash could be syphilus prior to
reviewing the patient later today.
Thanks again
Jim’s Reply
• Very interesting!
If they fail to improve and it is scabies
there are a lot of possible reasons
[reinfestation, secondary eczema, irritation
from the treatment, scabetic nodules, post
scabetic itch etc].
Why did they wonder about syphilis?
SETS
SKIN
EMERGENCY
TELEMEDICINE
SERVICE