Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
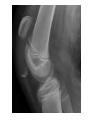
LAWRENCE PICCIONI MD Current team physician for Delaware State University since 1993 Team physician for Wesley College 1992 to 2004 Team physician for Dover High School 1992 to 2004 Familiarize you with common features of injuries Reinforce what you already know about diagnosis and treatment Help decision making as far as treatment or referral Reviewing pertinent anatomy, History and Physical findings Review differences in adult and pediatric injury patterns Give some PEARLS Bones more pertinent in pediatric group Tendons – Patellar and Quadriceps Cartilage – articular and meniscal Ligaments – ACL, PCL, Medial and lLateral Collateral Cartilage is like a rock in your shoe pain and swelling the more you do the more it hurts Ligament injuries are like walking on ice DOES IT HURT AND GIVE OUT OR GIVEOUT AND HURT? Often minor trauma in adults due to degeneration, sometimes feel a pop Feel a click plus or minus effusion (popliteal) Joint line tenderness pain with rotation (McMurray, Appley, etc) Pain and swelling with activity, low grade Usually surgical or live with it Meniscus relatively inert and poor healing potential Outpatient procedure, arthroscopic, 2 to 4 weeks return to many sports if motivated Not a surgical emergency, difficult to play through “Repair” usually means taking out torn portion Only 10% repairable (bucket and vertical tears in outer 1/3) NFL meniscal injuries more career ending than ACL Most common in sports particularly with acceleration/deceleration Not always a violent injury many noncontact Classic is feel a pop followed by intense swelling within 6 hours (hemarthrosis) Not a surgical emergency Surgery often delayed 3 or more weeks (reconstruction) May have effusion may not some walk in comfortable Lachman’s test is most classic and STILL most useful Often missed on MRI (femoral detachment difficult to pick up) Not always surgical initial RICE and ROM PT for quad hamstring strengthening Brace treatment Coping and sport modification Surgery Reconstruction with multiple graft choices Who gets it? – under 40, women, buckling with daily activity, competitive level 1 sports Outpatient surgery mostly arthroscopic return to full sport variable but 6months to one year More rare usually in the realm of orthopedist Not a “Pulled muscle” Many are not surgical but require detailed diagnosis (combined injuries) Not emergency but protection with crutches and immobilizer needed Bones now important Physeal injuries common (weaker than ligaments and cartilage) Different age leads to different fractures ie tibial eminence 12yrs tibial tubercal 14yrs ACL eqivalent in younger age Same mechanism of injury May require surgery usually requires referral Typically occur during adolescence 3 types depending on severity Only most severe (type 3) require surgery but all require referral Common in younger kids Represents an avulsion of inferior patellar cartilage from bone Analogous to patellar tendon rupture in adults Can be difficult to diagnose (pain, fear etc) Usually occur during adolescence Three types depending on severity Only type 3 requires surgery but all require referral for treatment History and physical still the key as imaging is confirmatory. Most injuries not a “pulled muscle” Relax most are not surgical emergencies Pediatric injuries tend to be physeal and more emergent