Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
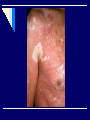
Papulo-squamous diseases Dr.MOHAMED NASR Lecturer Of Dermatology & Venereology Zagazig University PSORIASIS It is a chronic proliferative skin disease that affects about 1-2% of general population. Cause: Genetic predisposition with triggering factors: Trauma: can elecit (koebner phenomenon). Weather: worse in winter. Endocrinal factors: It may improves with pregnancy and exacerbate with puberty and menopause. Infection: steptococcal infection may be followed by guttate psoriasis . Drugs: ß adrenergic blockers, NSAIDs and ACE inhibitors. Emotional stress. Alcohol and smoking. Histopathology Epidermis: Parakeratosis (accelerated incomplete keratinization of horny cells with retension of neuclei) with focal orthokeratosis. Absent granular cell layer. Regular acanthosis and elongation of club shaped rete ridges. Suprapapillary thinning of epidermis. Munro microabscesses formed of collected neutrophils in stratum corneum or just beneath it. Spongiform pustules in malpighian layer. Dermis: Elongation and edema of dermal papillae. Dilated tortuous capillaries in the upper portion of papillae. Perivascular mononuclear and neutrophil inflammatory infiltrate in upper dermis. Clinical picture: The primary lesion is a salmon pink papule covered with silvery scales. Papules may enlarge or coalesce forming plaques. Sites: extensor surfaces of limbs, elbows, knees, scalp, and nails. Grattage test Scraping of psoriatic lesion with the edge of a glass slide results in removal of the scales layer after layer with accentuation of the silvery appearance until a smooth glossy red membrane is finally left. On scratching this membrane pinpoint hemorrhages appear (Auspitz's sign). Morphological patterns 1-Punctate psoriasis (pin point size) 2-Guttate psoriasis (size of drops) 3-Discoid psoriasis (coin shaped) 4-Annular psoriasis (ring shaped lesions produced by involution of center of the lesions) 5-Geographical psoriasis (curved patterns produced on a large area as the back). 6-Linear psoriasis Clinical varieties - Flexural psoriasis: as in axillae and groins. - Psoriasis of palms and soles: may be either; Typical scaly plaques Or thick, fissured plaques similar to hyperkeratotic eczema Or pustular type - Erythrodermic type: generalised erythema and scaling. - Psoriasis of nails: pitting, yellowish discolouration, circular area of discolouration (oil drop) transverse ridging, onycholysis (distal separation), thickening, subungual hyperkeratosis. - Arthropathic psoriasis. - Psoriasis of scalp: not crossing the hair line (D D from seborrheic dermatitis). - Pustular psoriasis: localised or generalized, the primary lesions here is a sterile pustule. Flexural psoriasis Psoriasis of palms and soles: Erythrodermic psoriasis: Psoriasis of nails: Psoriasis of scalp: Pustular psoriasis: Pathogenesis: Epidermal keratinocyte hyperproliferation. The transit time of epidermal cell maturation from a basal cell to be a horny cell in normal skin is about 26-28 days whereas in psoriatic skin it is only 3-4 days. T-cell mediated inflammatory involving mainly Th1 cells. process Koebner phenomenon: It is development of isomorphic pathologic lesions in the traumatized uninvolved skin of patients who have psoriasis. Psoriasis, warts, lichen planus, vitiligo, molluscum contagiosum and pityriasis rubra pilaris (PRP). Treatment: A-Topical treatment 1-Tar :crude coal tar 2-5%. 2-Anthralin 0.1-1%. 3-Salicylic acid (3-5%) keratolytic remove scales. 4-Corticosteroids ointment. 5-Intralesional corticosteroid injection of triamcinolone acetonide in localised resistent plaques but less effective in nail psoriaisis. 6-Calcipotriol ointment (vitamin D analogue). It inhibits keratinocyte proliferation. B-Systemic treatment 1-Methotrexate 2.5mg tab (5mg every 12 hour for 3 doses) every week. It is indicated in erythrodermic psoriasis and generalized pustular psoriasis. Liver function should be monitored. 2-Retinoids; etretinate: 1 mg/kg/day and acitretin 0.5-1 mg/kg/day in severe cases and erythrodermic psoriasis 3-Photochemotherapy (PUVA): psoralens 0.6 mg/kg 2 hours before the exposure to UVA rays 2-3 times weekly 4- Phototherapy: narrowband UVB rays (NBUVB) 5-Cyclosporin A: immunosuppresive for severe cases 2.55mg/kg/day. LICHEN PLANUS Lichen planus is an itchy chronic inflammatory disease which affects skin and mucous membranes. Pathogenesis: 1-Genetic predisposition 2-Autoimmune 3- Strong association with hepatitis C infection 4- Emotional stress Clinical picture The primary lesion is a pruritic shiny violaceous flat topped polygonal papule which retains the skin lines and shows white streaks (wickham’s striae). These striae can be seen well with a magnifying lens. It is commonly seen on wrist, back of hands, shin and ankles in hypertrophic type, lumbar region, glans penis in annular type and palms and soles. Mucous membrane lesions are very common (in 30-70% of cases) and may occur alone without skin involvement. After disappearance of the lesions deep pigmentation is left for several months Clinical varieties: 1- Atrophic lichen planus; fading annualr or hypertrophic type. 2- Hypertrophic Lichen planus: deep violet rough papules over shin of tibia and ankles. 3- Linear lichen planus. 4- Annular lichen planus (on glans penis). 5- Lichen planus bullosus. 6- Lichen planus circinatus. 7- Lichen plano-pilaris: follicular papules which result in cicatricial alopecia. 8- Lichen planus actinicus: on sun exposed areas in the form of annular lesions with violet brown centre and well defined hypopigmented margin. 9- Lichen planus of mucous membrane: (White streaks or network on the buccal mucosa, fixed white plaques on the tongue or ulcerative lesions). 10- Lichen planus of palms and soles: firm rough non itchy deep yellowish papules. 11- Lichen planus of the nails: thinning of nail plate, linear ridges and grooves, adhesions between dorsal nail fold and nail bed may cause partial destruction of nail (pterygium). Histopathology: 1-Compact hyperkeratosis. 2-Focal hypergranulosis. 3-Irregular acanthosis and irregular elongation of rete ridges giving a (saw toothed appearance). 4-Liquefactive degeneration of basal layer. 5-Band like inflammatory infiltrate. Treatment: 1-Assurance and avoidance of stress 2-Topical therapy: a- Fluorinated topical steroid ointment b- Topical tacrolimus c- Intralesional steroids (Hypertrophic LP and lichen planus of nail) 3-Systemic therapy: a-Antihistamines b-Systemic steroids (15-20mg/day for 6 weeks) indicated in: 1-severs pruritic or generalized cases 2-ulcerative mucous membrane lesions 3-progressive nail destruction 4-extensive lichenplanopilaris to prevent cicatricial alopecia c- Retinoids d- Cyclosporin A e- Antimalarials for actinic L.P f- NBUVB and PUVA PITYRIASIS ROSEA It is an acute self limited disorder characterized by superficial, scaly lesions on the trunk. It is more common in spring and autumn. Clinical picture: 1- The primary lesion is the herald patch. 2- It is followed after 5-15 days by multiple similar macules or patches. 3- The long axes of lesions follow lines of cleavage parallel to the ribs in a Christmas tree pattern on the upper chest and back. 4- The eruption fades within 4-8 weeks. Types: 1- Classical type. 2- Inverted type. 3- Abortive type. 4- Localised type. Etiology: a- Infective agent: virus (HHV6-7). b-Drug induced (pityriasiform drug eruption) as captopril, metronidazole, ketotifen and barbiturates. c- Autoimmune disease. Treatment: 1-Reassurance 2-Antihistaminics 3-Calamine lotion 4-Narrow band UVB PITYRIASIS RUBRA PILARIS This is a chronic disease characterized by follicular hyperkeratosis, branny scales, orange red erythema and palmoplanter keratoderma. Etiology: Unknown. It may be dominantly inherited. Vitamin A deficiency is also reported. Clinical signs: 1-Diffuse scaliness of scalp. 2- Patches showing keratotic follicular papules. 3- Dry scaly erythematous areas simulating psoriasis. 4- Hyperkeratosis of palms and soles. 5- Follicular hyperkeratosis of proximal phalanges of fingers and toes. 6- Nails: dull, thickened rough dystrophic. 7-Erythroderma with islands of normal skin. Types: 1. 2. 3. 4. 5. Classical adult type (most common 55%) Atypical adult type (5%) Classical jeuvenile type (10%) Circumscribed jeuvenile type (25%) Atypical jeuvenile type (5%) Treatment: 1-Emollients in cases of erythroderma to reduce scaling and restore skin barrier 2-Topical steroids and salicylic acid ointment 3-Topical vitamin D analogues (calcipotriol) 4-Oral Vit A: 150,000-300,000 IU/day 5-Isotretinoin and acitretin 6-Methotrexate 10-25mg/week 7-Narrow band UVB 8-PUVA alone or/and oral retinoid