Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Vectors in gene therapy wikipedia , lookup
Patient safety wikipedia , lookup
Medical ethics wikipedia , lookup
Gene therapy wikipedia , lookup
Gene prediction wikipedia , lookup
Public health genomics wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Electronic prescribing wikipedia , lookup
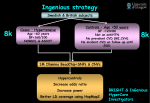
Pharmacogenetics: From DNA to Dosage – Just A Click Away Cindy L. Vnencak-Jones, PhD, FACMG Vanderbilt University Medical Center April, 2011 DISCLOSURE INFORMATION Cindy L Vnencak-Jones, PhD FACMG No relationships to disclose Pharmacogenetics: From DNA To Dosage – Just A Click Away Pharmacogenetics: • influence of genetic variation on an individual’s response to pharmacologic agents • Pharmacogenetics testing is not routinely used in clinical practice • when ordered, is done “as needed” preventing usefulness for initial dosing • many drugs, many genes, many studies result in information overload for the provider Pharmacogenetics: From DNA To Dosage – Just A Click Away PREDICT: Pharmacogenomic Resource for Enhanced Decisions In Care and Treatment PREDICT Initiative Rationale Provide real-time decision support thereby facilitating individualized drug therapy to maximize efficacy, minimize adverse drug reactions, and reduce health care costs PREDICT Initiative Assemble multidisciplinary, multidepartment team Pathology, Informatics, Pharmacy, Clinicians, Ethics, Legal, Regulatory Proof of Concept Which drug/gene relationship should test the model? Genotyping Which methodology? Research or CLIA lab? Informatics Data management, Electronic health record, decision support Implementation – 9/15/2010 Assessment of the initiative – ongoing Measure utility of decision support and clinical impact of genotyping PREDICT Initiative Office of Personalized Medicine Pharmacy and Therapeutic Committee Vanderbilt University Ethics/Legal/ Regulatory PREDICT Vanderbilt Informatics Center VUMC Computational Genetics Core Molecular Diagnostics Lab Clinicians Optimize Patient Management PREDICT Process – Phase I • Consent process – Adult Admitting & ED Registration – “CONSENT FOR ROUTINE TESTS, MEDICAL TREATMENT, AND GENETIC TESTS TO GUIDE DRUG THERAPY…” • Provider discusses genotyping studies – Blood drawn • Sample arrives in laboratory – DNA extracted (day 1) – Assay performed (day 2) – Results reviewed and released (day 3) PREDICT Process – Phase I • Raw data converted to drug genome interaction fact for computerized decision support in electronic health record (EHR) • Provider accesses EHR; alerted to results • Provider receives decision support regarding dosing or alternative medications • Provider optimizes patient management utilizing information provided by genotyping studies PREDICT Model Clopidogrel (PLAVIX) –CYP2C19 • FDA issued a “black box” warning regarding the clinical relevance of genotype analysis • Widely prescribed to patients at our medical facility • Could provide decision support and measure the change in prescribing behavior of the provider based on the given decision support • Targeted patient population to launch model – the cardiac catheterization lab FDA – Black Box Warning Issued March 12, 2010 WARNING: DIMINISHED EFFECTIVENESS IN POOR METABOLIZERS • Effectiveness of Plavix depends on activation to an active metabolite by the cytochrome P450 (CYP) system, principally CYP2C19. • Poor metabolizers treated with Plavix at recommended doses exhibit higher cardiovascular event rates following acute coronary syndrome (ACS) or percutaneous coronary intervention (PCI) than patients with normal CYP2C19 function. • Tests are available to identify a patient's CYP2C19 genotype and can be used as an aid in determining therapeutic strategy. • Consider alternative treatment or treatment strategies in patients identified as CYP2C19 poor metabolizers. Clopidogrel - PLAVIX Simon T. et al, N Engl J Med 2009 • Requires gastro-intestinal absorption and hepatic biotransformation • Is an inhibitor to the P2RY12 receptor thereby preventing binding of ADP • Increases risk of bleeding; especially GI bleeding when combined with warfarin and nonsteroidal antiinflammatory drugs Clopidogrel - PLAVIX Prodrug CH3 Active CH3 • Antiplatelet therapy, often prescribed in combination with aspirin • Initial dose 300 mg followed by 75 mg daily • Indications for use: acute coronary syndrome; recent myocardial infarction or stroke; peripheral arterial disease; or patients managed following angioplasty, bypass surgery or stent placement Drug Metabolizing Enzymes Phase I Modification of functional groups: Hydrolysis Oxidation Dealkylation Dehydrogenation Reduction Deamination Desulfuration Evans and Relling, Science 1999 Phase II Conjugation with endogenous substituents to form: Glucuronide Acetate Glutathione Sulfate Methionine VeraCode ADME Core Panel • Absorption • Distribution • Metabolism • Excretion ADME Core (34 genes, 185 markers) ABCB1 CYP2C9 NAT1 SULT1A1 ABCC2 CYP2D6 NAT2 TPMT ABCG2 CYP2E1 SLC15A2 UGT1A1 CYP1A1 CYP3A4 SLC22A1 UGT2B15 CYP1A2 CYP3A5 SLC22A2 UGT2B17 CYP2A6 DPYD SLC22A6 UGT2B7 CYP2B6 GSTM1 SLCO1B1 VKORC1 CYP2C19 GSTP1 SLCO1B3 CYP2C8 GSTT1 SLCO2B1 Illumina CYP2C19 Multiple polymorphic sites with clinical significance W120R c.358T>C *8 g.-806C>T *17 W212X c.636G>A CYtochrome P450 Family 2 Subfamily C polypeptide 19 *3 X491C c.1473A>C *12 3’ 5’ *4 c.1A>G ATG>GTG *6 *2 c.681G>A c.395G>A R132Q *7 g.19294T>A P681P Location: 10q24.1 – q24.3 Gene: 90,209 bases mRNA: 1,473 Protein: 490 amino acid *5 c.1297C>T R433W missense truncation splicing promoter initiation codon insertion CYP2C19 – Clopidogrel Patients with reduced function alleles have: – significantly lower levels of the active metabolite –diminished platelet inhibition and higher rate of platelet aggregation –higher rate of major adverse cardiovascular events and higher risk of stent thrombosis ADME Assay Design Gene 1:SNP-1 CCCTACACAGATGTGGTGCACGAGGTCCAGAGATACATTGACCTTCTCCCCACCAGCCTGCCCCATGC A GGGATGTGTCTACACCACGTGCTCCAGGTCTCTATGTAACTGGAAGAGGGGTGGTCGGACGGGGTACG T Gene 1:SNP-2 Gene 1:SNP-3 SNP-3 SNP-2 Patient 1 Patient 30 SNP-1 SNPs Optimized in 3 pools + control - control Adapted from Illumina Assay – Primer Design Universal PCR Forward Sequences (1, 2) 5’ A Universal PCR Reverse Sequence 3 3’ 3’ G SNP (1-20 nt gap) 5’ Locus Specific Oligo Locus Specific Oligos A/G IllumiCode ™ Sequence tag identifies bead GENOMIC DNA TEMPLATE SNP Adapted from Illumina Assay – Allele Specific Extension and Ligation Polymerase GENOMIC DNA Universal PCR Sequence 1 T A Ligase SNP specific primer binds and is extended Universal PCR Sequence 2 IllumiCode Sequence Tag Universal PCR Sequence 3 G Adapted from Illumina Assay – PCR Amplification Polymerase IllumiCode Sequence Tag Universal PCR Sequence 1 Universal PCR Sequence 3 Biotin Cy3 Universal Primer 1 Cy5 Universal Primer 2 A Primer specific for G with red dye does not bind Adapted from Illumina VeraCode Technology – the glass microbead • Cylindrical glass microbeads • 240 μm length x 28 μm diameter • Bar-coded for identification Adapted from Illumina Assay - Hybridization of PCR Products to VeraCode Beads A IllumiCode 1 SNP 1 G IllumiCode 2 A/A SNP 2 Homozygous IllumiCode 3 SNP 3 T C G/G Homozygous Red and green signal detection with the BeadXpress Reader C/T Heterozygous Adapted from Illumina BeadXpress Reader Adapted from Illumina VeraCode Bead Loading & Detection CAPILLARY FORCE ATTRACTS BEADS INTO GROOVES BEADS FALL INTO GROOVE PLATE BEADS ALIGN TIGHTLY FOR OPTIMAL SCANNING EFFICIENCY Adapted from Illumina VeraCode Bead Plate Scanning Reports with Automatic Translation Visualization of the Results PREDICT Database Samples with call rates >97.34% “Pass” Electronic Health Record Electronic Health Record Currently, CYP2C19 results sent to EHR, all other data is stored but can be sent to EHR in the future when drug genome interactions decisions become “actionable” Electronic Prescription Order Electronic Prescription Order Clopidogrel Response CYP2C19 Genotype RACE *2*2 *2 HET WT Caucasian 5% 21% 74% • Genetic Factors – Polymorphisms in CYP2C19 and other CYPs, as well as SNPs in P2RY12,GpIIb/IIIa • Cellular Factors African American 3% 24% 73% Asian 7% 43% 50% – P2RY12 and non P2Y pathways • Clinical Factors – Drug-drug interactions, ADME QA/QC • Allele frequencies of all genotypes • Discordant results: controls and repeat patients (which SNPs and frequency) • Assay performance: # of samples per plate with average call rates <97.30% (7/185 SNPs no call) • Locus performance (<95% call rates) PREDICT Results 9/15/10 - 4/4/11 *1*1 *1*17 *1,*2 *1,*3 *1,*4 *1*5 *1*7 *1*8 *1*12 *2*17 *17*17 1419 patients *5*5 *4*4 *3*3 *2*2 Assay Accuracy Controls Average Concordance Paragon Control Cell Lines 99.58% Coriell Control Cell Lines 98.34% Assay Reproducibility 150 patients repeated ADME QA/QC Paragon controls # of plates Locus Performance (<95% call rates) 80 plates Summary • Implemented a mid-throughput assay to screen 34 genes (185 SNPs) involved in drug absorption, distribution, metabolism and excretion • Detected polymorphisms similar in frequencies to that previously reported • Established QA/QC parameters for assay • Developed a process to enable decision support to providers for drug dosing based on DNA findings which will facilitate genetically informed medicine Summary • Implemented a scalable process to allow expansion to other actionable SNPs with associated decision support rules • Process enables retrospective auto-population of stored data in patients EHR for future without the need for repeat testing • Measure clinical utility and impact of genotyping data and decision support services • Phase II - system permits identification of “at risk” patient populations for preemptive genotyping Acknowledgements Vanderbilt University Nicholas Zeppos - Chancellor Jeff Balser, MD, PhD – Vice Chancellor VUMC Gordon Bernard, MD – Vice Chancellor Research Office of Personalized Medicine Dan Roden, MD PREDICT Implementation Team Jill Pulley, MBA Russ Wilke, MD Jim Jirjis, MD Josh Peterson, MD John McPherson, MD Andrea, Ramirez, MD Mike Laposata, MD, PhD Center for Biomedical Ethics and Society Ellen Clayton, MD, JD Kyle Brothers, MD Molecular Diagnostics Lab Gladys Garrison, MS Jennifer Carter, PhD Lisa Rocha Sonia Byon Vickie Fraser VUMC Computational Genetics Core Holli Dilks, PhD Doug Selph Brad Winfrey Vanderbilt Informatics Center Dan Masys, MD Joshua Denny, MD Ed Shultz, MD Marc Beller Pharmacogenetics: From DNA to Dosage – Just A Click Away Cindy L. Vnencak-Jones, PhD, FACMG Vanderbilt University Medical Center April, 2011